Which is cheaper: a fully covered metallic stent or a choledochoscope?
Liang-Hao Hu, Ping-Ping Zhang, Ting Yang, Yan-Wei Lv

Abstract
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
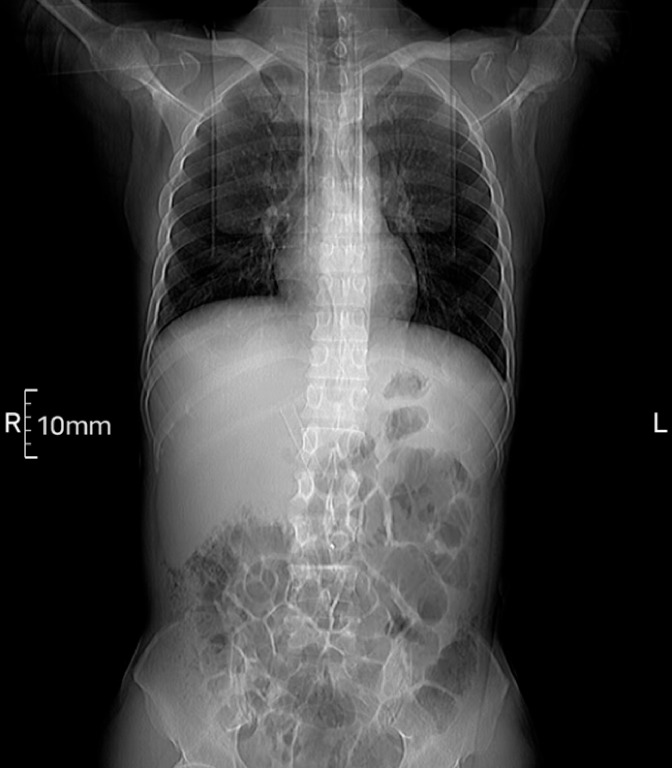 Fig. 1
Fig. 1 Fig. 2
Fig. 2 Fig. 3
Fig. 3 Fig. 4
Fig. 4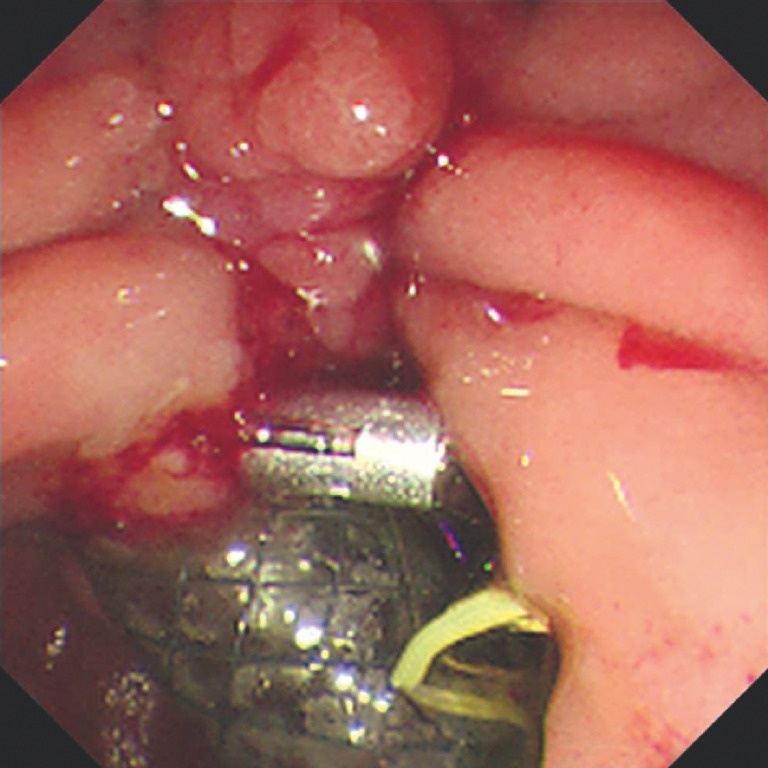 Fig. 5
Fig. 5Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsGallbladder and Bile Duct Disorders · Pediatric Hepatobiliary Diseases and Treatments · Pancreatic and Hepatic Oncology Research
Benign biliary obstruction may occur in patients with chronic pancreatitis 1 2 . Endoscopic placement of a fully covered self-expandable metallic stent (FCSEMS) for biliary drainage is an effective treatment strategy for biliary obstruction 3 . However, the migration rate of FCSEMSs is approximately 10% to 33% 4 5 . We report successfully repositioning a dislocated biliary FCSEMS using a choledochoscope.
A 49-year-old man with chronic pancreatitis with benign bile duct stenosis was admitted due to obstructive jaundice. Endoscopic retrograde cholangiopancreatography (ERCP) was performed and a FCSEMS (EVO-FC, 6 cm; Cook Medical) was placed. The patient developed a fever on the 15th day after the operation. Abdominal computed tomography indicated migration of the biliary FCSEMS ( Fig. 1 ). Another ERCP procedure was performed. Cholangiography indicated that the FCSEMS in the common bile duct (CBD) had moved into the proximal bile duct and the stent was mobile ( Fig. 2 ). The lower segment of the CBD (a length of 2 cm) was significantly narrowed, while the diameter of the middle and upper segments of the CBD was dilated to approximately 1.3 cm. We used a choledochoscope (SpyGlass; Boston Scientific) to reposition the FCSEMS ( Fig. 3 ). The retrieval string of the FCSEMS was visible. A biopsy forceps (SpyBite Max; Boston Scientific) was inserted through the accessory biopsy channel of the choledochoscope ( Fig. 4 ) and the retrieval string was grasped under direct visualization. The displaced FCSEMS was partially pulled out to the opening of the duodenal papilla. Finally, the stent was fixed to the papilla opening with a hemostatic clip (ROCC-F-26-165C; Micro-Tech) to prevent it from moving again ( Fig. 5 , Video 1 ).
Abdominal coronal computed tomography showed migration of the biliary fully covered self-expandable metallic stent (FCSEMS).
Cholangiography showed that the FCSEMS in the common bile duct had moved into the proximal bile duct.
Use of a choledochoscope (SpyGlass; Boston Scientific) to directly visualize the distal end of the stent.
A biopsy forceps was inserted into the bile duct through the biopsy channel of the choledochoscope.
The stent was fixed to the surface of the papilla by means of a hemostatic clip.
Successful repositioning of a dislocated biliary fully covered self-expandable metallic stent using a choledochoscope.Video 1
Choledochoscope-assisted repositioning of biliary FCSEMSs can be considered as feasible and has the advantages of safety and easy operation. Repositioned stents are not deformed and can continue to be used. However, in clinical practice the therapeutic choice between using the choledochoscope to adjust a displaced FCSEMS or to replace the displaced stent with a new FCSEMS should be based on a comprehensive consideration of all the elements including local medical conditions and medical expenses.
Endoscopy_UCTN_Code_TTT_1AR_2AZ
Correction: Which is cheaper: a fully covered metallic stent or a choledochoscope?Hu Liang-Hao, Zhang Ping-Ping, Yang Ting et al. Which is cheaper: a fully covered metallic stent or a choledochoscope? Endoscopy 2024; 56: E695–E696, doi:10.1055/a-2351-2645 In the above-mentioned article, the author name “Ting Yang” was corrected. This was corrected in the online version on August 22, 2024.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Costamagna G Boskoski I Current treatment of benign biliary strictures Ann Gastroenterol 201326374024714594 PMC 3959511 · pubmed ↗
- 2Deviere J Nageshwar Reddy D Puspok A Successful management of benign biliary strictures with fully covered self-expanding metal stents Gastroenterology 201414738539524801350 10.1053/j.gastro.2014.04.043 · doi ↗ · pubmed ↗
- 3Ramchandani M Lakhtakia S Costamagna G Fully covered self-expanding metal stent vs multiple plastic stents to treat benign biliary strictures secondary to chronic pancreatitis: a multicenter randomized trial Gastroenterology 202116118519510.1053/j.gastro.2021.03.01533741314 · doi ↗ · pubmed ↗
- 4Martins FP De Paulo GA Contini MLC Metal versus plastic stents for anastomotic biliary strictures after liver transplantation: a randomized controlled trial Gastrointest Endosc 20188713101.31E 1528455159 10.1016/j.gie.2017.04.013 · doi ↗ · pubmed ↗
- 5Tal AO Finkelmeier F Filmann N Multiple plastic stents versus covered metal stent for treatment of anastomotic biliary strictures after liver transplantation: a prospective, randomized, multicenter trial Gastrointest Endosc 2017861038104510.1016/j.gie.2017.03.00928302527 · doi ↗ · pubmed ↗