Sarcomatoid Mesothelioma With New Pancreatic Lesions Presenting As Acute Pancreatitis: A Case Report
Feras Al-Moussally, Faris Alamin, Saud Khan, Priya K Gopalan

TL;DR
This case report describes a rare instance of sarcomatoid mesothelioma metastasizing to the pancreas, presenting as acute pancreatitis in an elderly man.
Contribution
The novelty lies in documenting a rare pancreatic metastasis from sarcomatoid mesothelioma presenting as acute pancreatitis.
Findings
A 78-year-old male presented with acute pancreatitis due to metastatic sarcomatoid mesothelioma.
Pancreatic metastasis from sarcomatoid mesothelioma is extremely rare and has not been widely reported.
The case highlights the importance of considering rare metastatic sites in mesothelioma patients.
Abstract
Sarcomatoid mesothelioma is a rare, aggressive malignancy that usually follows asbestos exposure. It is the least common subtype of mesotheliomas, following epithelial and biphasic subtypes. Pleural mesothelioma can metastasize, with the liver, kidneys, adrenal glands, and opposite lungs being the most commonly reported sites for metastasis. Metastasis of the pancreas is extremely rare, which is why the authors of this case report intend to present the case of a 78-year-old male who was found to have acute pancreatitis, most likely secondary to metastatic lesions.
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
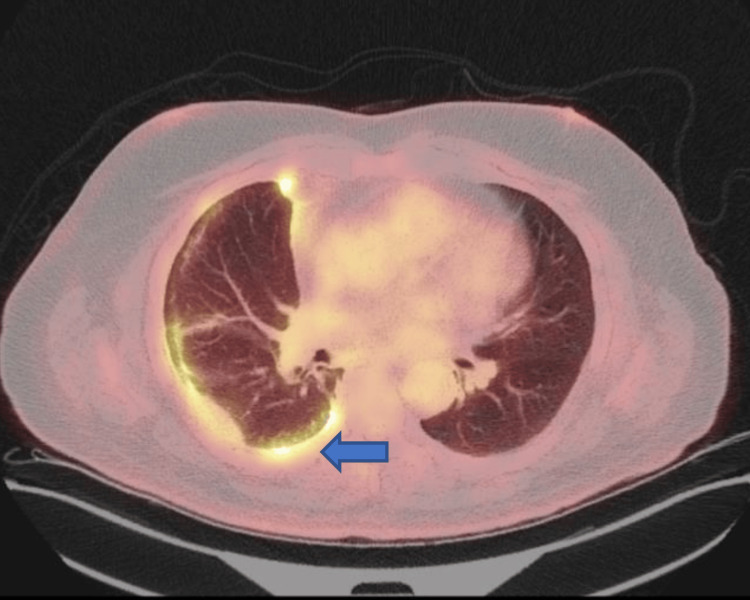 Figure 1
Figure 1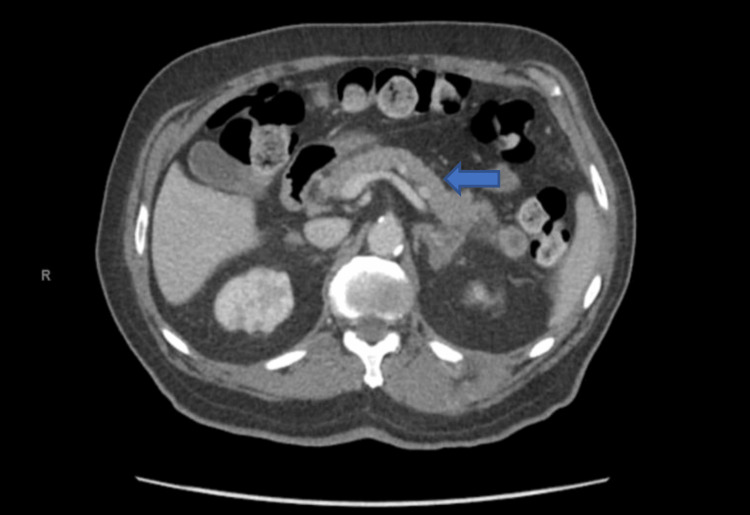 Figure 2
Figure 2| Laboratory test | Value | Reference range |
| Lipase | >1020 U/L | 8-78 U/L |
| White blood cell | 12.1 K/cmm | 4.2-10.3 K/cmm |
| Aspartate aminotransferase | 12 U/L | 5-34 U/L |
| Alanine aminotransferase | 12 UL | 10-55 U/L |
| Total bilirubin | 0.38 mg/dL | 0.16-1.25 mg/dL |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsOccupational and environmental lung diseases · Medical Imaging and Pathology Studies · Soft tissue tumor case studies
Introduction
Sarcomatoid cells are typically present in the bones, nerves, and connective tissues. Sarcomatoid mesothelioma is the rarest subtype of malignant mesothelioma with a median survival of four months with surgical treatment and 15 months with immunotherapy. It usually occurs following exposure to asbestos and is characterized by spindle cell proliferation under microscopy. Pleural mesothelioma most often metastasizes to the liver, spleen, kidneys, and adrenal glands. We intend to present a case of a 78-year-old male with a history of pleural sarcomatoid mesothelioma who presented to the emergency department with abdominal pain and was found to have acute pancreatitis likely secondary to metastatic lesions found in the neck and tail of the pancreas.
Case presentation
The patient is a 78-year-old male with a past medical history of diabetes mellitus, hyperlipidemia, benign prostatic hypertrophy, hypertension, allergic rhinitis, and remote history of possible occupational asbestos exposure, who was recently diagnosed with metastatic sarcomatoid mesothelioma (Figure 1), who came to the emergency department complaining of a three-day history of abdominal pain, nausea, and vomiting.
PET scan showing increased FDG activity in multiple foci throughout the right pleura, mostly posteriorly (arrow)PET: positron emission tomography; FDG: fluorodeoxyglucose
The patient reported that he had progressively worsening food intolerance with epigastric abdominal discomfort. He had multiple non-bloody and nonbilious vomiting episodes the day prior to the presentation. At home, the patient was taking acetaminophen 325mg three times a day, an albuterol inhaler every six hours, amlodipine 10mg once a day, docusate/sennosides 50mg/8.6mg once a day, fluticasone/salmeterol 250/50 twice a day, glipizide 5mg once a day, losartan 100mg once a day, metoprolol tartrate 25mg twice a day, oxycodone 10mg three times a day, pantoprazole 40mg once a day, and rosuvastatin 40mg once a day.
Notably, seven weeks prior to presentation, the patient underwent a biopsy of a chest wall mass which was consistent with a malignant spindle cell neoplasm, favoring sarcomatoid mesothelioma. Immunohistochemistry was positive for AE1/AE3, Cam52, OSCAR, D2-40, calretinin (weak and patchy), actin and GATA3; nonspecific for CD31, SATB2; negative for WT-1, ERG, CD34, STAT6, CK7, NKX3.1, Sox10, S100, SMMS-1, MyoD1, myogenin, CDK4, MDM2, TTF-1, p40 and Pax8; H3-trimethyl K27 nuclear expression preserved. Subsequently, he underwent right thoracotomy with resection of the chest wall mass and received palliative radiation therapy with the last session being a month prior to the presentation described.
In the emergency department, the patient was afebrile, pulse of 91 beats per minute, respiratory rate of 18 breaths per minute, and blood pressure of 158/80 mmHg. His laboratory investigation was significant for the following values in Table 1.
The patient had a computed tomography (CT) of the abdomen and pelvis which showed possible mild pancreatitis associated with new masses in the pancreatic neck and tail (Figure 2). The patient also had worsening metastatic disease involving the peritoneum, paraspinal muscle, and osseous involvement.
CT scan of the abdomen showing multiple new pancreatic metastases (arrow)
The patient was admitted to the hospital for the management of acute pancreatitis. He was initially placed on no diet and slowly progressed as tolerated, started on intravenous fluid replacement, and a pain control regimen. The patient slowly improved and was discharged home with plans to follow up with his oncologist to start the planned regimen of nivolumab and ipilimumab once acute pancreatitis resolved.
Discussion
Mesothelial tumors are divided into benign or preinvasive and mesotheliomas. The benign subgroup includes mesothelioma in situ, well-differentiated papillary mesothelial tumors, and adenomatoid tumors. Invasive mesothelioma is divided histologically into epithelial, biphasic, and sarcomatoid [1]. Epithelial subtype is the most common invasive mesothelioma subtype comprising 60% of cases, followed by biphasic which comprises 20%, and lastly, the sarcomatoid subtype is the rarest [2]. Identifying the subtype of mesothelioma is important since it impacts treatment plans and prognosis discussions [3]. The median survival in patients diagnosed with sarcomatoid mesothelioma who undergo surgical treatment is 4 months, compared to 19 months and 12 months in epithelioid and biphasic subtypes [3]. In a recent study, it was shown that the median survival for sarcomatoid mesothelioma could reach as high as 15 months with immunotherapy [2]. The worse prognosis of the sarcomatoid subtype is thought to be due to the subtype’s ability to invade the surrounding tissue, rapid growth, inconsistent expression of tumor markers, and fibrous nature [2,4].
The primary cause of sarcomatoid mesothelioma is thought to be asbestos exposure [2]. Cancer can arise after 20 years to 60 years following exposure [2]. Presenting symptoms vary but could include fatigue, anemia, anorexia, and similar to our patient, chest pain, cough, and hemoptysis [2]. It is defined as spindle cell proliferation in fascicles or haphazard patterns invading the lung parenchyma or adipose tissue [1]. Investigation studies include CDKN2A, MTAP, BAP1, cytokeratins, mesothelial markers, FLI1, CD31, ERG, CD34, STAT6, myogenin, S-100 protein, melan A, HMB45, SOX10 [1]. Pleural mesothelioma has the ability to metastasize. In fact, a study in 2012 showed more than half the patients had distant metastases with the most common site being liver, followed by adrenal glands, kidneys, and the opposite lung [2]. However, metastasis to the pancreas is extremely rare [5].
There is a chance of diagnostic inaccuracy for mesotheliomas as there are multiple dyes useful for immunohistochemistry, the combination of which is unique for different mesotheliomas, and the interpretation of these studies is subjective. Thus, it is recommended that a team of pathologists with proven experience in diagnosing mesothelioma confirm the diagnosis in cases of diagnostic uncertainty [6-7].
Conclusions
Our patient improved after the management of pancreatitis per the guidelines. He was later discharged and was planned to start immunotherapy outpatient. The authors of this case report intended to present a case highlighting the pancreas as a potential metastasis location for pleural sarcomatoid mesothelioma. In addition, metastatic disease involving the pancreas is an important differential diagnosis for acute pancreatitis.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Pleural mesothelioma classification-update and challenges Mod Pathol Dacic S 51563520223446588310.1038/s 41379-021-00895-7 · doi ↗ · pubmed ↗
- 2Deep-learning based classification distinguishes sarcomatoid malignant mesotheliomas from benign spindle cell mesothelial proliferations Mod Pathol Naso JR Levine AB Farahani H 202820353420213411295710.1038/s 41379-021-00850-6 · doi ↗ · pubmed ↗
- 3Impact of mesothelioma histologic subtype on outcomes in the Surveillance, Epidemiology, and End Results database J Surg Res Meyerhoff RR Yang CF Speicher PJ 233219620152579182510.1016/j.jss.2015.01.043PMC 4430361 · doi ↗ · pubmed ↗
- 4Sarcomatoid mesothelioma: unusual findings and literature review J Surg Case Rep Clopton B Long W Santos M Asarian A Genato R Xiao P 02022202210.1093/jscr/rjac 512PMC 967576236415726 · doi ↗ · pubmed ↗
- 5A rare case of malignant pleural mesothelioma with metastases to the pancreas concurrently diagnosed with invasive ductal adenocarcinoma Kans J Med Wuthnow C Agha YH Srinivasan S Salyers W Tofteland N 2692711320203317356410.17161/kjm.vol 13.14765 PMC 7651784 · doi ↗ · pubmed ↗
- 6Guidelines for pathologic diagnosis of malignant mesothelioma 2017 update of the consensus statement from the International Mesothelioma Interest Group Arch Pathol Lab Med Husain AN Colby TV Ordóñez NG 8910814220182868650010.5858/arpa.2017-0124-RA · doi ↗ · pubmed ↗
- 7Mesothelioma: scientific clues for prevention, diagnosis, and therapy CA Cancer J Clin Carbone M Adusumilli PS Alexander HR Jr 4024296920193128384510.3322/caac.21572 PMC 8192079 · doi ↗ · pubmed ↗