Case Report: Diabetic ketoacidosis after co-administration of empagliflozin and probenecid
William P. Martin, Niamh Reidy, Justin Low, Tomás Ahern, Prashant Nasa, William Martin, Simeon I Taylor, Zhinous Shahidzadeh Yazdi, William Martin

TL;DR
A patient with type 2 diabetes developed severe diabetic ketoacidosis after taking empagliflozin and probenecid together, likely due to a drug interaction.
Contribution
The paper identifies a pharmacokinetic interaction between empagliflozin and probenecid via OAT3 that increases DKA risk.
Findings
Co-administration of empagliflozin and probenecid may reduce empagliflozin secretion in the kidney.
This interaction could increase empagliflozin exposure and raise the risk of diabetic ketoacidosis.
Clinicians should be cautious when prescribing OAT3 inhibitors with empagliflozin.
Abstract
Sodium-glucose cotransporter-2 (SGLT2) inhibitors are filtered and secreted to their primary site of action in the proximal tubule of the kidney. Many commonly used medications have potential to diminish renal elimination of SGLT2 inhibitors by inhibiting their tubular secretion. We present a case of severe diabetic ketoacidosis (DKA) in a patient with type 2 diabetes occurring several days after co-prescription of empagliflozin and probenecid. Other than the recent introduction of empagliflozin, no cause for the DKA episode was apparent. A pharmacokinetic interaction between probenecid and empagliflozin, involving organic anion transporter 3 (OAT3), reduces proximal tubular secretion of empagliflozin. Co-administration of an OAT3 inhibitor, such as probenecid, with empagliflozin may increase patient exposure and diminish glucosuric response to the SGLT2 inhibitor, thereby increasing…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
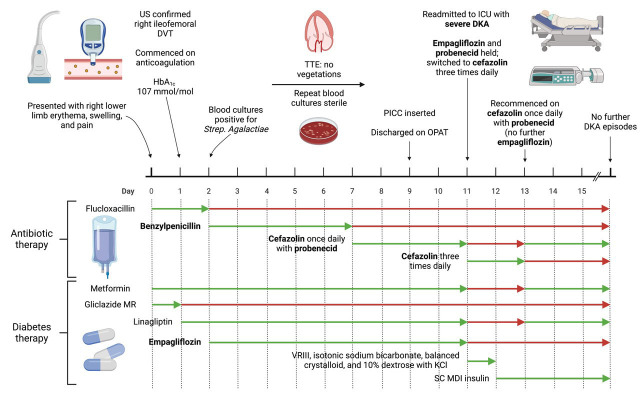 Figure 1
Figure 1- —Wellcome Trust
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsDiabetes Treatment and Management · Pancreatic function and diabetes · Pancreatitis Pathology and Treatment
Introduction
Sodium-glucose cotransporter-2 (SGLT2) inhibitors are strongly recommended for patients with type 2 diabetes in the latest clinical practice guidelines based on their demonstrated cardiovascular and renal benefits ^ 1 ^. Nevertheless, these medications increase the risk of diabetic ketoacidosis (DKA) ^ 2, 3 ^, a severe acute complication of diabetes which carries a substantial risk of morbidity and mortality ^ 4 ^.
SGLT2 inhibitors are both filtered and secreted to their primary site of action in the proximal tubule of the kidney ^ 5 ^. Although many commonly prescribed medications have the potential to diminish renal elimination of SGLT2 inhibitors by inhibiting their proximal tubular secretion, these interactions are not recognised to increase the risk of DKA nor other side effects of SGLT2 inhibitors and do not influence routine prescription of these medications. We present a case of severe DKA in a patient with type 2 diabetes occurring several days after co-prescription of the SGLT2 inhibitor empagliflozin alongside probenecid, an inhibitor of organic anion transporter 3 (OAT3) ^ 6 ^, a transporter which plays a key role in the secretion of empagliflozin into the proximal tubule ^ 5 ^.
Case report
A 54-year-old woman with obesity (body-mass index 39.5 kg/m ^2^) and type 2 diabetes mellitus (T2DM, diagnosed 7 years ago) presented to our hospital with a one-week history of right leg redness, swelling, and pain ( Figure 1). There was a family history of type 1 diabetes mellitus (T1DM) diagnosed at 8 years of age in a maternal first cousin and of T2DM diagnosed in a maternal uncle in his mid-50s. The patient lived alone, was independent in activities of daily living, drank alcohol rarely on social occasions, and was a lifelong non-smoker. On examination, the patient had a heart rate of 118 beats per minute (sinus tachycardia on an electrocardiogram), respiratory rate of 19 breaths per minute, blood pressure of 141/91 mmHg, peripheral oxygen saturations of 100% on room air, and a temperature of 38.8 degrees Celsius. Erythema, swelling, and tenderness of the entire right lower limb was noted. Examination of the cardiovascular, respiratory, and abdominal systems was unremarkable.
Overview of patient presentation and management, outlining timing of emergence of diabetic ketoacidosis after co-administration of empagliflozin and probenecid.Created with BioRender.com. DKA, diabetic ketoacidosis; DVT, deep vein thrombosis; HbA 1c, glycated haemoglobin; ICU, intensive care unit; KCl, potassium chloride; MDI, multiple daily injection; MR, modified release; OPAT, outpatient parenteral antibiotic therapy; PICC, peripherally inserted central catheter; SC, subcutaneous; TTE, transthoracic echocardiogram; VRIII, variable rate intravenous insulin infusion. Figure 1 was created with BioRender.com.
Ultrasound imaging confirmed the presence of a right iliofemoral deep vein thrombosis. The blood glycosylated haemoglobin level was 107 mmol/mol. Streptococcus agalactiae was cultured in peripheral blood samples. No evidence of infective endocarditis was present on transthoracic echocardiography. The patient was anticoagulated with enoxaparin 1 mg/kg (90 mg) twice daily subcutaneously initially, and later transitioned to apixaban 5 mg twice daily orally. Metformin therapy was continued at a dose of 850 mg three times daily orally, modified release gliclazide 120 mg once daily orally was stopped, and linagliptin 5 mg once daily orally and empagliflozin 10 mg once daily orally were commenced to improve glycaemic control.
The Streptococcus agalactiae isolate tested susceptible to penicillin, and treatment with intravenous high dose benzylpenicillin 2.4 g four times daily was commenced with good clinical effect. The source of bacteraemia was unclear; however, given the presence of a deep vein thrombosis, this was presumed to be infected. Blood C-reactive protein and neutrophil count values decreased during her inpatient stay (196 to 33 mg/L and 10.6 to 5.7 x10 ^9^/L, respectively). Prior to discharge, a peripherally inserted central catheter was placed and the antibiotic regimen was switched to intravenous cefazolin (2 g once daily) with oral probenecid (1g once daily) to facilitate a 6-week antibiotic course via the outpatient parenteral antibiotic therapy service.
The patient was readmitted 48 hours later with severe DKA. The patient’s infection was well controlled at the point of readmission with DKA. The patient had received the prescribed cefazolin via the outpatient parenteral antibiotic therapy service after hospital discharge. The patient also reported good compliance with prescribed medications, including oral hypoglycaemics, after hospital discharge. Nevertheless, venous blood gas results included: pH 6.87; bicarbonate 3.6 mmol/L; anion gap 30.4 mmol/L; and glucose 15.8 mmol/L. The blood ketone level was 4.3 mmol/L. The patient was treated with a variable rate intravenous insulin infusion, which was prepared by adding 50 units of Actrapid human soluble insulin to 49.5 mL of 0.9% sodium chloride and administered at insulin infusion rates of 0.5 - 8mL/hour. Intravenous isotonic sodium bicarbonate 1.26%, balanced crystalloid (Hartmann’s solution), and 10% dextrose with potassium chloride were also administered as per institutional protocol. Subcutaneous insulin therapy was commenced when the DKA resolved: insulin detemir (Levemir ^®^) 10 units twice daily and insulin aspart (Fiasp ^®^) 8 units three times daily with meals. Metformin 500 mg twice daily orally and linagliptin 5 mg once daily orally were recommenced 48 hours after readmission, with the metformin uptitrated to 1 g twice daily after one week.
At the point of readmission with severe DKA, and after having commenced systemic anticoagulation for the deep venous thrombosis, the patient reported vaginal bleeding and an ulcerated vulval lesion was noted on physical examination. Biopsies later confirmed the presence of a squamous cell carcinoma, which was staged as IVB disease on the basis of inguinal and pelvic sidewall lymphadenopathy and bone metastases present on staging scans. The vulval cancer is likely to have contributed to formation of the deep vein thrombosis as well as serving as a source of entry of Streptococcus agalactiae into the bloodstream ^ 7 ^.
However, the occurrence of DKA within several days of co-prescription of empagliflozin and probenecid implicates interaction between these medications rather than other factors such as infection or malignancy as the primary cause of the severe DKA observed in this case, particularly as the infection was well controlled at the time of readmission with DKA. Furthermore, testing for T1DM sent after readmission with DKA, including an islet autoantibody screen and urinary C-peptide to creatinine ratio, was not consistent with an underlying diagnosis of T1DM. Specifically, antibodies to zinc transporter 8, islet antigen 2, and glutamic acid decarboxylase were negative and the 2-hour post-prandial urinary C-peptide to creatinine ratio was 3.51 nmol/mmol, indicative of substantial endogenous insulin secretion.
Discussion
Other than the introduction of empagliflozin 9 days prior, no cause for the severe DKA episode described in this case was apparent. SGLT2 inhibitors are recognised to increase risk of DKA. A meta-analysis of 39 randomised clinical trials highlighted that SGLT2 inhibitors double the risk of DKA in people with T2DM ^ 2 ^. This risk is higher in elderly patients and those using SGLT2 inhibitors for longer periods of time ^ 2 ^, neither of which applied in the current case. Whilst SGLT2 inhibitors substantially increase risk of DKA in patients with T1DM ^ 3 ^, as outlined above, further evaluation for T1DM after readmission with DKA was negative in the present case. Thus, additional factors are likely to have contributed to the SGLT2 inhibitor associated DKA occurring in the context of T2DM described herein.
Empagliflozin reaches its primary site of action in the proximal tubule by a combination of glomerular filtration and tubular secretion by transporters including OAT3, which is expressed on the basolateral membrane of the proximal tubule ^ 6 ^. Probenecid inhibits OAT3 ^ 6 ^, with this property underlying its use alongside cefazolin in the present case. By diminishing renal cefazolin secretion, sufficient circulating cefazolin concentrations are achieved with once daily dosing.
In a pharmacokinetic study in healthy volunteers, co-administration of probenecid and empagliflozin, at the same total daily doses as those in the present case (1 g and 10 mg, respectively), resulted in a 26% increase in peak empagliflozin plasma concentrations and a 53% increase in area under the concentration-time curve ^ 6 ^. These findings were not felt to be clinically meaningful ^ 6 ^. However, the impact of this pharmacokinetic interaction between empagliflozin and probenecid has not been studied in patients with T2DM. In the present case, co-administration of empagliflozin and probenecid preceded immediately a presentation with DKA with no other apparent cause. Moreover, both benzylpenicillin and cefazolin, antibiotics administered to this patient while she was receiving empagliflozin, are OAT3 inhibitors and likely contributed to enhanced empagliflozin exposure ^ 8, 9 ^. Aside from increased circulating concentrations, mice with genetic knockout of OAT3 had a diminished glucosuric response to empagliflozin despite comparable tubular secretion of the drug to wild-type controls ^ 5 ^.
Thus, we suggest that clinicians exercise caution when co-prescribing empagliflozin and probenecid, or indeed other inhibitors of proximal tubular organic anion transporters, which will increase patient exposure and/or diminish glucosuric response to empagliflozin. A similar interaction may be relevant to dapagliflozin, which is also a substrate of OAT3 ^ 10 ^.
Consent
Written informed consent for publication of their clinical details was obtained from the patient.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Davies MJ Aroda VR Collins BS : Management of Hyperglycemia in Type 2 Diabetes, 2022. A Consensus Report by the American Diabetes Association (ADA) and the European Association for the Study of Diabetes (EASD). Diabetes Care. 2022;45(11):2753–2786. 10.2337/dci 22-0034 36148880 PMC 10008140 · doi ↗ · pubmed ↗
- 2Liu J Li L Li S : Sodium-glucose co-transporter-2 inhibitors and the risk of diabetic ketoacidosis in patients with type 2 diabetes: A systematic review and meta-analysis of randomized controlled trials. Diabetes Obes Metab. 2020;22(9):1619–27. 10.1111/dom.14075 32364674 · doi ↗ · pubmed ↗
- 3Danne T Garg S Peters AL : International Consensus on Risk Management of Diabetic Ketoacidosis in Patients With Type 1 Diabetes Treated With Sodium–Glucose Cotransporter (SGLT) Inhibitors. Diabetes Care. 2019;42(6):1147–54. 10.2337/dc 18-2316 30728224 PMC 6973545 · doi ↗ · pubmed ↗
- 4Gibb FW Teoh WL Graham J : Risk of death following admission to a UK hospital with diabetic ketoacidosis. Diabetologia. 2016;59(10):2082–7. 10.1007/s 00125-016-4034-0 27397023 PMC 5016550 · doi ↗ · pubmed ↗
- 5Fu Y Breljak D Onishi A : Organic anion transporter OAT 3 enhances the glucosuric effect of the SGLT 2 inhibitor empagliflozin. Am J Physiol Renal Physiol. 2018;315(2):F 386–F 94. 10.1152/ajprenal.00503.2017 29412698 PMC 6139528 · doi ↗ · pubmed ↗
- 6Macha S Koenen R Sennewald R : Effect of gemfibrozil, rifampicin, or probenecid on the pharmacokinetics of the SGLT 2 inhibitor empagliflozin in healthy volunteers. Clin Ther. 2014;36(2):280–90.e 1. 10.1016/j.clinthera.2014.01.003 24491572 · doi ↗ · pubmed ↗
- 7Graux E Hites M Martiny D : Invasive group B Streptococcus among non-pregnant adults in Brussels-Capital Region, 2005-2019. Eur J Clin Microbiol Infect Dis. 2021;40(3):515–23. 10.1007/s 10096-020-04041-0 32944894 PMC 7498195 · doi ↗ · pubmed ↗
- 8Takeda M Babu E Narikawa S : Interaction of human organic anion transporters with various cephalosporin antibiotics. Eur J Pharmacol. 2002;438(3):137–42. 10.1016/s 0014-2999(02)01306-7 11909604 · doi ↗ · pubmed ↗