Cytomegalovirus Infection of the Gastrointestinal Tract in Patients on Hemodialysis: A Case Report and Literature Review
Toshiyuki Nakanishi, Kazuhiro Ishikawa, Yusuke Ohashi, Takuya Fujimaru, Mori Nobuyoshi

TL;DR
A case report and literature review show that cytomegalovirus can cause gastrointestinal issues in hemodialysis patients, requiring early detection and treatment.
Contribution
This paper adds a new case of CMV colitis in a hemodialysis patient and reviews existing literature on the topic.
Findings
CMV infection in the GI tract was diagnosed in a hemodialysis patient through biopsy and treated successfully with valganciclovir.
A literature review identified 24 cases of CMV GI tract infections in dialysis patients, with symptoms like hematochezia and diarrhea.
Clinicians should consider CMV infection in dialysis patients with unexplained bloody diarrhea and perform endoscopy and biopsy promptly.
Abstract
Cytomegalovirus (CMV) infection is widespread in immunocompromised people, and several cases of CMV infections of the gastrointestinal (GI) tract have been reported in these individuals. We present a case of an immunocompetent patient on hemodialysis (HD) who developed CMV colitis. We also conducted a review of the literature on CMV GI tract infections among patients with chronic kidney disease undergoing dialysis. A 46-year-old man with a history of end-stage renal disease and undergoing HD developed severe diarrhea and hematochezia. A colonoscopy revealed ulcers, and CMV infection was identified in the biopsy sample. We successfully treated the patient with valganciclovir for 2 months. Our review of the literature yielded 21 articles and 24 cases of CMV GI tract infection in patients undergoing dialysis, including the current case. Hematochezia and diarrhea were purported to serve as…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
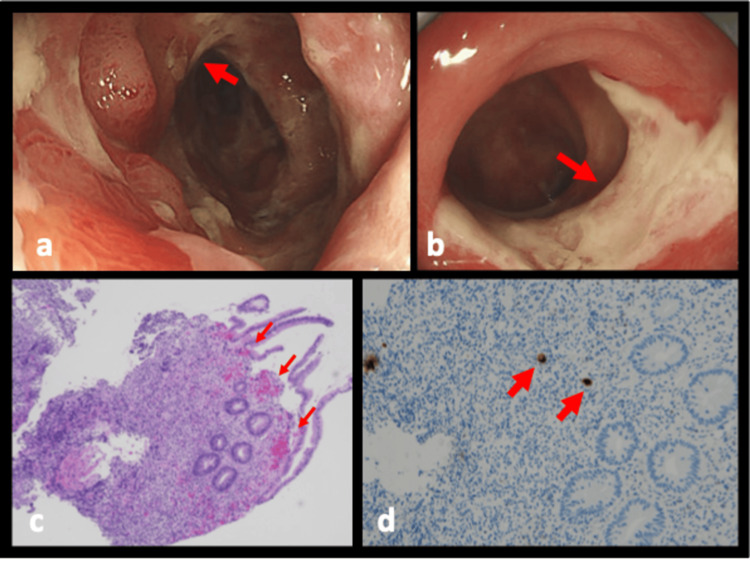 Figure 1
Figure 1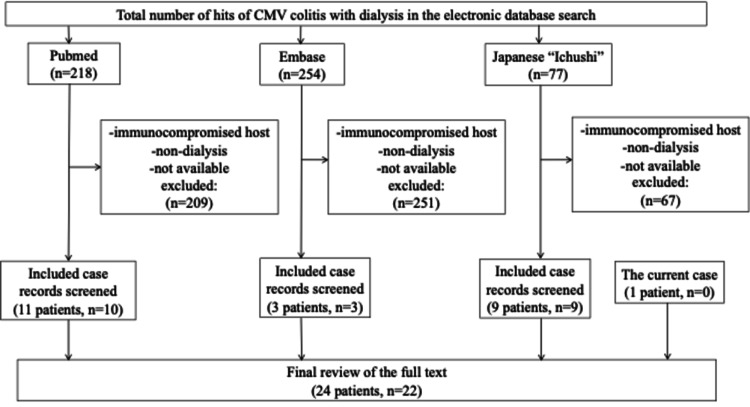 Figure 2
Figure 2| Test | Reference range | Results |
| White blood cells | 4.0-10 x 103/μL | 12.8 |
| Neutrophils | 40-70% | 85 |
| Lymphocytes | 20-45% | 9 |
| Monocytes | 5.0-12% | 6 |
| Hemoglobin | 12.0-17.0 x g/dL | 13.3 |
| Hematocrit | 40.0-51.0% | 43.2 |
| Platelets | 150-400 x 103/μL | 216 |
| Sodium | 136-146 mmol/L | 134 |
| Potassium | 3.50-5.10 mmol/L | 4.7 |
| Chloride | 98-106 mmol/L | 99 |
| Urea | 2.5-6.6 mmol/L | 29.9 |
| Creatinine | 72-127 μmol/L | 744 |
| ALT | <40 U/L | 8 |
| AST | <42 U/L | 9 |
| Bilirubin | <17 μmol/L | 0.5 |
| GGTP | 7-50 U/L | 33 |
| Albumin | 35-52 g/L | 29 |
| C-reactive protein | <5 mg/L | 247 |
| Case No | Author | Age (years) | Sex | Type of dialysis | Dialysis vintage (months) | Underlying diseases | Chief complains | Time lag from developing symptoms to the diagnosis (days) | Diagnostic method | Infected sites | WBC (×109/L) | CRP (mg/dL) | Hb (g/dL) | Complications | Antiviral therapy (+/-) | Therapeutic duration (weeks) | Outcome | Recurrence (+/-) |
| 1 | Esforzado et al. (1993) [ | 74 | Male | HD | 1 | DM, gastric ulcer | Hematochezia* | Biopsy | Colon | 20.5 (Ly 11%) | (+: GCV) | 3 | Survived | |||||
| 2 | Esforzado et al.(1993) [ | 59 | Female | HD | 24 | DM, right food distal amputation due to peripheral vascular disease | Hematochezia, fever, abdominal pain, diarrhea | Biopsy | Colon | 18.1 | (+) | Survived | (-) | |||||
| 3 | Falagas et al. (1996) [ | 57 | Male | HD | 6 | ADPKD, HTN, nephrolithiasis, asthma, gout, HBV career | Hematochezia, abdominal pain, diarrhea | Biopsy | Colon | 10.8 (Ly 7%) | 11.5 | Hemicolectomy | (+: GCV) | 2 | Survived | (-) | ||
| 4 | Liu et al. (2018) [ | 77 | Female | HD | Type 2 DM, HTN, atrial fibrillation, congestive heart failure | Loss of appetite, nausea, epigastric pain | Biopsy | Stomach | 5.3 | 1.9 | 6.2 | (+: VGCV) | 2 | Survived | ||||
| 5 | Kim et al. (2011) [ | 56 | Male | HD | 24 | Type 2 DM | Watery diarrhea, abdominal pain | 14 | Biopsy | Colon | 13.2 | 30 | 9.1 | (+: GCV) | 4 | Survived | ||
| 6 | Rankin et al. (2009) [ | 72 | Male | HD | COPD, type 2 DM, cardiovascular disease | Hematochezia | Biopsy | Colon | 20.2 | 42 | 9.5 | (+: GCV) | 3 | Survived | ||||
| 7 | Sudcharoen et al. (2016) [ | 72 | Male | HD | Ischemic heart disease, cerebrovascular disease, HTN, gout | Hematochezia | 56 | Biopsy | Colon | (+: GCV) | 1 | |||||||
| 8 | Tabernero et al. (2004) [ | 72 | Male | HD | 36 | Renal tuberculosis | Fever, hematochezia, abdominal pain | 21 | Biopsy | Colon | 2.7 | 9.5 | (+: GCV) | 3 | Survived | |||
| 9 | Hsieh et al. (2015) [ | 59 | Female | PD | 60 | Fever, abdominal pain | 85 | Biopsy | Colon | 17.5 | (+: GCV) | 3 | Survived | |||||
| 10 | Huang et al. (2017) [ | 44 | Male | HD | DM | Hematochezia, shock, abdominal pain, fever | 13 | Biopsy | Colon | Right-colon ischemia with pneumatosis intestinalis, hemicolectomy | (+: GCV) | 12 | Survived | |||||
| 11 | Quintana et al. (2005) [ | 65 | Male | PD | 72 | Type 2 DM, chronic neurovascular complications | Vomiting, dysphagia | 29 | Biopsy | Esophagitis | (+: GCV) | 2 | Survived | |||||
| 12 | Lo (2017) [ | 70 | Female | HD | 70 | Coronary artery disease | Hematemesis | Gastric fluid | Stomach | Hyperkalemia, atrial flutter | (+: GCV → VGCV) | |||||||
| 13 | Yap et al. (2016) [ | 52 | Male | HD | HTN | Hematochezia, abdominal pain | Biopsy | Small intestine | 5.0 | (+: GCV) | ||||||||
| 14 | Li et al. (2015) [ | 83 | Female | HD | DM | Hematochezia | (+: GCV) | Survived | ||||||||||
| 15 | Isekawa et al. (2013) [ | 76 | Female | HD | 144 | DM | Hematochezia, diarrhea | Biopsy | Colon | (+: GCV) | 4 | Survived | ||||||
| 16 | Imoto et al. (2010) [ | 65 | Male | HD | 72 | Chronic nephritis, AA amyloidosis | Abdominal pain, diarrhea | Biopsy | Colon | (+: GCV) | Died | |||||||
| 17 | Okada et al. (2012) [ | 72 | Female | HD | 36 | DM | Abdominal pain | Biopsy | Colon | 16.1 | 9.7 | 15.6 | Necrosis of the intestine, colectomy, colostomy | (-) | Survived | |||
| 18 | Asai et al.(2009) [ | 76 | Male | HD | 144 | Chronic glomerulonephritis, CABG, PAF, cervical spondylotic myelopathy | Fever, abdominal pain, diarrhea | Biopsy | Colon | (+: GCV) | Survived | |||||||
| 19 | Bando et al. (2008) [ | 72 | Male | HD | 216 | Renal sclerosis | Fever, abdominal pain | 38 | Biopsy | Colon | 22 | Fungal abscess of the iliopsoas muscle | (+: GCV) | Survived | ||||
| 20 | Miyauchi et al. (2006) [ | 74 | Male | HD | 1 | Gastric cancer, prostatic cancer, empyema, lung aspergillosis | Vomiting, hematemesis | 28 | Biopsy | Esophagus | 15.8 | 7.7 | 3.85 | (+: GCV, stopped due to pancytopenia) | Died | |||
| 21 | Sasaki et al. (2004) [ | 68 | Female | HD | 60 | Tuberculosis pleurisy | Abdominal pain | 84 | Biopsy | Duodenum | 7.1 | 7.9 | 8.7 | (+: GCV) | Survived | |||
| 22 | Nishimoto et al. (2002) [ | 57 | Female | PD | 48 | Cholecystectomy, acute pyelonephritis | Watery diarrhea, vomiting | Biopsy | Colon, esophagus, stomach | 13.4 | 5.4 | AA amyloidosis | (+: GCV) | 5.6 | Died | |||
| 23 | Dayasu et al. (1999) [ | 63 | Male | HD | 12 | Hematochezia | 37 | Biopsy | Colon | (+: GCV) | Died | |||||||
| 24 | The present case | 46 | Male | HD | 108 | DM, shunted stenosis | Diarrhea, hematochezia | 11 | Biopsy | Colon | 14.6 | 2.4 | 12.7 | (+: VGCV) | 8 | Survived | (-) |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsCytomegalovirus and herpesvirus research · Pneumocystis jirovecii pneumonia detection and treatment · Herpesvirus Infections and Treatments
Introduction
Cytomegalovirus (CMV) infection is common in immunosuppressed individuals. However, CMV reactivation can sometimes occur without immunosuppression, with blood transfusion being a risk factor for developing CMV infection among immunocompetent patients [1,2]. Although CMV can put several organ systems at risk, the gastrointestinal (GI) tract is affected most frequently in immunocompetent patients [3]. A retrospective cohort study reported that chronic kidney disease (CKD) increases the risk of CMV enteritis [4], while another revealed that even in CKD patients without the presence of overt immunodeficiency, the GI tract is the most common site of involvement [5]. Furthermore, a retrospective cohort study found that the majority of immunocompetent individuals with GI CMV disease had CKD of stage III or more and that this was significantly more common in immunocompetent rather than immunocompromised patients (62.9 vs. 24.2%, P<0.001) [6], and a literature review of 44 immunocompetent patients with CMV colitis found eight of these patients had renal failure, which was considered one of the comorbidities affecting immune function [7].
Thus, a relationship likely exists between CMV reactivation in the GI tract and CKD, particularly in the dialytic state. Here, we present a case of CMV colitis in an immunocompetent patient undergoing hemodialysis (HD) with end-stage renal disease (ESRD). We also performed a literature review and identified the characteristics of GI tract infections with CMV among patients with ESRD receiving HD or peritoneal dialysis.
Case presentation
A 46-year-old man with a 9-year history of ESRD, being treated with HD was transferred to our emergency department with complaints of diarrhea and hematochezia. One week before the transfer, he was hospitalized for 4 days with watery diarrhea. During admission, the patient was receiving levofloxacin (500 mg every 48 h) and ceftriaxone (1 g every 24 h) for the possible diagnosis of bacterial gastroenteritis. He stated he had not eaten raw poultry or eggs or traveled abroad recently, and had no history of HIV infection or blood transfusion. His ESRD was due to diabetic kidney disease. The patient was hypotensive upon admission, and a physical examination revealed tenderness in the lower middle abdomen. Laboratory tests showed elevated white blood cell (WBC) count, low hemoglobin, and elevated levels of C-reactive protein (CRP) and creatinine (Table 1). Although differential diagnosis included Campylobacter, Salmonella, and Clostridioides difficile (CD) infection, stool culture did not reveal any pathogenic bacteria, and CD toxin A/B or glutamate dehydrogenase was negative. A colonoscopy revealed erosions and small ulcers around the hepatic flexure (Figure 1a). A tissue biopsy was performed, and immunohistochemical analysis detected CMV-positive cells (Figures 1c-1d). On this basis, the patient was diagnosed with CMV colitis. There were no obvious findings on physical examination suggesting the other CMV direct effects, such as retinitis, ventriculitis, and pneumonia. We administered oral valganciclovir (VGCV, 225 mg) three times a week, and the watery diarrhea decreased. A follow-up colonoscopy was performed a month after treatment initiation. There were still multiple ulcers in the colon (Figure 1b), although the repeat biopsy was CMV-negative. Blood investigation showed normalized WBC count and CRP. He was treated with oral VGCV for 8 weeks. There were no signs of relapse at the 3-month follow-up.
Colonoscopy imagesInitial colonoscopy (upon admission) (a) reveals erosions and small well-defined ulcers (arrow), consistent with CMV colitis. The follow-up colonoscopy (b) identified scarring and a healed ulcer (arrow). Hematoxylin-eosin staining (×4, c) revealed inflammation of the colon (arrow) , and immunohistochemical staining (×10, d) detected CMV-positive intranuclear inclusions (arrow).CMV: cytomegalovirus
Discussion
We performed a literature review, the strategy for which is presented in Figure 2. The clinical characteristics of 24 patients, including our patient, are shown in Table 2 [8-29]. The median age of the patients was 68 years with 62.5% men. In 78.2% of patients, the colon was the primary infected GI site. The median period since dialysis began (dialysis vintage) was 48 months. The main symptoms of CMV gastroenterocolitis were abdominal/epigastric pain (54.1%), hematochezia (50.0%), and diarrhea (33.3%). The median time delay from symptom onset to definitive biopsy was 29 days. Of the 24 patients, one was excluded because of missing data. Twenty patients were treated with ganciclovir (GCV), two received VGCV, and one required a switch from GCV to VGCV. In one of the 20 GCV-treated patients, administration was interrupted because of pancytopenia. Regarding the prognosis, as mentioned during the follow-up period, the mortality rate was 18.1%.
Flowchart of the literature review process.Three authors (T.N., I.K., and Y.O.) independently reviewed the relevant titles and abstracts in the database records, retrieved full texts for eligibility assessment, and extracted information from these cases. We performed a search using the keywords “cytomegalovirus,” “CMV,” “esophagitis,” “gastritis,” “colitis,” “enterocolitis,” “gastroenteritis,” “renal dialysis,” “hemodialysis,” “hemodialysis,” “dialysis,” “chronic,” “kidney,” “renal,” and “nephron” in the electronic databases PubMed, Embase, and Ichushi from inception until May 31, 2022. We excluded immunocompromised patients with HIV infection, recipients of solid organ or hematopoietic stem cell transplantation, those receiving immunosuppression therapy, and those who had not been treated with dialysis before CMV infection. A total of 22 articles and 24 cases of GI CMV infection among dialysis patients were included.CMV: cytomegalovirus; HIV: human immunodeficiency virus; GI: gastrointestinal
Our study supports the hypothesis that dialysis in patients with ESRD is a risk factor for CMV infection. One case-control study did not identify renal disease requiring HD as an independent risk factor for CMV colitis in immunocompetent patients (odds ratio: 1.72, 95% CI: 0.24-12.22, P-value: 0.58) but suggested that red blood cell transfusion within 1 month of diagnosis of colitis was a risk factor [1]. This could explain why dialysis patients receiving frequent transfusions have a higher CMV infection risk. As mentioned previously, another retrospective cohort study identified CKD as a risk factor for CMV enteritis [4]. More specifically, CKD and ESRD led to dendritic cell depletion and dysfunction, reduced CD4/CD8 ratio, increased Th1/Th2 ratio, and depleted naïve and central memory CD4+ and CD8+ T cells [30]. Therefore, it remains controversial whether CMV infection of the GI tract is correlated with dialysis. Our literature review was unable to reveal the detailed history of previous blood transfusion or CD4/CD8 ratio among dialysis patients and prompts further prospective studies.
Furthermore, one retrospective cohort study on GI tract CMV disease showed that the most frequent sites of infection among 89 immunocompetent patients were the colon and rectum (66.3%), followed by the esophagus (5.6%), stomach (4.5%), and small intestine (19.1%) [6]. These results are similar to those of our review. Another literature review of CMV colitis in immunocompetent patients without chronic renal failure [31], reported that the most common presenting symptoms were fever (76%), abdominal or rectal pain (53%), hematochezia (53%), and watery diarrhea (29%). In our study, the symptoms observed in dialysis patients with CMV infection were consistent with these two studies. Additionally, our review revealed that CMV gastroenterocolitis often affects the colon and is accompanied by hematochezia or watery diarrhea. Since CMV diagnosis should be confirmed by a colon biopsy, our findings suggest that if dialysis patients present with hematochezia or watery diarrhea, a colonoscopy should be performed.
Regarding treatment, although low creatinine clearance (<20 mL/min) was reported to be a risk factor for GCV-induced thrombocytopenia [32], the cessation of GCV or VGCV treatment due to thrombocytopenia was not observed in our review, except for one patient with pancytopenia. Therefore, HD-dependent CKD may not increase the incidence of thrombocytopenia and further studies are required to evaluate adverse events associated with GCV or VGCV use in HD patients.
In our review, the median time delay from symptom onset to a definitive biopsy was 29 days, which could be attributed to several reasons. First, CMV enterocolitis is often self-limiting [33,34], and patients can be cured before being diagnosed. Second, it is uncommon for clinicians to suspect CMV infection in immunocompetent patients. Finally, clinicians may not perform a biopsy of a suspicious lesion in some cases, preventing CMV detection at an earlier stage.
A limitation of our study is that the literature review methodology can have reporting bias, lack of generalizability, and a large amount of missing data. Thus, prospective studies are required to confirm the relationship between ESRD with HD and CMV infections of the GI tract in the future.
Conclusions
To our knowledge, this is the first literature review on CMV infections of the GI tract in patients on HD. Hematochezia and diarrhea were observed as the likely symptoms that increase the pretest probability of CMV reactivation in the GI tract among HD patients. Our analysis suggests that clinicians should suspect CMV infection of the GI tract in dialysis patients, who experience unexplained bloody diarrhea, and promptly perform GI endoscopy and biopsy.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Clinical presentation and risk factors for cytomegalovirus colitis in immunocompetent adult patients Clin Infect Dis Ko JH Peck KR Lee WJ 0660201510.1093/cid/ciu 96925452594 · doi ↗ · pubmed ↗
- 2Cytomegalovirus infection in immunocompetent critically ill adults: Literature review Ann Intensive Care Al-Omari A Aljamaan F Alhazzani W Salih S Arabi Y 110620162781302410.1186/s 13613-016-0207-8PMC 5095093 · doi ↗ · pubmed ↗
- 3Severe cytomegalovirus infection in apparently immunocompetent patients: A systematic review Virol J Rafailidis PI Mourtzoukou EG Varbobitis IC Falagas ME 47520081837122910.1186/1743-422X-5-47PMC 2289809 · doi ↗ · pubmed ↗
- 4Clinical manifestations, risk factors, and prognostic factors of cytomegalovirus enteritis Gut Pathog Yeh PJ Chiu CT Lai MW 531320213440787910.1186/s 13099-021-00450-4PMC 8371416 · doi ↗ · pubmed ↗
- 5Cytomegalovirus disease in nonimmunocompromised, human immunodeficiency virus-negative adults with chronic kidney disease J Microbiol Immunol Infect Chen YM Hung YP Huang CF 3453494720142348140810.1016/j.jmii.2013.01.011 · doi ↗ · pubmed ↗
- 6Clinical features, endoscopic findings, and predictive factors for mortality in tissue-invasive gastrointestinal cytomegalovirus disease between immunocompetent and immunocompromised patients Gastroenterol Res Pract Wetwittayakhlang P Rujeerapaiboon N Wetwittayakhlung P 1112021202110.1155/2021/8886525 PMC 805215533897776 · doi ↗ · pubmed ↗
- 7Meta-analysis of outcome of cytomegalovirus colitis in immunocompetent hosts Dig Dis Sci Galiatsatos P Shrier I Lamoureux E Szilagyi A 6096165020051584468910.1007/s 10620-005-2544-6 · doi ↗ · pubmed ↗
- 8Cytomegalovirus colitis in chronic renal failure Clin Nephrol Esforzado N Poch E Almirall J BombíJA López-Pedret J Revert L 275278391993 https://pubmed.ncbi.nlm.nih.gov/8390337/8390337 · pubmed ↗