Perinatal outcome in anti-NMDAr encephalitis during pregnancy—a systematic review with individual patients’ data analysis
Giovanna Scorrano, Fedele Dono, Clarissa Corniello, Stefano Consoli, Giacomo Evangelista, Armando Di Ludovico, Francesco Chiarelli, Francesca Anzellotti, Angelo Di Iorio, Stefano L. Sensi

TL;DR
This study reviews the outcomes of pregnancies affected by anti-NMDAr encephalitis, highlighting risks to both mothers and fetuses and the impact on child neurodevelopment.
Contribution
The study provides a systematic analysis of individual patient data to clarify perinatal outcomes in anti-NMDAr encephalitis during pregnancy.
Findings
Pregnant women with anti-NMDAr encephalitis experienced spontaneous pregnancy loss, premature birth, and cesarean delivery.
Fetal and neonatal complications were linked to maternal anti-NR1 antibody levels, including movement disorders and low birth weight.
Neuropsychiatric issues in children were associated with pathogenic NMDAr antibodies in maternal or neonatal serum.
Abstract
Anti-N-methyl-D-aspartate receptor (NMDAr) antibody encephalitis is an autoimmune disorder characterized by synaptic NMDAr current disruption and receptor hypofunction, often affecting women during pregnancy. Clinical manifestations associated with anti-NMDAr encephalitis can occur both in the mother and fetus. We generated a systematic search of the literature to identify epidemiological, clinical, and serological data related to pregnant women with anti-NMDAr encephalitis and their children, analyzing the fetal outcomes. We examined the age and neurologic symptoms of the mothers, the presence of an underlying tumor, immunotherapies used during pregnancy, duration of the pregnancy, and type of delivery. Data from 41 patients were extrapolated from the included studies. Spontaneous interruption of pregnancy, premature birth, and cesarean section were reported in pregnant women with…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
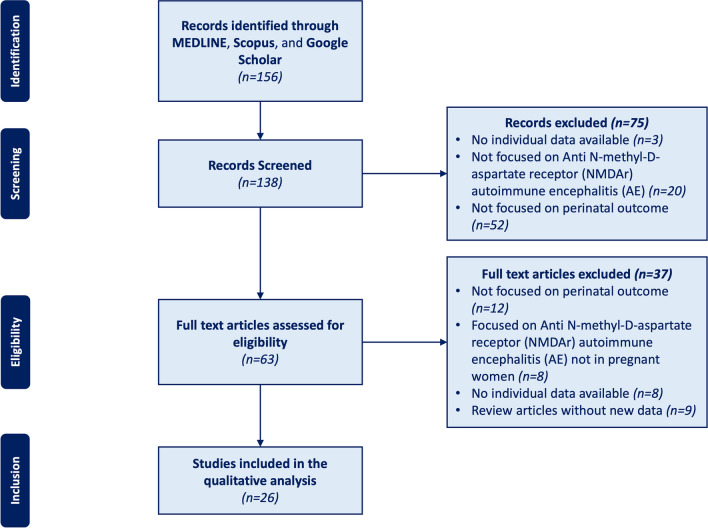 Figure 1
Figure 1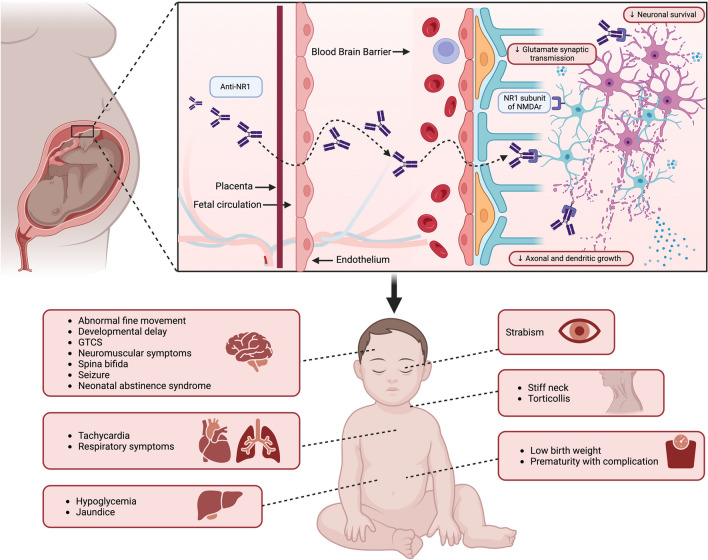 Figure 2
Figure 2- —Università degli Studi G. D'Annunzio Chieti Pescara
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsAutoimmune Neurological Disorders and Treatments · Genetics and Neurodevelopmental Disorders · Adenosine and Purinergic Signaling
Introduction
Anti-N-methyl-D-aspartate receptor (NMDAr) autoimmune encephalitis (AE) is one of the most common causes of noninfectious encephalitis during pregnancy [1–3]. It is characterized by an autoimmune response against the NR1 subunit of NMDAr, which causes a reversible internalization of the receptor into neurons, leading to a more extended NMDAr channel opening and excessive synaptic and extra-synaptic NMDAr activation [4–6].
From the clinical point of view, the subacute onset of several neurological (e.g., cognitive decline, speech impairment, seizures, central hypoventilation, and movement disorders) and psychiatric (e.g., psychosis, anxiety, and depression) symptoms is recognized as diagnostic hallmarks. Furthermore, according to Graus’ criteria [7], laboratory (i.e., cerebral spinal fluid/serum specific auto-antibodies positivity) and radiological (i.e., mesial-temporal signal abnormalities in MRI T2 fluid-attenuated inversion recovery (FLAIR) images of the brain) findings can help the diagnostic process. Anti-NMDAr AE is frequently associated with an underlying tumor pathology, mostly ovarian teratoma, which detection is fundamental for treatment purposes.
Experimental and clinical evidence support the risk of early postnatal mortality and the increased prevalence of neurologic and systemic abnormalities in newborns delivered by mothers affected by anti-NMDAr AE during pregnancy. This phenomenon is partially related to the specific treatment employed for AE management (i.e., antiseizure medications and immunomodulatory drugs) as well as diagnostic interventions (i.e., computer tomography (CT) or magnetic resonance image (MRI) scans with contrast agents) whose teratogenic potential is already well documented. On the other hand, animal models have shown that maternal-to-fetal anti-NR1 auto antibodies transfer can be associated with a dose-dependent altered fetal neurodevelopment which may lead to growth retardation and impaired cognitive functions. Anti-N1 antibodies are an IgG class of antibodies that can cross the placental barrier from the 13th week of gestational age onwards.
This systematic review analyzed the available data on perinatal outcomes of newborns whose mothers have been affected by anti-NMDAr encephalitis during pregnancy. We also highlighted possible risk factors associated with increased newborns’ perinatal mortality and morbidity.
Methods
Searching strategy and review organization
We systematically reviewed the literature using the following search strategy: (“autoimmune encephalitis”/exp OR “autoimmune encephalitis”) AND (“fetal outcome”/exp OR “pregnancy”). The following electronic databases and data sources were systematically searched: MEDLINE (accessed through PubMed), Scopus, and Google Scholar. As per inclusion criteria, we evaluated all studies which (1) reported a confirmed diagnosis of anti-NMDAr encephalitis during pregnancy according to Graus’ criteria and (2) reported fetal and/or newborn outcomes. We included only papers written in English.
Results of this systematic review have been reported following the guidelines of the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) statement. The quality of the included studies was assessed using the Newcastle–Ottawa Quality Assessment Scale (NOS). According to this scale, each study has been evaluated based on eight items, described as follows: (1) representativeness of the exposed cohort, (2) selection of the not exposed cohort, (3) ascertainment of exposure, (4) demonstration that outcome of interest was not present at the start of the study, (5) comparability of the cohorts included, (6) assessment of outcome, (7) adequate length of the follow-up, (8) adequacy of follow-up of cohorts. This score ranges from 0 to 9, and a quality score equal to or higher than three was considered acceptable.
Data collection
The following demographic and clinical information about the mother have been collected: age, gestational age, history of epilepsy, comorbidities, neurologic symptoms at AE onset, seizure characteristics (seizure type), status epilepticus (SE) characteristics, presence of an underlying tumor, EEG features, magnetic resonance image (MRI) findings, immunomodulatory therapy, ASM administered (number, and type), and surgery procedures performed.
Data on stillbirth, type of delivery (vaginal or cesarean), Apgar score 1 and 5 min after delivery, neonatal symptoms, and NMDAr antibodies dosage at birth were collected.
The data were recorded within a specialized Excel spreadsheet.
Statistics
Statistical analysis was performed on the final dataset containing all information pooled from the studies selected by our systematic review. Data were analyzed in IBM SPSS™; the normality of continuous data was checked via the Kolmogorov–Smirnov test. The Fisher chi-square test was employed to compare the perinatal outcome (born at term Vs preterm delivery; born at term Vs spontaneous abortion) according to maternal clinical and treatment features. Alpha level was set at 0.05 for statistical significance.
Results
Literature search
The literature search reported above yielded 156 articles. Seventy-five abstracts were excluded because they did not focus on anti-NMDAr AE during pregnancy or perinatal outcome or did not report individual patients’ data. Of the 138 records screened, the full texts of 63 articles were reviewed for eligibility (Fig. 1). Thirty-seven articles initially considered for possible inclusion were eventually excluded (excluded articles with reasons for exclusion are reported in Fig. 1), and twenty-six were finally included in our review [8–33]. They included twenty-three case reports, and three case series (Table 1). According to the NOS evaluation, 13 articles were scored 5, 6 were scored 4, and 7 were scored 3 (Supp. Tab.1).Fig. 1. Flow chart of the article screening process. The Preferred Reporting Items for Systematic Reviews and Meta-Analyses diagram describes the search from the literature; 138 records were screened; from which, 26 articles were selectedTable 1Patients clinical and neuro-electrofisiological featuresStudyPatientsMaternal Seizures typeSE during pregnancyOncologic evaluationDeliveryApgar(1,5 minutes)IMTASMsSurgeryBorn pre-termNewborns’ sympotmsSerum anti-NMDAr antibodies in newbornsMaternal presenting symptoms and comorbiditiesMaternal additional therapiesMaternalEEGMaternalBrain MRISabrina Kalam et al. 2019[8]1GTCSNoTeratomaSD\Iv CS, IVIg, PLEX\Tumor resectionYes\\Non-specific diffuse cortical dysfunction with no epileptiform activityAmygdala hyperintensity bilaterally, more marked on the rightKim J. et al. 2015[9]1\TeratomaSI\IV CS, PLEX, RTX\Tumor resection\\None\NormalMathis S. et al. 2015[10]1GTCSYesNegativeSD10IVIg, IV CSCNZ, PHT, LMT\NoNo symptoms\\\Lai Wan Chan et al. 2015[11]1\TeratomaSI\CS, PLEX, RTX\Tumor resection\\History of multiple suicide attempts\Bilateral rhythmic and semi-rhythmic delta activities (predominantly frontal)T2-FLAIR Hyperintensities of right hippocampus and cerebellar parenchymaLeah M. Lamale-Smith et al. 2015[12]1Not specified seizure typeYesNegativeCSe3,4IVIg, CS, PLEXLEV, TPM, Midazolam, PHT, CLBBilateral oophorectomyYesLow birth weight, supraventricular tachycardiaPositive, 1:20Depression and anxiety\Diffuse background slowing, right temporal dischargesMedial left temporal lobe and bilateral insula T2 HyperintensitiesJagota P. et al. 2014[13]1\NegativeCSe4,7CS, IVIg\YesIntermittent episodes of continuous fine abnormal movementsPositive, 1:450\Diffuse slow waves with no epileptic discharges\Lu J. et al. 2015[14]1NoNoNegativeSD\CS, IVIg\NoNone\Visual hallucination, hyposexuality, speech disturbance\NormalNo acute intracranial processesMagley J. et al. 2012[15]1NoNoNegativeSD8,9CS, IVIg, PLEX\YesTorticollis, strabismus\Coreoathetosis, bradykinesia, weakness, depressionClonazepam, sertraline, gabapentin, haloperidol, venlafaxineIntermittent polymorphic bilateral frontal slowingAbnormal T2 signal hyperintensity in bilateral caudate, globus pallidus and putamenKumar et al. 2010[16]1GTCSNoTeratomaCSe3,6IVIg, IV CSPHT, LorazepamTumor resection\No symptoms\Headache, malaise, bizarre behavior, paranoid delusionNot specifiedGeneralized slowingNot specified1GTCSYesTeratomaSI\IVIgMDZ, CBZ, GBPTumor resection\\Abnormal behavior, History of ovarian teratomasNot specified1 Hz spikes and slow activity in the frontal lobesNot specified1FS, GTCSNoNegativeSD8,9CSPB\NoNo symptoms\Abnormal behaviorNot specifiedGeneralized high-amplitude slow activityNormalShahani L., 2015[17]1NoNoNegativeSD\Iv CS, PLEX\NoNo symptomsNegativeBizarre behavior, paranoid delusion\NormalNormalMcCarthy A. et al. 2012[18]1NoNoTeratomaCSe\IV CS, PLEX\Tumor resectionYesNo symptoms\Urinary retention, constipation, new daily persistent headache\Diffuse slowingNormalIto et al. 2010[19]1GTCSNoNegativeSD\CSPB\NoNo symptoms\Irritability and speech disturbances\Diffuse high-voltage slow wavesNormalXiao X. et al. 2017[20]1GTCSNoNegativeCSe9IVIg, IV CSLZP, CNZ, CBZ, LEV, VPAWedge-shaped resection of bilateral ovaries (no oncological indication)YesNo symptoms\Psychiatric symptoms, visual and auditory hallucinations\Generalized seizures during sleepNormalLiu H. et al. 2021[21]1 (first pregnancy)NoNoNegativeVA\IVIg, oral and IV CSLMT\Yes\Psychiatric symptoms, oral-face-brachial dystoniaOlanzapineBilateral and diffuse persistent theta-delta slow wavesHyperintense signal in the right hippocampus1 (second pregnancy)NoNoNegativeVA\IVIg, IV CSLEV, LMT\Yes\Psychiatric symptoms, epilepsy\Diffuse slow wavesNegativeBastien J. et al. 2020[22]1GTCSNoTeratomaCSe\IVIg, CSLEVTumor resectionYesRespiratory distress, neuromuscular complicationsPositiveAgitation, delusion, visual hallucinations, headache, oro-facial dyskinesiaAmoxicilline, Aciclovir\Mesio-temporal hyperintensity in T2 wighted sequences1Not specifiedNoNegativeCSe-,9CS, IVIg,\Tumor resectionYesNo symptoms\Bulbar palsy, bilateral facial hypoesthesia, dysartria, bradychardia, agitation\Normal1Not specifiedNoNegativeCSe\CS, IVIg\NoRespiratory insufficiency\Oro-facial dyskinesia, memory problems\Bilateral mesio-temporal hyperintensity in T2 wighted sequences1Temporal lobe seizureNoTeratomaCSe-,10IV CS, IVIg, PLEX, RTX\Tumor resectionYesNo symptoms\Psychotic symptoms\Bilateral mesio-temporal hyperintensity in T2 wighted sequences1GTCSYesNegativeSD-,10CS, IVIgLEV, Propofol\YesNo symptoms\Behavioral changes, difficulties in speaking and readingAmoxicilline, Aciclovir\Normal1FASNoTeratomaCSe\IV CS, IVIg\YesLow birth rate\Nausea, auditory hallucinations, catatonia, autonomic dysfunction, cardiac arrest\NormalKyu-On J. et al. 2020[23]1GTCS, FS (motor seizures)YesNegativeCSe\IVIg, CS, RTXLEV, OXC, LCS, MDZ, CLB\YesNo Symptoms\Headache\Continuous mixed, slow activity in the right temporal area. No epileptiform dischargesRight temporal and Insular cortices hyperintensity. ASL showed increased cerebral blood flow in the right insula and temporal areaScorrano et al. 2023[24]1GTCSNoNegativeCSe9CSLEV, LCS\NoRespiratory distress, hypoglycemia, jaundice, low birth weight, spina bifida\Psychiatric symptoms\NormalDemma L. et al. 2017[25]1GTCSYes (recurrent SE)TeratomaCSe1,9IV CS, IVIg, PLEX, RTX, CyclophosphamideLEV, LCS, PTHTumor resection\\Anxiety, insomnia, hallucinations, feverAntibiotics\Scattered white matter hyperdensitiesTailland M. et al. 2019[26]1GTCSNoNegativeCSe\IV CS, IVIgLEV\NoNo symptoms\Fever, left side hemiparesis, confusion, oro-facial dyskinesia,\Right perisilvian fissure and temporal lobe FLAIR hyperintensity.Lu Y-T et al. 2016[27]1GTCSGCSENegativeCSe\OXC, VPA, PB\No symptoms\\Left temporal ictal theta rhythmLeft mesial temporal hypersignal on FLAIR1GTCSGCSENegativeSD\PHT, VPA\YesNo symptoms\\Right central area focal slowSuperior sagittal sinus thrombosis with venous hemorrhagic infarction1GTCSGCSENegativeSI\LEV\No symptoms\\NormalSuperior sagittal sinus thrombosis with venous hemorrhagic infarction1Not specifiedFSENegativeCSe\PHT, LEV, TPM, PB, VPA\Prematurity with complications\\Left anterior quadrant rhythmic sharp wavesMild hypersignal over left mesial temporal area1GTCSGCSE evolved to NCSENegativeSI\CS, PLEXLEV, VPA, CLB, LMT\No symptoms\\Ictal focal spikes over right frontocentral areaBilateral frontoparietal area hypersignal on DWI; left mesial temporal hypersignal on FLAIR1Not specifiedFSENegativeSI\CS, IVIg,VPA, PHT, CLB, LEV, PB, TPM\NoNo symptoms\\Bilateral independent ictal focal sharp delta activitiesHypersignal over bilateral medial temporal, left posterior insular and bilateral thalami on T2 imaging1GTCSGCSE evolved to NCSETeratomaNot specified\CS, PLEX, AZA, CyclophosphamideVPA, LEV, TPM, CLBNo surgeryYesNot specified\\Rhythmic bifrontal delta with superimposed sharp wavesNormalChourasia N.et al. 2018[28]1Not specifiedNoTeratomaCSe1,2\Lorazepam, LEVTumor resection\Intubation and mechanical ventilation, probable seizuresPositive, 1:320History of anti-NMDA receptor encephalitis and unilateral oophorectomy\Diffuse cerebral edemaUeda A. et al. 2017[29]1NoNoNegativeCSe\IVIg, Iv CS, PLEX\\No symptomsNegativeFever, oro-lingual-facial dyskinesia, choreoathetosis\Diffuse slowingNormalZhang S. et al. 2020[30]1 (first pregnancy)FASNoNegativeNot specified\Iv CS, IVIg\\No symptoms\Visual hallucinations, delusions, systemic lupus erythematosus (SLE)Hydroxychloroquine, prednisone\1 (second pregnancy)FASNoNegativeSI\IVIg, IV CSLMT, LEV, VPA\\Visual hallucinations, delusions, systemic lupus erythematosus (SLE)Hydroxychloroquine, prednisoneSlow theta activity with an extreme delta brush patternNormalLiao Z. et al. 2017[31]1GTCSNoNegativeCSe9,10CS, IVIg, PLEXLEV, VPA\YesLow birth weight\Delirium, visual hallucinations, catatonia,\Paroxysmal middle- slow mixed wave.NormalKokubun N.et al. 2016[32]1NoNoTeratomaVA\CS\Tumor resectionYes\Involontary movement, hypoventilation, past history of a teratoma\\Mizutamari E. et al. 2015[33]1NoNoTeratomaSD\PLEX, IVIg, CS\Right oophorectomyNoNo symptomsNegativeFever, headache, respiratory failure, nucal rigidity, history of left ovarian teratoma\
AZA azathioprine, CFSE complex focal SE, CLB clobazam, CLZ clonazepam, oral or intravenous (IV) corticosteroid (CS), CSe Cesarean section, FAS focal aware seizure, FS focal seizure, GTCS Generalized tonic-clonic seizure, GCSE Generalized convulsive status epilepticus, IVIg Immunoglobulin intravenous, LCS lacosamide, LEV Levetiracetam, LMT lamotrigine, MS myoclonic seizure, NCSE non-convulsive status epilepticus, NE not evaluated, OXC oxcarbazepine, PHB phenobarbital, PHT phenytoin, PLEX plasma exchange, PLEX plasmapheresis, pp post-partum, RTX rituximab, SD spontaneous delivery, SE status epilepticus, SI spontaneous interruption, SW sharp-waves, TPM topiramate, VA voluntary abortion, VPA Valproic Acid
Maternal demographics and clinical features
A literature search showed thirthy-nine pregnant women with a median age of 25 years (range, 16–36 years). Twenty-one patients (21/39, 53.8%) presented anti-NMDAr encephalitis onset within the first trimester of pregnancy, whereas 17 patients (18/39, 46.2%) during the second one. The most common presenting symptoms included abnormal behaviors, movement disorders, autonomic disturbance, and seizures. According to seizure type, nineteen patients (19/39, 48.7%) had tonic–clonic generalized seizures, and six patients (4/39, 10.3%) had only focal seizures. Thirteen patients (13/39, 33.3%) presented status epilepticus and required intensive care management. The oncological evaluation revealed the presence of ovarian teratoma in seventeen patients (14/39, 35.9%). EEG analysis results were reported in 26 patients (26/39, 66.7%) and documented slow activity and interictal epileptic abnormalities in 23 cases (23/39, 59%), whereas ictal discharges and extreme delta brush in three patients (3/39, 7.7%). Brain MRI was normal in all cases except for 21 patients (21/39, 58.3%), who showed cerebellum, hippocampus, bilateral amygdala, basal ganglia, and insular cortex hyperintensity in T2-weighted MRI scans.
Immunotherapy was administered to thirty-five patients (36/39, 92.3.%). Thirty-five patients (35/39, 89.7%) received high oral or EV corticosteroid therapy, 26 mothers (26/39, 66.7%) were treated with IGEV, 6 with third-line treatments (i.e. RTX, cyclophosphamide, and azathioprine) (6/39, 15.4%), and 14 with plasmapheresis (14/39, 35.9%). ASM was administered in 25 (25/39, 64.1%) patients, with levetiracetam (LEV) and phenytoin (PHT) being the most used.
Extensive demographics and clinical information are listed in Table 1.
Perinatal outcomes
Data from 41 subjects in the perinatal period were evaluated. In two cases, the mothers suffered from a first episode of AE during a first pregnancy and a relapse during a second one. In 7 cases (7/41, 17.1%), a spontaneous interruption of the pregnancy was reported, whereas a voluntary interruption was reported in 3 (3/41, 7.3%) Of the 31 remaining alive subjects, 19 (19/31, 61.3%) were born from a cesarean section, and 10 (10/31, 32.3%) had a vaginal delivery. Nineteen subjects (18/31, 58.1%) experienced premature birth.
The APGAR score was available in 14 infants, showing a 5-min score within the normal range in 10. Serum anti-NMDAr antibody levels were tested in 7 cases (7/41, 17.1%) and found positive in 4. These patients showed perinatal complications, which mostly included neuromuscular and respiratory symptoms.
Above all the neurological manifestations reported, impaired neonatal reflexes (i.e., Moro, sucking, and grasping), cervical dystonia, strabismus, movement disorders, spina bifida, and seizures were the most reported. On the other hand, non-neurological symptoms mostly included respiratory depression, low birth weight, and supraventricular tachycardia 13.
Extensive information about perinatal outcomes is listed in Table 1.
Statistical analysis of the pooled data
According to the data analysis of single patients, no differences were observed between mothers who complete their pregnancies and those who experienced a spontaneous interruption (Table 2). However, a trend towards a reduced risk of abortion was also observed in women treated with IVIg (p = 0.06). In addition, a trend towards an increased risk of pre-term born was observed in mothers who underwent surgery procedures for teratoma removal (p=0.06) (Table 3). Table 2. Frequency distribution of clinical features of patients enrolled according to spontaneous interruption of pregnancy. Data were reported as absolute number and relative percentage. Differences comparison between the two groups were assessed by Fisher chi-square test. ASM anti-seizure medication, IVIg intravenous Immunoglobulins, PLEX plasma exchanges, RTX rituximabDelivered pregnancies(n=31)Spontaneous interruption(n=7) p-value
Teratoma 10 (32.3)3 (33.3)0.95 Oral corticosteroid 16 (51.6)3 (33.3)0.33 Intravenous corticosteroid 10 (32.3)4 (44.4)0.49 IVIg 21 (67.7)3 (33.3)0.06 PLEX 9 (29)2 (16.7)0.69 RTX 3 (3.2)2 (22.2)0.31 Seizure 20 (64.5)7 (77.8)0.45 Status epilepticus 9 (29)4 (44.4)0.38 ASM administration 18 (58.1)7 (77.8)0.28 ASM polytherapy (>2 ASM) 8 (25.8)4 (44.4)0.28 Surgery 12 (38.7)3 (33.3)0.77Table 3Frequency distribution of clinical features of patients enrolled according to preterm birth. Data were reported as absolute number and relative percentage. Differences in comparison between the two groups were assessed by Fisher's chi-square test. ASM anti-seizure medication, IVIg intravenous Immunoglobulins, PLEX plasma exchanges), RTX rituximabFull term(n=10)Preterm(n=18) p-value
Teratoma 1 (10)7 (38.9)0.10 Oral corticosteroid 7 (70)10 (55.6)0.45 Intravenous corticosteroid 3 (30)7 (38.9)0.63 IVIg 6 (60)14 (77.8)0.31 PEX 2 (20)7 (38.9)0.30 RTX 0 (0.0)1 (5.6)NA Seizure 5 (50)11 (61.1)0.56 Status epilepticus 2 (20)5 (27.8)0.64 ASM administration 6 (60)10 (55.6)0.81 ASM polytherapy (> 2 ASM) 2 (20)4 (22.2)0.89 Surgery 1 (10)8 (44.4)0.06
Discussion
Anti-NMDAr encephalitis is the most frequent autoimmune encephalitis during pregnancy [34]. According to our data, in the perinatal period, newborns delivered by mothers suffering from anti-NMDAr AE may show neurological (i.e., non-finalistic limb movements, cervical dystonia, strabismus, spina bifida, impaired Moro reflexes, poor sucking and grasping) as well as non-neurological (i.e., respiratory distress, neonatal infection, icterus, hypoglycemia, low birth weight, and supraventricular tachycardia) sequelae (Fig. 2). All individuals developing perinatal symptoms presented positive serum NMDAr antibodies [12, 13, 22, 28]. This evidence supports the notion of a harmful maternal-to-fetal NR1 autoantibody transfer extensively described in preclinical models. However, further concurrent factors should be explored as a putative cause of newborns’ perinatal symptoms onset. In fact, several therapeutic interventions largely employed in AE management such as ASM and immunomodulant therapies (IMT) are associated with a great risk of perinatal complications.Fig. 2. Clinical manifestations in newborns’ delivered by mothers suffering from anti-NMDAr encephalitis
According to the literature, ASM exposure during pregnancy may increase the rate of preterm birth, intrauterine growth restriction, low Apgar score, neonatal hypoglycemia and sepsis, respiratory distress, major congenital malformations (MCMs), and/or cognitive-behavioral impairment [35]. Specifically, some ASM like valproate acid (VPA), phenobarbital (PB), phenytoin (PHT), carbamazepine (CBZ), and topiramate (TPM) have been labeled as the most dangerous in terms of fetal harm. Thus, their use during pregnancy should be avoided. On the other hand, lamotrigine (LMT) and LEV seems to be associated with a very low rate of major congenital malformations (MCMs) and perinatal distress [36, 37]. Surprisingly, according to our results, newborns exposed to VPA during pregnancy mostly presented normal Apgar score, a low rate of miscarriage (3/9, 33.3%), and prematurity with complications (1/9, 11%). However, this data should be interpreted with caution in light of publication and reporting biases.
A solid set of evidence indicates that IMT may increase perinatal disorders in newborns [34]. Even though first-line IMT (i.e., corticosteroids, plasma exchange, and intravenous immunoglobulin) seem to be safe, second-line IMT (i.e., azathioprine, mycophenolate mofetil, cyclophosphamide, and rituximab) should be used with caution given the potential harmful profile towards fetal and newborns’ health. In line with this evidence, our study did not revealed a significantly increased risk of spontaneous pregnancy interruption in mothers who received treatment with RTX. RTX is a chimeric anti-CD20 monoclonal antibody that leads to depletion of B cells in humans, with consequent hypogammaglobulinemia. RTX can cross the placental barrier, and its use during pregnancy has been associated with neonatal transient lymphopenia and decreased gamma globulin levels.
A potential increase of pre-term birth was also described for women with ovarian teratoma who underwent subsequent surgical treatment. According to the literature, pregnant women suffering from cancer generally show an increased risk of abortion (i.e., 10% higher) than the general population. Furthermore, large epidemiological studies have shown that non-obstetric surgery in pregnant patients is associated with small, but real, increases in the risks of stillbirth, preterm delivery, and the need for cesarean section. This is mainly related to the anesthesia risk, the pre-operatory imaging, the development of changes in fetal hemodynamics, and the fetal surgical stress, still largely unknown [38–42]. However, a fetal monitoring during surgery, anesthesia between 4 and 20 gestational weeks, a regular patient follow-up with high-resolution ultrasonography, and attention to clinical symptoms and other signs were associated with a relatively safe non-obstetric surgery [38–42].
Conclusions
The management of pregnancy in women with anti-NMDAr encephalitis remains challenging. Our study depicted the potential outcomes of children born from mothers suffering from anti-NMDAr encephalitis and analyzed risk factors related to pregnancy and maternal disorders. To prevent complications that could harm the mother and the child, a personalized management should be enforced, targeting potential fetal risks related to anti-NMDAr encephalitis, autoantibodies, and therapy administered during pregnancy.
Supplementary Information
Below is the link to the electronic supplementary material.Supplementary file1 (DOCX 22.8 KB)