Burkholderia cepacia Complex Producing a Peculiar Violet Pigment: A Case Series From a Tertiary Care Hospital in Meghalaya
Kunjjal Shah, Mercy Ngairangbam, Neeta Gogoi, Papia Chakraborty, W Valarie Lyngdoh

TL;DR
This paper reports cases of BCC infections at a hospital in Meghalaya, where the bacteria produced a rare violet pigment.
Contribution
The study highlights a unique violet pigment-producing BCC isolate in clinical cases from a specific region.
Findings
BCC isolates were found to produce a violet pigment, a rare characteristic.
The isolates were associated with bacteremia in clinical cases.
The pigment production may have implications for identification and clinical management.
Abstract
The Burkholderia cepacia complex (BCC) represents a group of bacteria that are gram-negative, aerobic, and non-fermenters. They are notorious for causing infections in vulnerable individuals, such as those with compromised immune systems. Examples are patients suffering from cystic fibrosis or chronic granulomatous disease. These bacteria are prevalent in diverse habitats, like soil and water. Over the last four decades, they have gained recognition as both emerging opportunistic pathogens and nosocomial threats. Managing BCC infections poses significant challenges due to their inherent resistance to numerous antibiotics, thus raising substantial concerns within clinical settings. Here, we present a case series of bacteremia, with BCC as the causative organism. The isolates showed a curious phenomenon of producing a violet pigment.
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
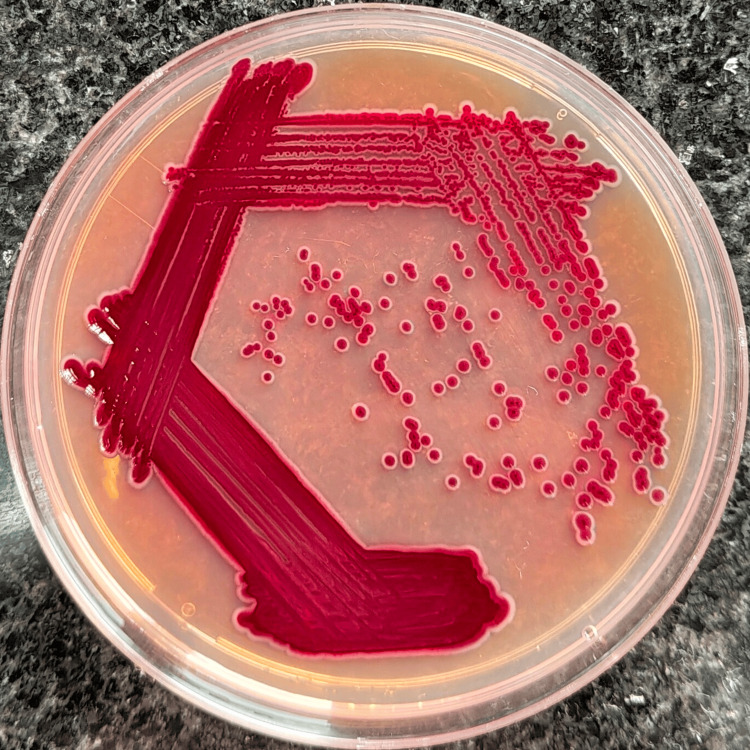 Figure 1
Figure 1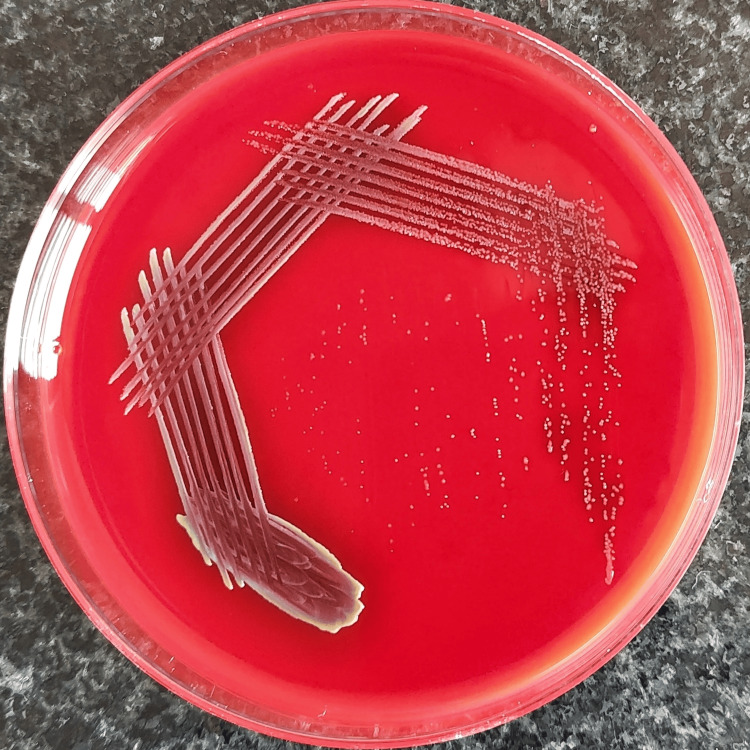 Figure 2
Figure 2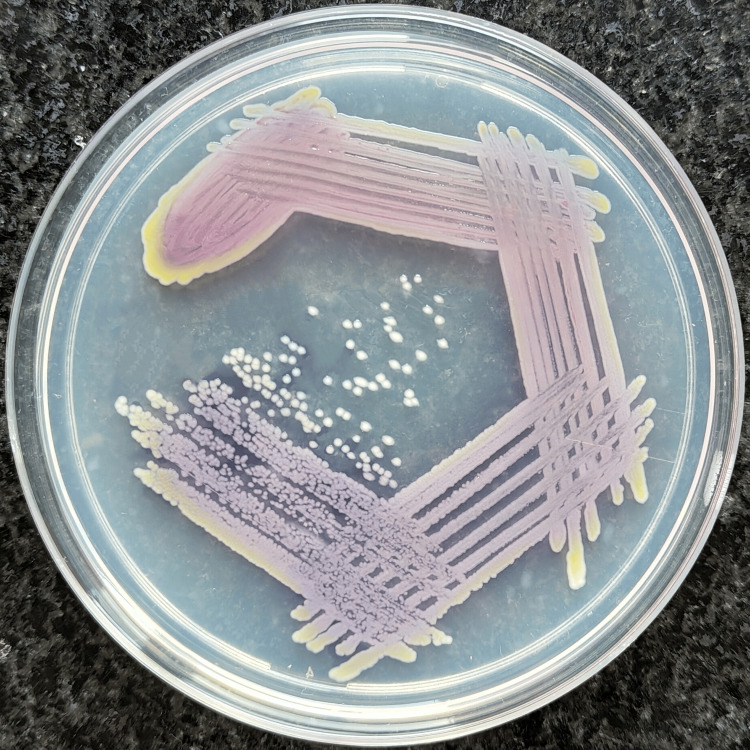 Figure 3
Figure 3| Sl. no. | Age/sex | Ward/ICU | Relevant clinical history | Indwelling device | Diagnosis | Surgical intervention |
| 1 | 56/F | MICU | History of fever seven days after surgery, known case of diabetes mellitus (not on medication) and hypertension | Central venous catheter, Foley's catheter | Diabetic ketoacidosis with uncontrolled type 2 diabetes mellitus, dry gangrene of left foot, hypertension, mild aortic regurgitation, bilateral pleural effusion, septic shock, severe anemia | Above knee amputation of left lower limb |
| 2 | 18/M | Male Surgery Ward | History of fever three days after surgery, no history of diabetes mellitus, hypertension, or tuberculosis | Foley's catheter, abdominal drain | Gastric outlet obstruction | Laparoscopic truncal vagotomy + loop gastrojejunostomy under general anesthesia |
| 3 | 38/M | Urology Ward | History of fever one hour after surgery, no history of diabetes mellitus, hypertension, or tuberculosis | PCN catheter | Left renal staghorn calculus | Left percutaneous nephrolithotomy under spinal anesthesia |
| 4 | 70/F | MICU | Shortness of breath, coughing on lying down, known case of diabetes mellitus and hypertension | Foley's catheter | Coronary artery disease, uncontrolled type 2 diabetes mellitus, lower respiratory tract infection, hyperosmolar hyperglycemic syndrome, septic shock, acquired cystic kidney disease | None |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsVibrio bacteria research studies · Bacterial biofilms and quorum sensing · Cystic Fibrosis Research Advances
Introduction
Burkholderia cepacia complex (BCC) is a concerning group of bacilli, characteristically aerobic, gram-negative, non-fermenters, gaining notoriety for causing infections in individuals with compromised immune systems. Examples are patients suffering from cystic fibrosis (CF) or chronic granulomatous disease. These bacteria are found widely in diverse habitats, including soil and water. They have been recognized as emerging opportunistic as well as nosocomial pathogens over the past four decades. Infections with BCC can be challenging to treat owing to their intrinsic resistance to many antibiotics, making them a significant concern in clinical settings [1].
Here, we present a report on four cases of bacteremia, with the causative organism being BCC. The isolates displayed a peculiar phenotypic characteristic of violet-pigmented colonies. Reports of this unique pigmentation in BCC are rare. However, such knowledge can contribute to the identification of non-fermenters being more comprehensive, particularly in resource-limited settings.
Case presentation
We have recorded four cases of bacteremia caused by BCC. For each patient, we collected the relevant clinical history along with their demographic profile, including their age and sex. We also looked into whether any invasive interventions were performed for each patient. The collected data has been compiled and presented in Table 1.
Paired blood samples were sent in automated blood culture bottles the same day a high temperature was recorded for each patient. Subsequently, on receipt of each sample, they were incubated in the BacT/ALERT 3D. Each sample was flagged positive, followed by their inoculation onto MacConkey agar, blood agar, and chocolate agar. Overnight aerobic incubation of the plates was done at a temperature of 37℃. The isolates that grew on culture were then identified with the VITEK® 2 system, which also determined the minimum inhibitory concentration (MIC) values for the organisms. The antimicrobial susceptibility profile was reported by interpreting the MIC values using the Clinical and Laboratory Standards Institute (CLSI) Guidelines, 2024.
The blood cultures showed growth of gram-negative bacilli, which appeared as 1-2 mm, violet-pigmented colonies on MacConkey agar (Figure 1), while 5% sheep blood agar showed growth of 0.5 mm, black to burgundy colonies with diffusible pigment of similar hue and the margins of the well showed yellow pigmentation (Figure 2). On nutrient agar, 1-1.5 mm colonies with a light violet pigment were seen, and the margins of the well showed a yellow pigmentation (Figure 3). Conventional biochemical tests revealed the organism to be catalase-positive, delayed oxidase-positive, lactose non-fermenting, and motile. Subsequent automated bacterial identification was done with the VITEK® 2 system, which established the organism as BCC. The VITEK® 2 system calculated the antibiotic susceptibility profile for the organism and interpreted it by the CLSI Guidelines, 2024. All four isolates were found to share a similar antibiotic susceptibility pattern, exhibiting sensitivity to ceftazidime, minocycline, levofloxacin, trimethoprim/sulfamethoxazole, and meropenem.
The blood cultures of the respective four cases were interspersed by weeks to months. The patients were started on levofloxacin. On completion of the antibiotic course, the BCC bacteremia was cleared, as evidenced by subsequent blood cultures.
Colonies of BCC on MacConkey agar showing a violet pigmentation.BCC: Burkholderia cepacia complex.
Colonies of BCC on blood agar showing black to burgundy pigmentation.BCC: Burkholderia cepacia complex.
Colonies of BCC on nutrient agar showing a light violet pigmentation.BCC: Burkholderia cepacia complex.
Discussion
The BCC comprises bacteria that share similar characteristics phenotypically but differ genetically. All members of this complex are aerobic gram-negative bacilli equipped with multiple polar flagella, granting them motility. The BCC presently comprises 22 closely related species [2]. Initially identified by Burkholder in 1940 as a cause of onion rot, the BCC demonstrates the potential for beneficial interactions with plant hosts and may serve as a valuable asset in bioremediation and as a plant-growth enhancer, partly owing to its capability of synthesizing anti-fungal agents [3-5].
In individuals with cystic fibrosis (CF), the BCC contributes to heightened mortality and morbidity, decreased lung function, and pro-inflammatory damage [6]. Typically, there are instances featuring rapid and severe pneumonic infection accompanied by fever and respiratory failure, sometimes coupled with bloodstream infection, which are referred to as "cepacia syndrome" [7].
Additionally, BCC is gaining notoriety as a nosocomial pathogen. Its capability to contaminate medical apparatus and objects, such as ultrasound gel and chlorhexidine wipes, has increasingly come to light in recent years [8-10]. Owing to its capacity to flourish in diverse habitats, BCC leads to immense mortality and morbidity among hospitalized patients. Instances of septicemia caused by BCC occur in hospitalized patients across various settings, including those who are immunocompetent or immunosuppressed, as well as in intensive care units (ICUs) and oncology units [11]. The presented cases had developed bacteremia after more than 48 hours of hospital stay, pointing to BCC being a nosocomial pathogen in these patients. In this case series, two out of four patients were in the ICU when their cultures were sent. It was also noted that three of the four cases had undergone surgical interventions, and blood cultures were dispatched during their respective episodes of fever in the postoperative period. These cultures flagged positive, suggesting the need to further investigate the source of infection, with a special focus on the operation theaters and ICUs.
The BCC demonstrates intrinsic resistance to numerous commonly employed antibiotics, including antipseudomonal penicillins (such as piperacillin, carbenicillin, and ticarcillin), aminoglycosides, polymyxins, and first- and second-generation cephalosporins [1]. These antimicrobial agents are frequently utilized in treating Pseudomonas infections, underscoring the significance of accurately distinguishing between BCC and Pseudomonas. BCC is known to display increasing drug resistance, which, however, was seen less significantly in these reported cases as the isolates showed sensitivity to ceftazidime, minocycline, levofloxacin, trimethoprim/sulfamethoxazole, and meropenem.
The isolates showed colonies having a violet pigment, which is a peculiar feature displayed by BCC. Other studies done by De et al. [12], Ranjan et al. [13], and Rastogi et al. [14] emphasize a similar phenotypical attribute of violet pigment production of BCC that they encountered. The knowledge of such peculiarities in BCC can help broaden the approach to the identification of non-fermenters, especially in resource-limited settings.
Deeper and more extensive research needs to be conducted in order to find the root cause of such phenotypical and genotypical diversity among the members of the BCC.
Conclusions
The BCC is commonly known to be a nosocomial pathogen. We have recorded four cases where the BCC has caused hospital-acquired infection. Out of these cases, three patients shared the commonality of having surgical procedures done in the hospital. Also, out of the four patients, two had been admitted in critical care units. Rigorous surveillance and good infection prevention and control practices will aid in the prevention of nosocomial infections.
The BCC isolates from this case series displayed a rare occurrence of a violet pigment produced by these organisms. A few other studies showing similar findings warrant the need for further research into finding the root cause of such phenotypic and genotypic diversity among the BCC. The knowledge of such peculiarities in BCC is important. It can contribute to a more comprehensive approach in the identification of non-fermenters, particularly in resource-limited settings.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Burkholderia cepacia complex: beyond pseudomonas and acinetobacter Indian J Med Microbiol Gautam V Singhal L Ray P 4122920112130418710.4103/0255-0857.76516 · doi ↗ · pubmed ↗
- 2Accurate identification and epidemiological characterization of Burkholderia cepacia complex: an update Ann Clin Microbiol Antimicrob Devanga Ragupathi NK Veeraraghavan B 71820193071779810.1186/s 12941-019-0306-0PMC 6360774 · doi ↗ · pubmed ↗
- 3The various lifestyles of the Burkholderia cepacia complex species: a tribute to adaptation Environ Microbiol Vial L Chapalain A Groleau MC Déziel E 1121320112088009510.1111/j.1462-2920.2010.02343.x · doi ↗ · pubmed ↗
- 4Time to revisit polyphasic taxonomy Antonie Van Leeuwenhoek Vandamme P Peeters C 576510620142463391310.1007/s 10482-014-0148-x · doi ↗ · pubmed ↗
- 5Diversity of the Burkholderia cepacia complex and implications for risk assessment of biological control strains Annu Rev Phytopathol Parke JL Gurian-Sherman D 2252583920011170186510.1146/annurev.phyto.39.1.225 · doi ↗ · pubmed ↗
- 6Host evasion by Burkholderia cenocepacia Front Cell Infect Microbiol Ganesan S Sajjan US 25120112291959010.3389/fcimb.2011.00025 PMC 3417383 · doi ↗ · pubmed ↗
- 7Burkholderia cenocepacia and Burkholderia multivorans: influence on survival in cystic fibrosis Thorax Jones AM Dodd ME Govan JR Barcus V Doherty CJ Morris J Webb AK 9489515920041551646910.1136/thx.2003.017210 PMC 1746874 · doi ↗ · pubmed ↗
- 8An outbreak of Burkholderia cepacia complex pseudobacteremia associated with intrinsically contaminated commercial 0.5% chlorhexidine solution Am J Infect Control Ko S An HS Bang JH Park SW 2662684320152555777010.1016/j.ajic.2014.11.010 · doi ↗ · pubmed ↗