Descriptive study of the oral health status of disadvantaged mexican populations in relation to their adherence to the mediterranean diet
Javier Flores-Fraile, Sergio Parra-García, Diego González-Gil, Alejandro Moreno-Barrera, Alejandra Peramato-Benito, Antonio Castaño-Seiquer

TL;DR
This study explores how dietary habits, especially adherence to the Mediterranean diet, affect oral health in a disadvantaged Mexican population.
Contribution
The study investigates the link between oral health-related quality of life and Mediterranean diet adherence in a specific Mexican population.
Findings
Low adherence to the Mediterranean diet correlates with higher caries prevalence.
The average OHIP-14Sp score indicates moderate oral health-related quality of life.
The study highlights the interplay between diet, obesity, and oral health.
Abstract
Background: Obesity in Mexico is an alarming problem that has been increasing in recent decades. Dietary factors make this pathology more common at younger ages and closely related to oral health. This study attempts to investigate the association between the oral health status of a Mexican population in the state of Yucatan and their dietary habits. Objective: This study explores the relationship between oral health-related quality of life and adherence to the Mediterranean diet in a disadvantaged population in the state of Yucatan, Mexico. Methods: The research was conducted in July 2023 in Merida, Yucatan (Mexico). The sample consisted of 109 individuals aged between 4 and 72 years old. Data analysis focused on factors such as body mass index (BMI), oral health-related quality of life, and adherence to the Mediterranean diet. Results: A notable presence of caries is observed in…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
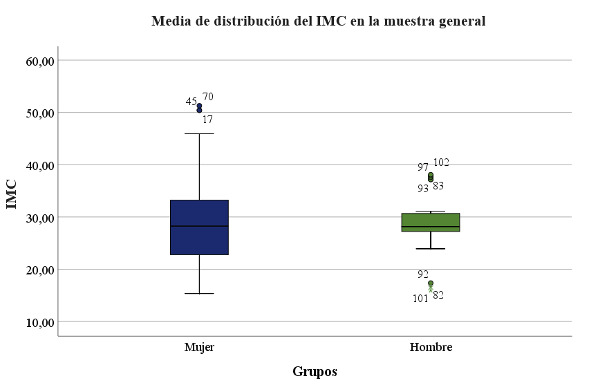 Figure 1
Figure 1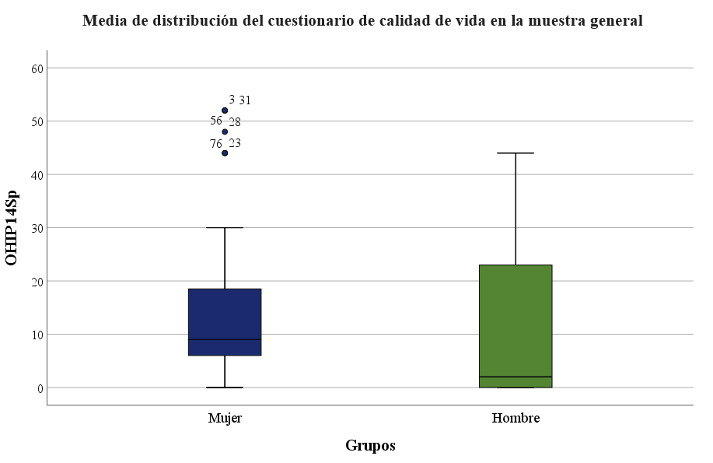 Figure 2
Figure 2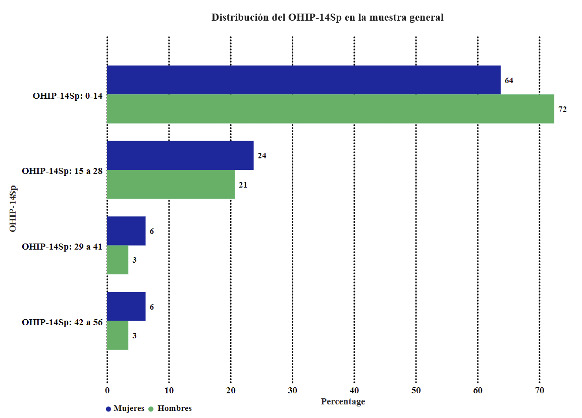 Figure 3
Figure 3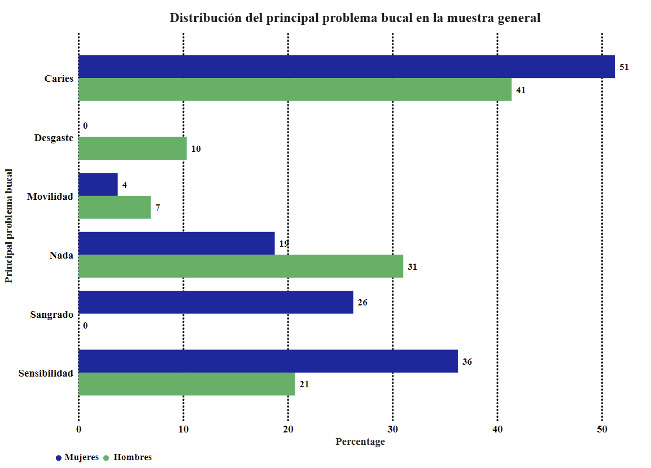 Figure 4
Figure 4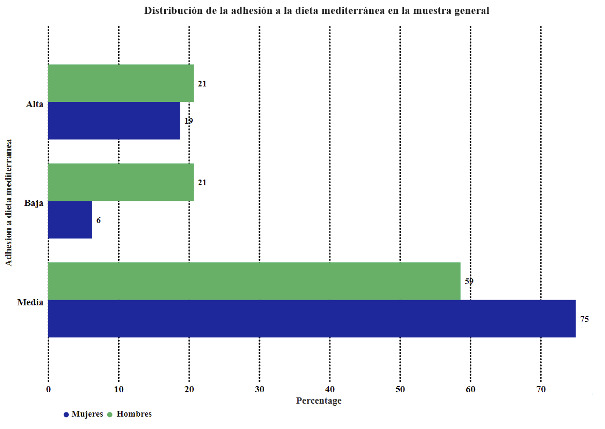 Figure 5
Figure 5Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsDental Health and Care Utilization · Oral microbiology and periodontitis research · HIV/AIDS oral health manifestations
INTRODUCTION
Oral health is a dynamic state influenced not only by hygiene and dietary habits, but also by the absence of oral and systemic diseases 1^,^2. Currently, oral cavity diseases present a high prevalence and incidence, significantly impacting the perceived quality of life and daily functioning of individuals due to factors such as pain, inflammation, and functional limitations 3^-^6.
Over 70% of the population presently experiences some form of oral pathology, defined as deviations from ideal oral health, including complete dentition, absence of pathology, proper dental and intermaxillary relationships, and optimal morpho-functional parameters, all of which can variably affect systemic health. This prevalence is notably higher in underdeveloped or developing countries despite basic dental care being provided by the National Health System 6^,^7. In Mexico, for example, epidemiological data suggests a prevalence of oral pathology exceeding 90%, reflecting both a local and broader socio-health issue. This research specifically focuses on the Yucatan region, serving as a microcosm whose oral and systemic pathology statistics can be extrapolated nationally 8^-^11.
Numerous oral diseases stem from unhealthy dietary habits, with the Mediterranean diet serving as a reference model 12^-^18. These oral diseases present significant public health challenges, resulting in pain, social consequences, and functional limitations. Globally, nine out of ten individuals are at risk of experiencing such issues 19^-^23.
Mexico is among countries with a high prevalence of oral diseases, with caries affecting over 90% of its population. It is important to note that the Universal Catalog of Health Services (CAUSES) provides medical coverage, including dental specialties 24^,^25.
Focusing on the Yucatan region, the General Directorate of Epidemiology data indicates oral disease rates in 2019 comparable to national averages and significantly lower than those observed in other North American or European nations 26.
Obesity in Mexico is a growing concern, driven by socio-cultural and dietary factors, despite governmental efforts to promote healthy lifestyles and their impact on quality of life. This issue is closely related to oral health, as optimal oral health facilitates efficient initial digestive processes such as chewing, bolus formation, and swallowing 27^-^29.
This study aims to investigate the association between oral health status and adherence to the Mediterranean diet in a disadvantaged Mexican population in the state of Yucatan.
MATERIAL AND METHODS
Type of study and characteristics.
An observational, cross-sectional, and descriptive study was conducted as part of the "Odontólogo Residente Internacional" course at two health centers in the city of Mérida, in the state of Yucatán, Mexico, in July 2023.
The study adhered to the principles outlined in the Declaration of Helsinki and obtained approval from an Ethics Committee (protocol code 03/2018, approved in August of 2018). Informed consent was obtained from all participants, as well as from parents or legal guardians if applicable. The study followed STROBE guidelines.
The sample comprised 109 patients who attended routine check-ups at public health centers without prior knowledge of the data collection to prevent bias. Participants ranged in age from 4 to 72 years. They voluntarily sought dental and medical care and were provided detailed oral explanations before signing an informed consent form. Subsequently, they completed a research dossier covering questions about their oral and dental health, medical history, adherence to a Mediterranean diet, body measurements, and socioeconomic status, although the latter was not directly relevant to the investigation's primary objective.
All patients underwent examination by the same clinical examiner using a consistent methodology to minimize bias. Data collection was performed by a single experienced dentist specializing in prosthesis assessment. Intra-observer calibration was conducted to assess the consistency of observations, yielding a Kappa test agreement ratio of 0.85.
Measurement of variables
The study examined the following variables: gender, body mass index (BMI), oral quality of life, and the presence of dental caries. Gender was the main variable of interest.
The diet was evaluated using an oral quality of life and nutritional habits questionnaire OHIP-14Sp.
These variables were collected during voluntary dental exams at the "International Resident Dentist" campaign site. The same examiner recorded and transcribed the data to create a validated research dossier.
Statistical analysis.
The qualitative and quantitative variables were analyzed using the statistical software NCSS277/GESS2006. Descriptive and inferential statistics were be employed, including cross-tabulation analysis, Fisher's exact test, Chi-square test, Student's t-test, Pearson correlation test, and multivariate analysis. A significance level of p < 0.05 was accepted as statistically significant.
All data was collected in a Microsoft Excel v.16 (2020) database for subsequent analysis.
RESULTS
Age
The mean age was 35.53 years, SD ±19.58, median 37.00, range 4-72.
Table 1 displays the age in the study groups, with no significant differences found (p=0.544).
Table 1. Age in the study groups.GroupMeanSDMedianRangeFemale Group39.9518.8138.004-72Male Group34.3821.8532.005-66
3.2. Body Mass Index.
The mean body mass index (BMI) was 29.16, SD ±7.56, median 28.14, range 15.36-51.28.
Table 2 and Figure 1 show the distribution of body mass index in the study groups. There were no significant differences observed (p=0.739).
Table 2. Body Mass Index in Study Groups.GroupMeanSDMedianRangeFemales Group29.298.0928.2415.36-51.28Males Group28.805.9628.1415.97-38.09
Figure 1. Mean Body Mass Index in Study Groups.
3.3 Oral Health-Related Quality of Life (OHIP-14Sp).
The mean Oral Health-Related Quality of Life (OHIP-14Sp) score was 13.19, SD ±13.57, median 8.00, range 0-52.
Figure 2 and Table 3 display the measurement of Oral Health-Related Quality of Life (OHIP-14Sp) in the study groups, which was higher in the female group with significant differences (p=0.028).
Table 3. Oral Health-Related Quality of Life (OHIP-14Sp) in the study groups.GroupMeanSDMedianRangeFemale Group14,1513,399,000-52Male Group10,5513,982,000-44
Figure 2. Mean Oral Health-Related Quality of Life (OHIP-14Sp) in the study groups.
Table 4 and Figure 3 compare Oral Health-Related Quality of Life (OHIP-14Sp) in the study groups.
Table 4. Comparison of Oral Health-Related Quality of Life (OHIP-14Sp) in the study groups.GroupsFemales, Males, Total, n= 80 n= 29 n=109 OHIP-14SpN%n%N%p-valueOHIP-14Sp: 0-145163.752172.417266.060.4948OHIP-14Sp: 15 - 281923.75620.692522.940.8026OHIP-14Sp: 29 - 4156.2513.4565.501.0000OHIP-14Sp: 42 - 5656.2513.4565.501.0000
Figure 3. Distribution of Oral Health-Related Quality of Life (OHIP-14Sp) in the study groups.
3.4. Primary oral issue.
Table 5 and Figure 4 compare the primary oral issue in the study groups.
Table 5. Comparison of the primary oral issue in the study groups.GroupsFemales, n= 80 Males, n= 29 Total, n=109 Primary oral issuen%n%N%p-valueNothing1518.75931.032422.020.1956Caries4151.251241.385348.620.3932Sensibility2936.25620.693532.110.1649Mobility33.7526.9054.590.6074Bleeding21262500.002119.270.0008Wear00.00310.3432.750.0174
Figure 4. Distribution of the primary oral issue in the study groups.
3.5. Adherence to the Mediterranean diet.
Table 6 and Figure 5 compare the study groups' adherence to the Mediterranean diet.
Table 6. Comparison of adherence to the Mediterranean diet in the study groups.GroupsFemales, n= 80 Males, n= 29 Total, n=109 Adherence to the Mediterranean dietn%N%N%p-valueHigh1518.75620.692119.270.7899Medium6075.001758.627770.640.1520Low56.25620.691110.090.0645
Figure 5. Distribution of adherence to the Mediterranean diet in the study groups.
DISCUSSION
The Oral Health Impact Profile (OHIP) questionnaire comprises 14 questions to assess the limitations and effects of an individual's oral health status, including existing oral pathologies. It aims to evaluate the importance of oral health in a person's quality of life. In the case of obesity type 1, lower scores were obtained compared to obesity types 2 and 3, highlighting how obesity affects an individual’s quality of life and daily performance and influences oral health. For instance, a study by Dibello 30 in 2023 observed a correlation between high OHIP scores and eating disorders and obesity in elderly individuals in Italy 31 study directly links obesity to poor oral health, with dry mouth being one of the effects. However, research conducted by Tengku in 2021 on 400 obese and normal-weight individuals showed no significant impact of obesity on oral health.
Based on the information above, it is evident that further research is required to fully understand the link between high BMI and poor oral health. However, there is evidence to suggest a definite relationship between the two, and it appears that they impact each other, with an increase in either having adverse effects on an individual 32.
This impact is more pronounced as individuals age, with little to no noticeable difference among young people. This could be attributed to the aging process exacerbating the impact of obesity on oral health and the chronic nature of obesity and its duration in relation to oral health. It makes sense as obesity-related inflammation is mild and prolonged, leading to adverse effects over time rather than due to its intensity.
Additionally, the severity of obesity is directly related to its impact on oral health, with higher obesity rates likely linked to more significant discomfort and lower oral health-related quality of life.
The Mediterranean diet is a dietary pattern followed by countries and populations bordering the Mediterranean Sea. This diet is characterized by low consumption of meats and carbohydrates compared to, for example, an American diet and a notable increase in vegetable consumption. The benefits of the Mediterranean diet include better glycemic control, lower triglycerides, and a reduced risk of cardiovascular diseases and other health problems, such as cancer 33.
In a recent study, participants completed a validated questionnaire on adherence to the Mediterranean diet with 17 questions with "yes" or "no" responses. Each response scored one point for greater compliance with Mediterranean diet parameters or zero points for lesser compliance, with a maximum score of 17 indicating total adherence to the Mediterranean diet and zero indicating the most remarkable difference from this dietary pattern.
The study results showed that the sample had a mean score of 7.57, a median score of 7, and a few subjects achieving a maximum score of 10. An inverse association was found, with lower adherence to the Mediterranean diet and lower scores linked to a significant increase in BMI and waist circumference. This result supports other studies correlating the Mediterranean diet with life expectancy, quality of life, and obesity. Researchers like the Carbajal group and collaborators have shown how the traditional Mediterranean diet is being adapted to modern times to make it even more efficient regarding current food supply and availability, maintaining and enhancing its health and weight control benefits 34. According to research conducted by the Schröder group, adopting the Mediterranean diet can regulate body weight, prevent obesity, and act as a protective factor against both type 1 and type 2 diabetes, with the latter being directly linked to obesity 35. A 2019 review also confirms the benefits of the Mediterranean diet in controlling body weight, preventing diseases, and promoting a lifestyle linked to increased life expectancy and quality of life 36. The disparity between the lifestyle of the population in the state of Yucatan and the Mediterranean diet standards is significantly associated with the high rates of obesity in the region.
CONCLUSION
The low adherence of the evaluated population to the Mediterranean diet is associated with a high prevalence of caries and a high body mass index, indicating an opportunity for improvement in quality of life.
It is necessary to conduct studies with a larger population to assess other dietary factors associated with obesity and their impact on oral health status.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Peres MA Macpherson LMD Weyant RJ Daly B Venturelli R Mathur MR Listl S Celeste RK Guarnizo-Herreño CC Kearns C Benzian H Allison P Watt RG Oral diseases a global public health challenge Lancet 20193941019424926010.1016/S 0140-6736(19)31146-831327369 · doi ↗ · pubmed ↗
- 2Kassebaum NJ BernabéE Dahiya M Bhandari B Murray CJ Marcenes W Global burden of untreated caries a systematic review and metaregression J Dent Res 201594565065810.1177/002203451557327225740856 · doi ↗ · pubmed ↗
- 3Bernabe E Marcenes W Hernandez CR Bailey J Abreu LG Alipour V Global, Regional, and National Levels and Trends in Burden of Oral Conditions from 1990 to 2017 AA 10.1177/0022034520908533 PMC 708832232122215 · doi ↗ · pubmed ↗
- 4Kassebaum NJ Smith AGC BernabéE Fleming TD Reynolds AE Vos T Murray CJL Marcenes W GBD 2015 Oral Health Collaborators Global, Regional, and National Prevalence, Incidence, and Disability-Adjusted Life Years for Oral Conditions for 195 Countries, 1990-2015: A Systematic Analysis for the Global Burden of Diseases, Injuries, and Risk Factors J Dent Res 201796438038710.1177/002203451769356628792274 PMC 5912207 · doi ↗ · pubmed ↗
- 5Manohar N Hayen A Fahey P Arora A Obesity and dental caries in early childhood A systematic review and meta-analyses Obes Rev 2020213 e 1296010.1111/obr.1296031721413 · doi ↗ · pubmed ↗
- 6Manton DJ Child Dental Caries - A Global Problem of Inequality E Clinical Medicine 201813410.1016/j.eclinm.2018.06.00631193614 PMC 6537533 · doi ↗ · pubmed ↗
- 7Henshaw MM Karpas S Oral Health Disparities and Inequities in Older Adults Dent Clin North Am 202165225727310.1016/j.cden.2020.11.00433641752 · doi ↗ · pubmed ↗
- 8Organización Mundial de la Salud Normas para la Identificacion y Definicion de Problemas Dentales; Informe de un Comité de Expertos en Higiene Dental Ginebra, Switzerland 1962