Septic cardioembolic stroke secondary to infective endocarditis in a young patient with rheumatic heart disease: a case report
Helena Agostingo Buque, Evangelina Namburete, Deise Catamo Vaz, Frederico João Sebasteão, Yanina Baduro, Elder Lorenzo Rosales, Nachan Arroz, Lazara Bacallao, Damiano Pizzol, Lee Smith

TL;DR
A young man with heart disease survived a rare stroke caused by an infection in his heart, successfully treated in a low-resource setting.
Contribution
Presents a successful treatment case of septic cardioembolic stroke in a low-resource setting.
Findings
A 24-year-old male with rheumatic heart disease developed septic cardioembolic stroke due to infective endocarditis.
The patient was successfully treated in a low-resource setting despite the high risk of complications.
The case highlights challenges in diagnosing and treating such conditions in areas with limited imaging and diagnostic resources.
Abstract
The risk of stroke due to infective endocarditis is particularly high during the first week. Moreover, in low-resource settings where imaging access is limited, and diagnostic pathways are inaccurate the risk further increases. In addition to antibiotic therapy, treatment may include intravenous thrombolysis, with high risk of hemorrhagic complications in patients with infective endocarditis or mechanical thrombectomy. We report here a case of a 24-year-old male with rheumatic heart disease presenting a septic cardioembolic stroke secondary to infective endocarditis that was successfully treated in a low-resource setting.
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
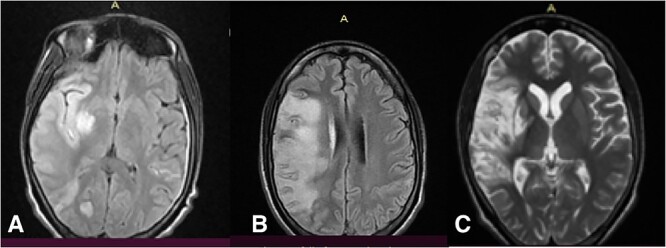 Figure 1
Figure 1Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsInfective Endocarditis Diagnosis and Management · Streptococcal Infections and Treatments · Bacterial Identification and Susceptibility Testing
Introduction
Cerebral ischemic events are among the most common presenting symptoms and a main cause of death of infective endocarditis, although stroke secondary to infections remain a rare condition [1]. Although the increase access to advanced neuroimaging allows the detection of silent early-stage cerebral embolism, clinically manifest stroke remains the classic presentation especially in low-resource settings where the imaging access is limited and diagnostic pathway often inaccurate [2]. Moreover, it is estimated that the risk of stroke due to infective endocarditis remains high (4.8/1000 patient-days) during the first week of antibiotic therapy and then declines rapidly [3]. Stroke secondary to infections is likely a result of embolism by migration of fragments vegetation and/or mycotic aneurysm rupture [1]. The main cerebrovascular complications include meningitis, intracerebral abscess, encephalopathy, hemorrhage and aneurysms with consequent high risk for intracranial bleeding [4]. In infective endocarditis the higher rate of cerebral embolic events are associated with Staphylococcus aureus when the anterior leaflet of the mitral valve is affected [5]. Interestingly, the most common location of ischemic events is the middle cerebral artery although also multifocal or distal ischemic events may occur [5]. Based on clinical and functional presentation and health general status, in addition to antibiotic therapy, treatment may include intravenous thrombolysis or mechanical thrombectomy [5].
We report here a case of a 24-year-old male with rheumatic heart disease presenting a septic cardioembolic stroke secondary to infective endocarditis that was successfully treated in a low-resource setting.
Case report
A 24-year-old male presented with sudden onset of muscle strength loss in the left hemi body, found fallen early in the morning, complaining of intense holocranial headache and fever, followed by drowsiness and hypo-responsiveness. He reported that he was attending outpatient follow-ups at the local health center for two months due to epigastric pain diagnosed as gastritis. He was previously healthy, with no smoking or alcohol habits, nor chronic diseases. He was not taking corticosteroids or other immunosuppressive medications. The examination showed drowsiness, clear and coherent speech, with gaze diverted to the right, mydriatic pupils reactive to light, deviation of the lip commissure to the left and facial asymmetry with facial paralysis to the left. Gait not assessable, with muscle strength at 1/5, with neck stiffness and preserved sensitivity. His body temperature was 38.9°C, blood pressure 90/55 mmHg, heart rate 90 bpm. A 5/6 murmur was detected in the 2^nd^ and 5^th^ intercostal space in the left mid-clavicular line, with thrill throughout the precordial area. Biochemistry revealed leukocytosis with neutrophilic predominance, moderate anemia, mild hyponatremia and hypochloremia. Malaria, HIV and Covid-19 tests were negative, but he had a positive blood culture for S. aureus, sensitive to Ceftriaxone. Cardiac ultrasound revealed carditis with vegetations on the mitral and aortic valves. Magnetic resonance imaging (MRI) showed an extensive lesion in the area of the right middle cerebral artery and occipital with extensive perilesional edema (Fig. 1A). He was first treated with Ceftiaxone 2 g twice per day, Gentamicin 160 mg/day, Mannitol 20% 80 ml each four hour, lactate ringer 2 l/day, Aspirin 100 mg/day, Simvastantin 20 mg/night, Lisinopril 5 mg/day, Paracetamol 1 g each six hours and Omeprazole 20 mg/day.
Magnetic resonance showing the cerebral lesion at admission (A) and after 14 (B) and 33 (C) days.
After 5 days of treatment, there was a clinical improvement, he was awake, cooperative, apyretic, with no neck stiffness or headache; The focal neurological deficit with left hemiparesis persisted and he started physiotherapy. On the 14^th^ day, he had improvement in muscle strength with 3/5 in the upper limb and 2/5 in the lower limb. Control MRI showed edema reduction with areas of cerebritis. (Fig. 1B). Ultrasound confirmed chronic rheumatic heart disease with severe mitral insufficiency and mild to moderate aortic insufficiency. Ceftriaxone was suspended and ciprofloxacin 500 mg twice per day was started for 14 days. On the 33^rd^ day MRI showed hypersignal in the territory of the middle cerebral artery, with rediffusion and without cerebral edema (Fig. 1C). On the 35^th^ day he was discharged with outpatient follow-up.
Discussion
The most important factor in managing cardioembolic stroke secondary to infective endocarditis is timing in terms of proper diagnosis and adequate treatment. In particular, the early administration of effective intravenous antibiotics allows to reduce mortality and morbidity from embolic complications and heart failure [5]. In the present case, the patient presented a full-blown symptomatic stroke including sudden and complete hemiparesis associated with fever, neck stiffness, altered level of consciousness and heart murmur. Such presentation raised the suspicion of cardiac involvement and, as expected, diagnosed, with subsequent MRI confirmation, a cardioembolic stroke secondary to infective endocarditis likely developed during previous weeks based on reported clinical history. On the one hand, this reiterates the lack of adequate tools for diagnosis, the lack of trained medical professionals and the absence of an effective referral system in low-resource settings. On the other hand, it significantly reduced the chances of a favorable outcome for the prognosis. In this case, ultrasound played a crucial role in diagnosis orientation, in line with previous evidence on the versatility of this diagnostic tool that can be easily employed in extremely resource-limited settings where radiological and microbiological investigations are scarce [6]. Moreover, the patient presented with large vessel occlusion and, at the time of writing, there is no consensus on the gold standard management for similar cases. Indeed, for in-patients with acute ischemic stroke treatment with intravenous thrombolysis is suggested; in patients with infective endocarditis particular attention must be paid due to the high risk of hemorrhagic complications [7]. An option to be considered for these patients could be a mechanical thrombectomy [7]. While the first option was not performed by choice, there was no possibility to consider the second option due to lack of equipment. In low-resource settings, limited equipment is common, reducing favorable prognosis [8]. Immediately, even before having confirmation of positive culture for S. aureus, the patient commenced an intravenous antibiotic therapy with Ceftriaxone and Gentamicin which proved to be lifesaving in this case. Indeed, the patient conditions improved significantly after 4–5 days of therapy institution and no complication such as heart failure or valve rupture developed.
This successful case highlights on one hand the proper management of such complicated and late-stage condition, and on the other hand the necessity to continuously train and support health professionals across low-resource settings. Onsite healthcare workers training is crucial to avoid “brain drain” as well as to avoid training on different standards of practice and ultimately to encourage a sense of belonging and professional growth. In particular, for this specific condition, a recent history of strep infection or rheumatic fever is the key to hypothesize the diagnosis of rheumatic heart disease. Moreover, symptoms of rheumatic fever vary and typically begin one to six weeks after a bout of strep throat and, in some cases, the infection may have been too mild to have been recognized, or it may be gone by the time the person sees a medical practitioner. These considerations reinforce the importance of appropriate training for health professionals especially in remote areas and make mandatory a call to action to all involved institutions to improve and increase the efforts to achieve universal health care coverage.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Thuny F, Avierinos JF, Tribouilloy C. et al. Impact of cerebrovascular complications on mortality and neurologic outcome during infective endocarditis: a prospective multicentre study. Eur Heart J 2007;28:1155–61.17363448 10.1093/eurheartj/ehm 005 · doi ↗ · pubmed ↗
- 2Baddour LM, Wilson WR, Bayer AS. et al. Infective endocarditis in adults: diagnosis, antimicrobial therapy, and Management of Complications: a scientific statement for healthcare professionals from the American Heart Association. Circulation 2015;132:1435–86.26373316 10.1161/CIR.0000000000000296 · doi ↗ · pubmed ↗
- 3Dickerman SA, Abrutyn E, Barsic B. et al. The relationship between the initiation of antimicrobial therapy and the incidence of stroke in infective endocarditis: an analysis from the ICE prospective cohort study (ICE-PCS). Am Heart J 2007;154:1086–94.18035080 10.1016/j.ahj.2007.07.023 · doi ↗ · pubmed ↗
- 4Kume Y, Fujita T, Fukushima S. et al. Intracranial mycotic aneurysm is associated with cerebral bleeding post-valve surgery for infective endocarditis. Interact Cardiovasc Thorac Surg 2018;27:635–41.29701786 10.1093/icvts/ivy 126 · doi ↗ · pubmed ↗
- 5Mowla A, Abdollahifard S, Sizdahkhani S. et al. Endovascular treatment of large vessel occlusion strokes caused by infective endocarditis: a systematic review, meta-analysis, and case presentation. Life (Basel) 2022;12:2146.36556511 10.3390/life 12122146 PMC 9780851 · doi ↗ · pubmed ↗
- 6Bobbio F, Di Gennaro F, Marotta C. et al. Focused ultrasound to diagnose HIV-associated tuberculosis (FASH) in the extremely resource-limited setting of South Sudan: a cross-sectional study. BMJ Open 2019;9:e 027179.10.1136/bmjopen-2018-027179 PMC 650028330944140 · doi ↗ · pubmed ↗
- 7Bettencourt S, Ferro JM. Acute ischemic stroke treatment in infective endocarditis: systematic review. J Stroke Cerebrovasc Dis 2020;29:104598.32024600 10.1016/j.jstrokecerebrovasdis.2019.104598 · doi ↗ · pubmed ↗
- 8Muhelo A, Zita A, Seni A. et al. Successful management of generalized tetanus in a 12-year old girl without anti-tetanus immunoglobulins: a case report. Oxf Med Case Rep 2022;2022:omac 098.10.1093/omcr/omac 098PMC 951410236176952 · doi ↗ · pubmed ↗