Rectal endoscopic full-thickness resection of peritoneal loose body
Minyuan Yang, Jinfeng Ren, Zhengying Yang, Xihui Yuan, Tianyu Liu

Abstract
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
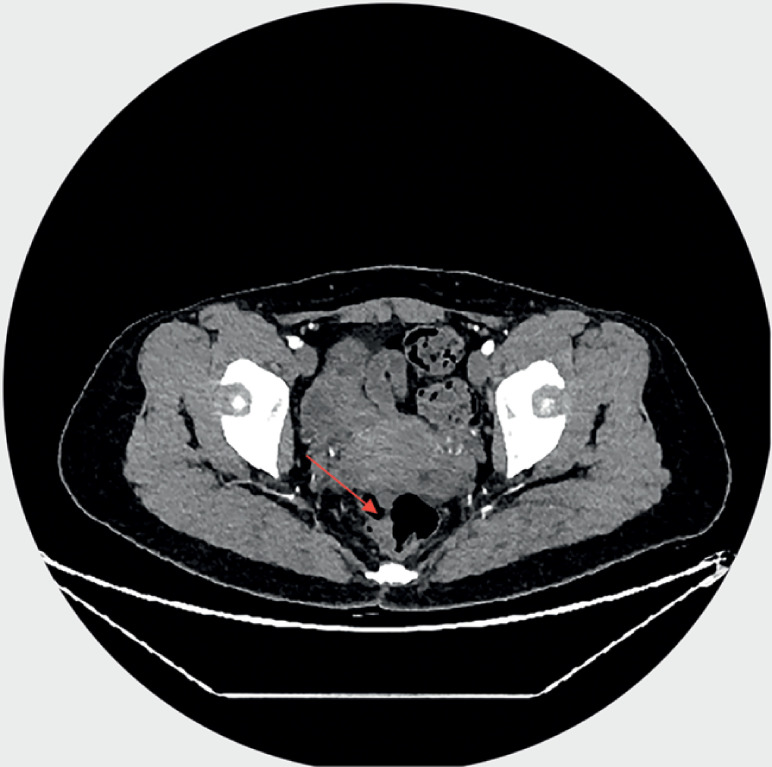 Fig. 1
Fig. 1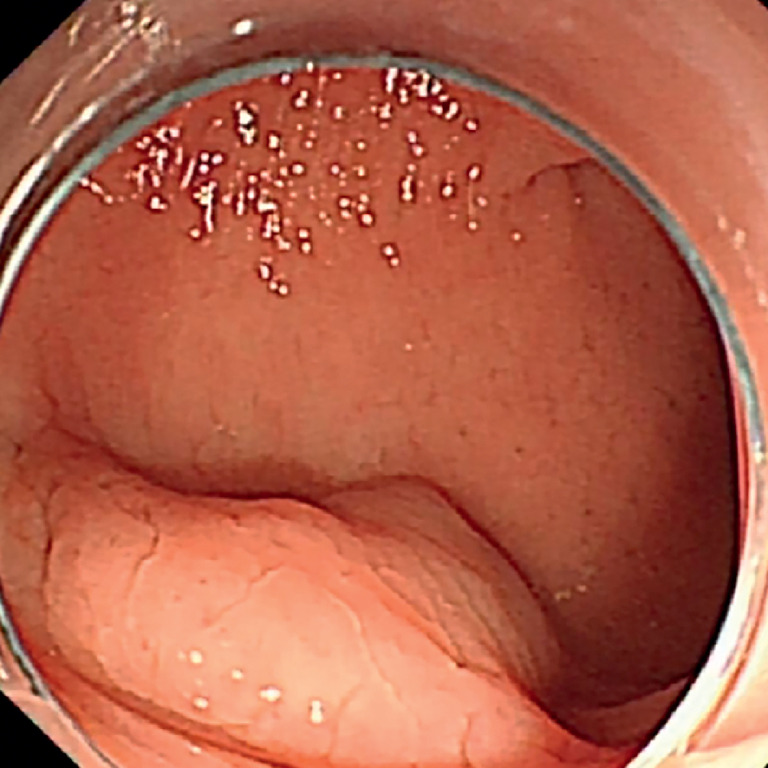 Fig. 2
Fig. 2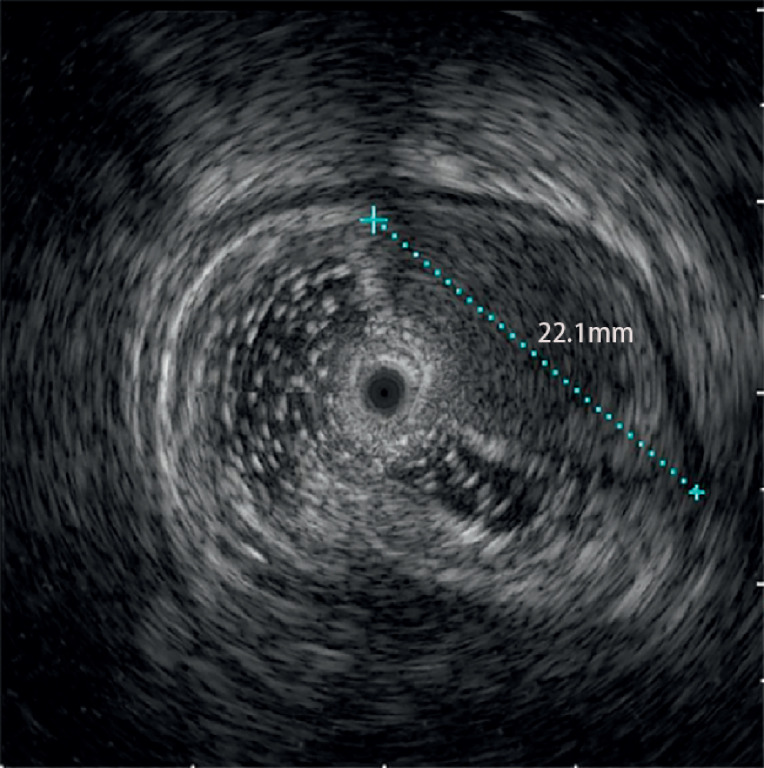 Fig. 3
Fig. 3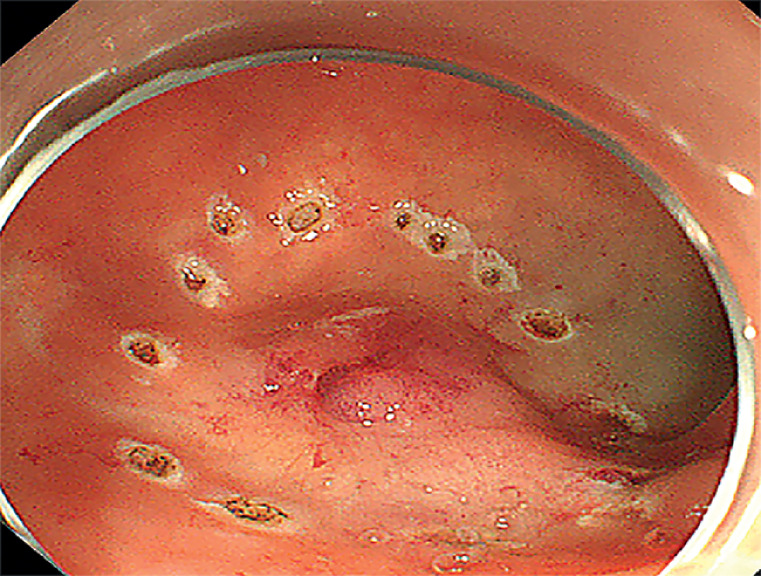 Fig. 4
Fig. 4- —Suining Central Hospital Projects
- —Sichuan Medical Scientific Research Youth Innovation
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsOmental and Epiploic Conditions · Intestinal and Peritoneal Adhesions · Appendicitis Diagnosis and Management
A 36-year-old woman presented with recurrent lower abdominal pain for 6 months. Abdominal contrast-enhanced computed tomography (CT) showed a 1.2-mm enhancing lesion in the upper rectum ( Fig. 1 ). Intestinal endoscopy revealed a 1.5 × 1.2-cm rectal mass located 15 cm from the anal dentate line ( Fig. 2 ). Mucosal biopsy indicated mild chronic inflammation. Endoscopic ultrasonography revealed a 2.2-cm submucosal lesion with an intact mucosal layer ( Fig. 3 ). After obtaining consent from the patient, submucosal tumor endoscopic resection was planned, but formation of the liquid pad by injection proved difficult. The margins of the lesion on the mucosal surface were marked using electrocoagulation ( Fig. 4 ). After obtaining a second consent, rectal endoscopic full-thickness resection was performed ( Video 1 ). A balloon catheter was placed in the sigmoid colon to block fecal matter. An endoscopic mucotomy knife (KD-650Q; Micro-Tech Co., Ltd., Nanjing, China) was used to incise the marked mucosa until an orifice formed. Then, an IT knife (KD-650L; Micro-Tech Co., Ltd.) was used to incise the full thickness around the lesion. After inspecting the outer intestinal wall fascia, an endoscopic electrified snare was used to dissect the lesion into two sections. The defect in the rectal wall was sutured using three three-armed clips (STA00002; Micro-Tech Co., Ltd.) and several titanium clips (ROCC-D-26–195-C; Micro-Tech Co., Ltd.). Histological examination of the biopsy specimen showed chronic submucosal inflammation with foam cell reaction and no abnormal cells at the horizontal and vertical margins. During the operation, no gas entered the abdominal cavity, all abdominopelvic cavity organs remained unaffected, and there was minimal bleeding. Follow-up after 6 weeks showed no residual mass on contrast-enhanced CT, with only scars and two clips at the junction site observed.
Preoperative abdominal contrast-enhanced computed tomography showing a lesion (red arrow) in the upper rectum.
Preoperative intestinal endoscopy showing a rectal mass.
Endoscopic ultrasonography showing a 2.2-cm submucosal lesion.
After failing to create a liquid pad by injecting epinephrine and methylene blue, electrocoagulation was used to delineate the margins of the lesion.
Rectal endoscopic full-thickness resection of a peritoneal loose body in a 36-year-old woman.Video 1
The postoperative biopsy revealed foam cells, consistent with the characteristics of peritoneal loose bodies 1 . This is the first reported case of endoscopic resection of a peritoneal loose body. The endoscopic procedure demonstrated efficiency and safety in this case. However, large-scale clinical studies are needed in the future.
Endoscopy_UCTN_Code_TTT_1AQ_2AH
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Baert L De Coninck S Baertsoen C Giant peritoneal loose body: a case report and review of the literature Acta Gastroenterol Belg 20198244144331566335 · pubmed ↗