A case of chorea-acanthocytosis with significant improvement of symptoms at one year with deep brain stimulation: case report and literature review
Yan Xu, Jiabin Yu, Yimeng Gao, Qiaozhen Su, Haitao Xie, Hongfeng Liang, Chunye Zheng

TL;DR
A man with chorea-acanthocytosis showed significant symptom improvement after deep brain stimulation, offering new treatment insights.
Contribution
First report of involuntary vocalizations relief and near-complete reduction of salivation and trunk movements in ChAc using DBS.
Findings
Patient showed significant improvement in speech, salivation, and trunk movements after GPi-DBS.
Involuntary vocalizations were notably reduced following treatment.
Symptoms remained stable after one year of follow-up.
Abstract
Chorea-acanthocytosis (ChAc) is a rare, neurodegenerative disorder caused by mutations in the VPS13A gene. In this article, we report on a 32-year-old man diagnosed with ChAc, with involuntary movements of the mouth and trunk, drooling of the mouth, slurred speech, and abnormal vocalizations as the main clinical manifestations. Three weeks after implantation of globus pallidus internal (GPi)-deep brain stimulation (DBS), the patient’s symptoms improved significantly. For example, articulation is clear, involuntary trunk movements and salivation have largely disappeared, and abnormal vocalizations have been significantly reduced. After 1 year of follow-up, the improvement in involuntary movement symptoms is essentially the same as before. As far as we know, we are the first to report the relief of involuntary vocalizations in a patient with GPi-DBS treatment, and that salivation and…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
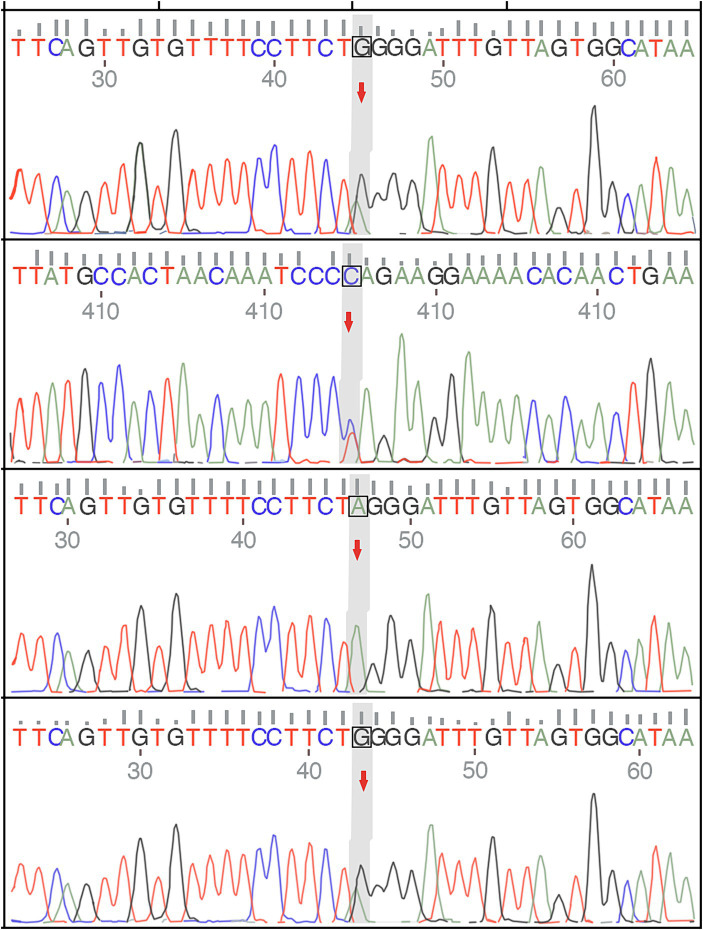 Figure 1
Figure 1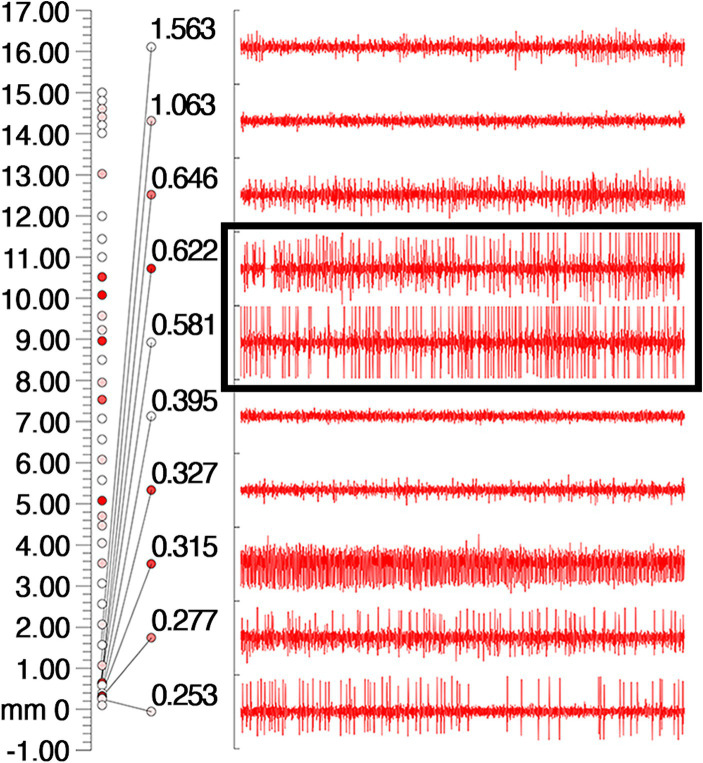 Figure 2
Figure 2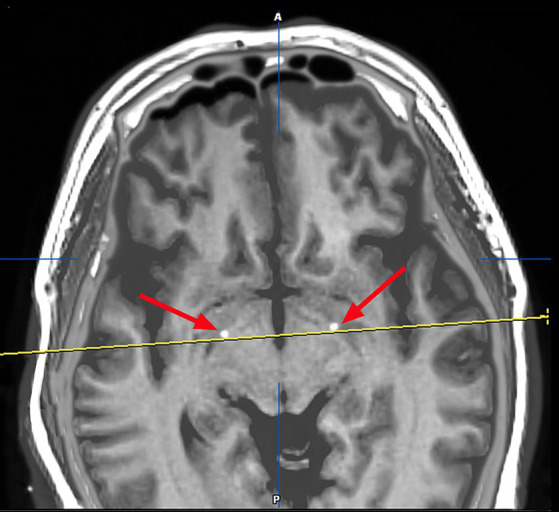 Figure 3
Figure 3| Location | X (mm) | Y (mm) | Z (mm) | Ring | Arc | Current | Pluse width (μs) | Frequency (Hz) |
|---|---|---|---|---|---|---|---|---|
| Left | 122.8 | 99.5 | 101.0 | 54.7° | 109.4° | 2.0 V | 120 | 135 |
| Right | 89.1 | 99.7 | 104.2 | 54.1° | 75.4° | 2.0 V | 120 | 135 |
| Time/Author | Age/Sex | VPS13A mutations | Main symptoms | Current | Pluse width (μs) | Fre (Hz) | UHDR (pre-op) | Follow-up (m) | UHDRS (post-op) | Outcome |
|---|---|---|---|---|---|---|---|---|---|---|
| 2009/Ruiz et al. ( | 35/F | NA | Oromandibular dyskinesia, dysarthria, irregular choreic gait with truncal spasm | (L)4.4 V | 180 | 130 | 24 | NA | 14 | Rapid relief of tension disorder and chorea symptoms, dysarthria did not improved |
| 2012/Shin et al. ( | 39/F | + | Whole body involuntary movement, orolingual dyskinesia with tongue protrusion and lip biting, involuntary head banging | (L)3.0 V | 90 | 130 | 44 | 13 | 12 | Dystonia, bradykinesia, choreic movements of the limbs and trunk had significantly improved, no improvement in chewing and biting of lips and tongue |
| 2012/Li et al. ( | 39/M | NA | Orofacial and lingual dyskinesia, shoulder shrugging, neck stretching and tongue biting, chorea of the lower limbs and trunk | (L)3.5 V | 60 | 40 | 36 | 9 | 13 | Obvious improvement in chorea symptoms and dysphagia, mild improvements in dystonia with 40 Hz stimulation of the GPi, both chorea and dystonia were exacerbated by 130 Hz GPi stimulation. |
| 30/M | NA | Orofacial and lingual dyskinesia with tongue biting, generalized chorea and trunk spasms, difficulties in writing, speaking, swallowing, and walking | (L)3.5 V | 60 | 40 | 53 | 5 | 27 | ||
| 2013/Kefalopoulou et al. ( | 54/M | NA | Orofacial dyskinesias and feeding dystonia, violent trunk spasms | (L)2.5 V | 60 | 130 | 40 | NA | 23 | Upper limb dexterityand truncal dips improved markedly, no improvement in feeding dystonia |
| 43/M | NA | Oromandibular dyskinesias, dysarthria, violent choreic movements of upper and lower limbs, lurching gait and poor balance | (L)2.5 V | 90 | 130 | 74 | NA | 50 | Significant improvement in choreic movement, walking and truncal spasms | |
| 2015/Nakano et al. ( | 43/M | NA | Involuntary movements of the tongue and all extremities | (L)3.0–3.5 V | 60–90 | 160 | 52 | 12 | 31 | The dexterity of the upper extremities improved markedly |
| 40/M | NA | Dysarthria and oromandibular dyskinesia, progressive violent choreic movement of all extremities, trunk spasm and head-drop | (L)3.0–3.5 V | 60–90 | 160 | 50 | 12 | 36 | Decreased limb movement, dysarthria and slight head-drop did not improved | |
| 2015/Lee et al. ( | 36/M | + | Slurred speech, orofacial olingual dyskinesia, biting tongue and lip, and choreiform movements of the head and neck | (L)2.9 V | 60 | 130 | 59 | 6 | 36–34 | Marked improvement in choreic movements, biting tongue and lip |
| 2016/Fernández-Pajarín et al. ( | 43/M | + | Abnormal movements of the orofacial region, upper limbs and trunk | (L)4 mA | 212 | 60 | 39 | 12 | 13 | Marked improvement in orofacial dyskinesias and limb choreic movements |
| Author | Age/ | VPS13A | Main Symptoms | Current | Pluse width (μs) | Fre (Hz) | UHDRS | Follow-up | UHDRS | Outcome |
| 2018/Liu et al. ( | 35/M | + | Clenching and biting, dysphagia, slurred speech, involuntary head and limb | (L)2.6–3.5 mA | 70–100 | 150–165 | 62 | 12 | 18 | Clinical improvement |
| 37/M | + | Biting, dysphagia, twitching limbs and trunk weakness and numbness of hands, myocardial infarction | (L)2.5–3.8 mA | 80–140 | 150–175 | 42 | 12 | 12 | ||
| 37/M | + | Biting, tongue involuntary movements, vocal tics, involuntary limb movements, generalized tonic–clonic seizure attack | (L)2.0–3.0 mA | 60–80 | 135–165 | 24 | 12 | 8 | ||
| 35/M | + | Biting, tongue involuntary movements involuntary limb movements, generalized tonic–clonic seizure attack | (L)2.5 mA | 90 | 160 | 22 | 12 | 8 | ||
| 36/F | + | licking lips, pouting, biting, dysphagia, chorea, gait instability | (L)2.0–2.7 mA | 90–100 | 150 | 48 | 12 | 14 | Clinical improvement | |
| 33/F | + | Biting, slurred speech, trembling legs and twitching arms, generalized tonic–clonic seizure attack | (L)0.0–1.6 mA | 60 | 130–145 | 16 | 12 | 6 | ||
| 2018/Doshi et al. ( | 77/F | NA | Orofacial dyskinesias, neck dyskinesias | (L)3.0 V | 90 | 130 | 36 | NA | 13 | Dyskinesias were completely resolved |
| 2019/Richard et al. ( | 31/M | + | Orolingual hyperkinesia, dysarthria, truncal and extremities chorea, gait instability, hyporeflexia, bradykinesia | (L)2.6 V | 60 | 100 | 13 | 6 | 4 | Speech, chorea and swallowing are ameliorated |
| 2019/Wang et al. ( | 43/F | NA | Dysphagia, dysarthria, involuntary tongue protrusion, biting lip, and teeth grinding | (L)2.2 V | 60 | 130 | 61 | 12 | 31 | Significantly improvement in dysarthria, chorea and dyskinesia |
| 2020/Wu et al. ( | 35/F | + | Involuntary movements of tongue, lower jaw, neck, trunk, and lower limbs, biting tongue and lip | (L)3.0 V | 60 | 160 | 51 | 12 | 27 | Remarkable remission in tongue biting, dysarthria, and gait abnormality |
| 35/M | + | Oromandibular dystonia, involuntary jaw movement, and upper limb right limb affecting handwriting. | (L)3.0 V | 50 | 130 | 40 | 12 | 22 | Remission of involuntary orofacial movements |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsNeurological disorders and treatments · Genetic Neurodegenerative Diseases · Neurological and metabolic disorders
Introduction
Chorea-acanthocytosis (ChAc) is an extremely rare autosomal recessive neurodegenerative disorder caused by mutations in VPS13A, which is located on 9q21, and is a subtype of neuroacanthocytosis syndrome (1). Its main clinical features include progressive movement disorders, seizures, psychiatric symptoms, cognitive deficits, etc., and orofacial dyskinesia is one of its most prominent features, and there may be self-injurious behavior (2, 3). The prevalence of the disease is about 1: 1,000,000, and most patients with ChAc have elevated creatine phosphokinase (CK) levels, in addition to the fact that ChAc is mainly characterized by peripheral blood acanthocytosis (4). Magnetic Resonance Imaging (MRI) of the brain generally shows bilateral symmetrical atrophy of the caudate nucleus. Clinical treatment options for ChAc are currently greatly limited and only limited improvement from symptomatic and supportive therapy (5). Previous studies have found that GPi-DBS not only improves dystonia and choreiform symptoms in ChAc patients, but may also be the best option for ChAc patients with predominantly orofacial and submandibular dystonia (6–8). At the same time, we also reviewed the relevant literature to explore the characteristics and advantages of GPi-DBS treatment of ChAc, in hopes of creating a reference for future ChAc treatments.
Case presentation
A 32-year-old man presented in September 2022 with involuntary movements of the corners of the mouth, drooling of the mouth (noticeable during eating or drinking), frequent involuntary vocalizations (similar to grunting) slurred speech, occasional involuntary forward flexion, and an unsteady gait. The patient’s choreic symptoms had significantly worsened after 6 months, such as more frequent involuntary movements of the corners of the mouth and involuntary movements of the limbs, occasional involuntary forward flexion of the trunk with a slight tilt to the right when walking, and the number of abnormal vocalizations made increased. Moreover, he developed new symptoms, involuntary turning of the neck and shrugging of the shoulders, involuntary grimacing, and lacking fluency in swallowing. The patient had no other typical symptoms, such as cognitive, psychiatric, neuropathic, or myopathic symptoms or seizures. A physical examination of the patient revealed dysarthria, occasional choking on food or water, decreased sensation of the posterior pharyngeal wall bilaterally, reduced pharyngeal reflexes on both sides of the pharyngeal wall, slow elevation of the soft palate bilaterally in the region, a slight decrease in muscle tone in the extremities, and muscle strength of the limbs of Grade 5. Furthermore, his knee-jerk and achilles tendon reflexes were diminished. Laboratory tests indicated the presence of 9% acanthocytes in the blood smear, while serum ceruloplasmin levels were within the normal range at 284 mg/L (normal values range from 150–600 mg/L). The cranial MR suggests atrophy of the caudate nucleus on the left side of the cranium. According to the electromyogram results, abnormalities in the measured tibial nerve H-reflex suggest damage to the lumbosacral nerve root. Nerve conduction and electro-neurography of the remaining extremities showed no significant abnormalities. The genetic examination results (Figure 1) showed the patient had two heterozygous mutations in the VPS13A gene, mutation 1 (c.7253A > G, p.Asn2481Ser, source of variation: father) was located in the coding region: nucleotide 7,253 was mutated from adenine to guanine resulting in a mutation of amino acid 2,481 from asparagine to serine. Mutation 2 (c.8908-2A > G, source of variation: mother) was located at the classical splice site: the second nucleotide upstream of nucleotide 8,908 was mutated from adenine to guanine, and this mutation may result in aberrant splicing of the exon, which could lead to aberrant mRNA splicing affecting the normal structure and function of the translated protein product. And these mutations not were reported previously.
The genetic examination results of the patient and show a single nucleotide variant and a small fragment insertion–deletion variant.
In the process of tracing the patient’s history, we found that there was no family history of neurological disease. In the past six months, the patient has tried a variety of drugs in other hospitals. In January 2023, the patient took tiapride hydrochloride (0.1 g/tid) and pramipexole (0.125 mg/tid). However, the symptoms did not improve. In one month, the patient accepted diazepam (5 mg/bid) and haloperidol (1 mg/bid), and the involuntary movements of the corners of the mouth began to improve, but as the patient continued to take the medication, the symptoms returned to the beginning. We tried treating the patient with levodopa and benserazide hydrochloride (0.125 mg/tid) after admission, but the symptoms did not improve. We also tried using Chinese medicine recipes for the patient. After taking Prof. Huang’s experienced Ge-Gen -Decoction, his drooling symptoms improved slightly, and other symptoms had not improved, but he wanted a greater improvement in the treatment effect. In the end, we recommend that patients try GPi-DBS therapy after careful consideration.
On March 23, 2023, we performed stereotactic deep brain electrode placement, as shown in Figure 2. In the first half of the procedure, deep brain electrodes are implanted while the patient is awake. Intraoperative electrophysiologic recordings of the GPi nuclei were satisfactory and in the correct position, and the location parameters are detailed in Table 1. After completing the first half of the procedure, we performed a Computed Tomography (CT) scan, fused the CT data with the preoperative implantation plan, and began implanting the peripheral pulse generator under general anesthesia after confirming the accuracy of the implantation position (Figure 3). We selected the corresponding parameters after a comprehensive evaluation based on the patient’s intraoperative symptom improvement and tolerance level (9). The frequency of the intraoperative test was 130 Hz, and the pulse width was 60 μs. In the third week after surgery (April 13, 2023), the patient returned to the hospital and DBS was turned on, and the stimulation parameters also started from low current and low frequency, and were slowly adjusted upward, while observing the patients’ symptom relief changes, and finally selecting the appropriate stimulation frequency and current (Table 1). Respectively, we assessed the patient’s pre-operative and post-operative Montreal Cognitive Assessment scores of 27 and 26(>26 normal cognitive functions). And we also assessed the patient’s pre-operative total Unified Huntington’s Disease Rating Scale (UHDRS) motor score of 53 and at post-operative week 3, a total UHDRS motor score of 21. After 1 year of follow-up, the improvement in involuntary movement symptoms is essentially the same as before. Ultimately, the patient’s choreic symptoms improved significantly, and a significant reduction in abnormal vocalizations.
Intraoperative electrophysiologic monitoring unit observed cellular discharges typical of GPi. The coordinates on the leftmost side of the picture, the number 0 indicates the preset depth of the target point, the number 17 indicates 17 mm above the target point, and the cellular discharges are continuously recorded from the number 17 downwards, and the cellular discharges are the most typical and obvious in the black box, and then 0.622 mm and 0.531 mm above the target point. The different colored circles are related to the background sound (the sound during intraoperative testing of the nuclei), with the higher the background sound the redder the color.
Image after fusion of preoperative MR plan and postoperative CT and it is a postoperative image fusion, suggesting that the stimulation electrode is precisely located in the GPI nucleus.
Literature review
Through literature reviewed in the PubMed database from 1978 to 2023, a total of 35 patients treated with DBS were identified. In the end, 21 patients were included, as detailed in Table 2, after removing reports with grossly incomplete information or inaccessible literature. The first attempt to treat ChAc with DBS was made by Wihl et al. (21), however, the patients failed to benefit from DBS treatment. Since then, approximately 30 patients have been successfully treated with DBS for ChAc, with varying results and frequency of treatment. Significant remission of chorea and dystonia was achieved in all patients, with variable results for improvements in symptoms such as dysarthria and dysphagia. This could be related to different stimulus frequencies, pulse widths, or current intensities in individual patients.
Discussion
Neuroacanthocytosis (NA) is a neurological syndrome associated with acanthocytosis, and its identification, diagnosis, and nomenclature have evolved. It was mainly used to characterize ChAc, McLeod syndrome (MLS), and Huntington’s disease-like 2 (HDL2) between 2001–2017, and it is understood that the current understanding of NA includes diseases caused by mutations in the VPS13A and XK genes (22, 23). However, there is a significant overlap in clinical symptoms, laboratory investigations, and imaging manifestations between the two subtypes. Genetic diagnosis is the primary method of differentiation. XK disease is a genetic disorder caused by mutations in the XK gene on the X chromosome that result in the loss or dysfunction of the encoded protein (24). The presentation of XK disease is characterized by muscular involvement, such as skeletal muscle myopathy, and peripheral neuropathy, and it can also affect other organ systems. Particularly, involvement of the heart may be a characteristic feature of the disease (25, 26).
ChAc is the most common type of neuroacanthocytosis. It may also be called VPS13A disease and is caused by pathogenic variants in the gene (27). The peak age of onset of the disease is 30–40 years of age, with progressive exacerbation of symptoms (28). Choreiform movements were the most prevalent clinical symptom in the disease (88%), followed by orofacial dystonia (80%), which includes increased facial expressions such as grimacing, smacking of the tongue, and biting of the tongue and lips (29, 30). Laboratory tests probably reveal an increase in the percentage of peripheral blood acanthocytes, which is a hint of the diagnosis of ChAc (31). Moreover, serum CK levels are significantly elevated. An Electromyogram is dominated by neuroaxonal damage and myopathic changes. Besides, cranial imaging may show symmetrical bilateral atrophy of the caudate. In this case, the patient was genetically tested and had classic choreic symptoms, so the ChAc diagnosis was clear.
At present, ChAc disease has no specific treatment, medications (such as dopamine blockers and VMAT2 inhibitors) can improve dyskinesia or rather chorea significantly, however not all of the symptoms of ChAc respond, and there may be side effects. Therefore, it is crucial to develop effective therapeutic approaches and evaluate treatment outcomes for ChAc patients. DBS is a widely used mainstream treatment for the treatment of movement disorders (9, 32). However, due to ChAc rarity, determining DBS therapeutic efficacy and safety remains challenging. A study was conducted to compare short- and long-term DBS treatment outcomes in fifteen ChAc patients, and the study found significant improvement in both chorea and dystonia, but results for dysarthria and swallowing were mixed. Additionally, akinesia did not improve among the patients (8). It is worth noting that we found most patients experience symptomatic relief with medium to high-frequency stimulation when summarizing the previous literature (Table 2), but Li et al. (7) reported two patients whose symptoms were relieved by low-frequency 40 Hz stimulation, on the contrary, both chorea and dystonia were exacerbated by 130 Hz GPi stimulation. We also found that most patients had pulse widths between 60 and 90 μs, with only two patients exceeding 150 μs and the stimulation current was between 2.5–3.0 volt (V) in most patients and 2.0–4.0 mA in some patients. The rational choice of stimulation frequency, pulse width, and current size for DBS treatment needs more research to verify, and we hope to make the treatment of the disease by DBS more standardized in the future.
In our case, the patient exhibited significant improvement in choreiform symptoms, It greatly improved the patient’s overall quality of life. To our knowledge, this is the first reported case of relief of involuntary vocalization symptoms through GPi-DBS treatment. Our patient had similar symptoms to a previously reported patient who experienced involuntary vocalizations (9). However, the patient in that report did not benefit from GPi-DBS stimulation. Fortunately, our patient responded well to the GPi-DBS treatment, with a reduction in involuntary vocalization, and movements of the trunk almost disappeared.
In conclusion, the patient’s symptoms have improved with DBS, particularly chorea, involuntary vocalization, and salivation at the corners of the mouth. It is reasonable to consider DBS as a safe treatment option for ChAc patients. However, the current reports on DBS for ChAc patients are mainly derived from a limited number of case reports and some small-sample retrospective studies from around the world. Therefore, further studies are still needed to confirm its efficacy and safety. Additionally, we believe that it is necessary to conduct long-term postoperative follow-ups of ChAc patients to continuously improve the treatment program and enhance their quality of life.
Data availability statement
The datasets presented in this article are not readily available because of ethical and privacy restrictions. Requests to access the datasets should be directed to the corresponding authors.
Ethics statement
Ethical review and approval was not required for the study on human participants in accordance with the local legislation and institutional requirements. Written informed consent from the patients/participants or patients/participants' legal guardian/next of kin was not required to participate in this study in accordance with the national legislation and the institutional requirements. Written informed consent was obtained from the individual(s) for the publication of any potentially identifiable images or data included in this article.
Author contributions
YX: Investigation, Writing – original draft, Methodology. JY: Formal analysis, Methodology, Resources, Writing – original draft. YG: Data curation, Writing – original draft. QS: Conceptualization, Methodology, Resources, Writing – review & editing. HX: Methodology, Supervision, Validation, Writing – review & editing. HL: Conceptualization, Data curation, Validation, Writing – review & editing. CZ: Conceptualization, Resources, Writing – review & editing.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Kaestner L. Proceedings of the eleventh international meeting on Neuroacanthocytosis syndromes. Tremor Other Hyperkinet Mov (N Y). (2023) 13:41. doi: 10.5334/tohm.826, PMID: 37928888 PMC 10624129 · doi ↗ · pubmed ↗
- 2Huang S Zhang J Tao M Lv Y Xu L Liang Z. Two case reports of chorea-acanthocytosis and review of literature. Eur J Med Res. (2022) 27:22. doi: 10.1186/s 40001-022-00646-735130982 PMC 8822714 · doi ↗ · pubmed ↗
- 3Walker RH. Untangling the thorns: advances in the Neuroacanthocytosis syndromes. J Mov Disord. (2015) 8:41–54. doi: 10.14802/jmd.15009, PMID: 26090076 PMC 4460540 · doi ↗ · pubmed ↗
- 4Jung HH Danek A Walker RH. Neuroacanthocytosis syndromes. Orphanet J Rare Dis. (2011) 6:68. doi: 10.1186/1750-1172-6-68, PMID: 22027213 PMC 3212896 · doi ↗ · pubmed ↗
- 5Peikert K Danek A Hermann A. Current state of knowledge in chorea-Acanthocytosis as core Neuroacanthocytosis syndrome. Eur J Med Genet. (2018) 61:699–705. doi: 10.1016/j.ejmg.2017.12.007, PMID: 29253590 · doi ↗ · pubmed ↗
- 6Wu Y Xu YY Gao Y Li JM Liu XW Wang MQ. Deep brain stimulation for chorea-acanthocytosis: a systematic review. Neurosurg Rev. (2022) 45:1861–71. doi: 10.1007/s 10143-022-01735-135020105 · doi ↗ · pubmed ↗
- 7Li P Huang R Song W Ji J Burgunder JM Wang X. Deep brain stimulation of the globus pallidus internal improves symptoms of chorea-acanthocytosis. Neurol Sci. (2012) 33:269–74. doi: 10.1007/s 10072-011-0741-y, PMID: 21863267 · doi ↗ · pubmed ↗
- 8Miquel M Spampinato U Latxague C Aviles-Olmos I Bader B Bertram K. Short and long term outcome of bilateral pallidal stimulation in chorea-acanthocytosis. P Lo S One. (2013) 8:e 79241. doi: 10.1371/journal.pone.0079241, PMID: 24223913 PMC 3818425 · doi ↗ · pubmed ↗