Prevalence and Resistance Profiles of Pediatric Enterococcal Isolates: A Five-Year Update from Children's Medical Center Hospital, Tehran
Bahram Nikmanesh, Sajjad Yazdansetad, Mona Konkori, Mehrzad Sadredinamin, Zohreh Ghalavand, Neda Yousefi Nojookambari

TL;DR
This study analyzed antibiotic resistance in enterococcal bacteria from pediatric patients in Tehran over five years, finding high resistance to gentamicin and vancomycin.
Contribution
The study reports the highest VRE prevalence in Iranian pediatric patients and identifies linezolid-insensitive VRE cases.
Findings
87.4% of isolates were high-level gentamicin-resistant (HLGR), and 49.3% were vancomycin-resistant enterococci (VRE).
Inpatient isolates showed twice the resistance to ampicillin, penicillin, and vancomycin compared to outpatient isolates.
2% of VRE isolates were not susceptible to linezolid, and nitrofurantoin showed 92.5% susceptibility against urine isolates.
Abstract
In this study, attempts were made to evaluate the frequency of high-level gentamicin-resistant (HLGR) and vancomycin-resistant enterococci (VRE) and the prevalence and antibiotic resistance profile of enterococcal species isolated from pediatric patients referred to Children's Medical Center Hospital, Tehran, over five years. A total of 404 enterococcal isolates from different patients referred to the Children's Medical Center between March 2016 and March 2021 were included in this cross-sectional study. Antimicrobial susceptibility testing was performed using standard methods according to the guidelines of the Clinical Laboratories Standards Institute (CLSI). Approximately one-third of the enterococcal strains were isolated from urology and intensive care units. 17.3% of the isolates were obtained from outpatient sources. However, 82.7% of the isolates were sourced from inpatient…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
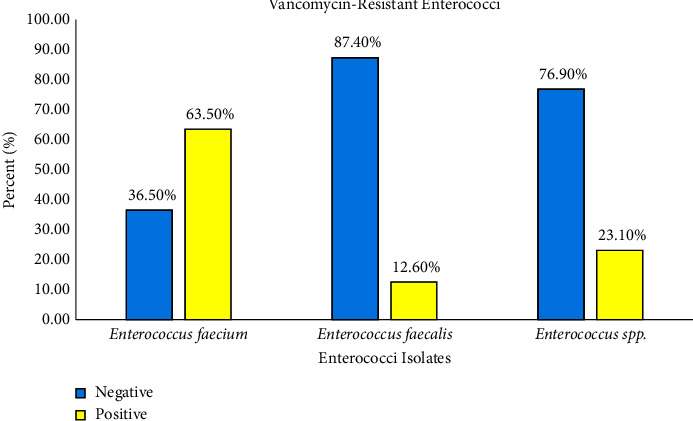 Figure 1
Figure 1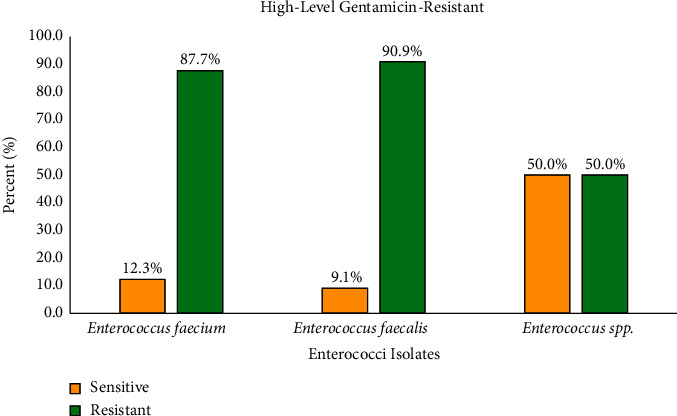 Figure 2
Figure 2Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsAntimicrobial Resistance in Staphylococcus · Streptococcal Infections and Treatments · Bacterial Identification and Susceptibility Testing
1. Introduction
Enterococcus species, particularly Enterococcus faecalis and Enterococcus faecium, are common opportunistic bacteria found in the human gastrointestinal (GI) tract, vagina, and oral cavity. They can cause severe infections in individuals under specific conditions [1]. Any disruption in the host/commensal balance that weakens the host defense system or environmental factors, such as the use of antibiotics that inadvertently promote the growth of resistant enterococci, can lead to life-threatening enterococcal infections [2]. In recent decades, enterococci have become significant nosocomial pathogens and are frequently isolated from serious hospital-acquired infections, including infective endocarditis (IE); urinary tract infections (UTIs); bacteremia; nosocomial meningitis; and intraabdominal, wound, and pelvic infections [3].
Enterococci, although not typically highly virulent, pose a significant challenge in clinical settings due to their high resistance to antimicrobial agents [4]. The intrinsic resistance of these bacteria, along with their ability to acquire additional resistance mechanisms and to thrive in hospital environments, complicates the treatment of enterococcal infections [5]. The rise of high-level aminoglycoside resistance (HLAR) and vancomycin-resistant enterococci (VRE) in clinical isolates is a growing global concern, leading to more severe infections and posing serious health risks [6, 7]. The increasing prevalence of HLAR and VRE isolates in areas such as Iran has alerted healthcare professionals, requiring strict infection control measures and presenting complex treatment challenges for clinicians. Actions to combat the spread of resistant enterococci strains are essential for maintaining public health and ensuring effective patient care [8–11].
The prevalence and impact of drug-resistant enterococcal infections among pediatric patients remain inadequately understood, despite extensive research in adult populations. This knowledge gap underscores the importance of investigating the epidemiology and antibiotic resistance profiles of enterococcal isolates in children. The current study sought to address this gap by evaluating the prevalence and resistance patterns of enterococcal infections in pediatric populations for five years.
2. Materials and Methods
2.1. Patients and Clinical Specimens
The present cross-sectional study was carried out on children with any obvious enterococcal infection referred to the Children's Medical Center Hospital in Tehran from March 2016 to March 2021. Various clinical samples were collected from outpatients and inpatients (hospitalized patients). In our study, UTI was defined as an infection of the urinary tract with 10^4^ CFU of cultured enterococci in urine and at least one UTI symptom, such as fever or urinary frequency. Only one isolate per patient was included in the study. The patients' personal and clinical information was recorded, including age, sex, length of hospital stay, time and ward of strain isolation, and microbiological data.
2.2. Identification of Enterococcal Isolates
Standard conventional biochemical tests for the identification of isolates were performed on colonies from the primary cultures. For this purpose, all suspected colonies of Enterococcus spp. were examined using Gram staining and further identified using the catalase test, hemolysis examination, bile-esculin agar, and growth in 6.5% NaCl. The isolates were stored at −70°C in trypticase soy broth containing 10% glycerol for later analysis.
2.3. Detection of HLGR and VRE Isolates
HLGR was detected using an agar-screening method. In brief, 10 μL of bacterial suspension adjusting to 0.5 McFarland turbidity standard was spotted on a brain-heart infusion (BHI) agar plate (HiMedia, India) containing 500 μg/mL gentamicin. The plates were incubated at 35 ± 2°C for 24 h. The growth of more than one colony in the spotted zone was considered HLGR. The control quality of the culture plates was determined by reincubation at 35 ± 2°C for 24 h. VRE isolates were also detected by culturing on BHI agar supplemented with 6 μg/mL vancomycin (HiMedia, Mumbai, India), according to a previously described method [10, 12].
2.4. Antimicrobial Susceptibility Testing
Antibiotic susceptibility tests were performed using the standardized Kirby–Bauer disc diffusion technique on Mueller–Hinton agar (HiMedia, Mumbai, India). Commercially available disks of antimicrobial drugs (Mast Group, UK), which have been most frequently used for the treatment of enterococcal infections, were selected and tested as recommended by the Clinical and Laboratory Standards Institute [13] (“CLSI (2021) Performance Standards for Antimicrobial Susceptibility Testing; Twenty-Fifth Informational Supplement; Clinical and Laboratory Standards Institute, Wayne, M100-S25.,” n.d.). Accordingly, the susceptibility of the isolates to the following antibiotics was examined: penicillin G (10 units/disk), ampicillin (10 μg/disk), ampicillin-sulbactam (10 + 10 μg/disk), gentamicin (10 μg/disk), nitrofurantoin (300 μg/disk) (only for patients with a suspected UTI), and linezolid (30 μg/disk). Susceptibility to vancomycin was confirmed by determining the MIC using Epsilometer (E) test strips (Liofilchem®, Italy). E. faecalis ATCC 29212 was used as a quality control reference strain.
2.5. Statistical Analysis
Data analysis was performed using Excel 2022 and IBM SPSS Statistics version 20.0 (Chicago, IL, USA).
3. Results
A total of 404 clinical isolates of Enterococcus spp. were obtained from children over five years. The patients' ages ranged from infancy (1 day) to 15 years. The median patient age was 3 ± 1 months. 47.5% of the patients were female, and 52.5% were male.
The proportions of enterococcal isolates from 2016 to 2021 were 71.3% (288 out of 404), 25.5% (103 out of 404), and 3.2% (13 out of 404) for Enterococcus faecium, Enterococcus faecalis, and Enterococcus spp., respectively.
The distribution of enterococci isolates based on the inpatient and outpatient clinics is outlined in Table 1. The data reveal that 17.3% (70 out of 404) of the isolates originated from outpatients, whereas the vast majority, constituting 82.7% (334 out of 404), were sourced from inpatients.
Seventy out of 404 isolates (17.3%) were collected from outpatients or those referred to emergency department and classified as community-acquired enterococci and the remainder (82.7%) from different wards as follows: urology (10.4%), pediatric intensive care unit (PICU) (7.4%), respiratory (10%), nephrology and dialysis (9.6%), neonatal intensive care unit (NICU) (4.8%), surgical (3.9%), neonatal (3.9%), gastroenterology (2.9%), infection (1.9%), neurology (1.4%), and oncology (1.4%), were considered as nosocomial enterococci.
A significant proportion of isolates was recovered from urine samples (55.9%, n = 226), followed by blood culture (29.7%, n = 120), wounds (3.5%, n = 14), nasal discharge (1.7%, n = 7), bronchoalveolar lavage (BAL) (1.2%, n = 5), ascitic fluid (1%, n = 4), abscess (0.7%, n = 3), CSF (0.7%, n = 3), dialysis fluid (0.5%, n = 2), peritoneal cavity (0.5%, n = 2), synovial fluid (0.5%, n = 2), central venous line (CVL) (0.2%, n = 1), urinary catheter (0.2%, n = 1), and other body fluid samples (3.5%, n = 14).
In our study, all isolates were assessed for resistance rates without species differentiation (Table 2), revealing high-level gentamicin resistance (HLGR) at 87.4% (90.9% in E. faecalis and 87.7% in E. faecium) and ciprofloxacin resistance at 98.2% (84.6% in E. faecalis and 99.3% in E. faecium). Ampicillin resistance rate was 60.9% (14.6% in E. faecalis and 78.8% in E. faecium), while vancomycin resistance was 49% (11.7% in E. faecalis and 63.5% in E. faecium) (Table 3). All the isolates were resistant to ampicillin-sulbactam. The resistance rates of ampicillin, penicillin, and vancomycin in inpatients were twice as high as those in outpatients (Table 4). 98% of the isolates were susceptible to linezolid and 2% were resistant (0% in E. faecalis and 2.2% in E. faecium). 92.5% of the isolates were susceptible and 5.3% were resistant to nitrofurantoin (0% in E. faecalis and 7.9% in E. faecium).
The antibiotic susceptibility results showed that linezolid was the most active antibiotic against the tested enterococcal isolates (98% susceptibility rate). Nitrofurantoin showed excellent activity against urinary enterococcal isolates (92.5% as the susceptibility rate). In addition, 49.3% (n = 199) of the isolates were identified to have the VRE phenotype (12.6% in E. faecalis and 63.5% in E. faecium). As well as VRE phenotype was seen in 56.9% of inpatients and 12.9% of outpatients. Figure 1 shows a panel of VRE and non-VRE Enterococcus strains.
Forty-two point one percent (42.1%) of the total enterococci isolates were MDR (11.7% in E. faecalis and 54.2% in E. faecium). MDR enterococci isolates were detected in 48.8% of inpatients and 10% of outpatients.
The HLGR phenotype was detected in 87.4% of E. faecalis, E. faecium, and other Enterococcus spp. isolates. The majority (90.9%) of HLGR was found in E. faecalis isolates. Figure 2 displays a panel of HLGR and non-HLGR Enterococcus strains.
Altogether, five of 404 (1.2%) enterococcal isolates had both VRE and HLGR phenotypes and were resistant to linezolid. In addition, resistance to linezolid and nitrofurantoin was only observed in E. faecium, and a greater number of E. faecium strains showed resistance to other antibiotics than E. faecalis strains.
4. Discussion
Since the late twentieth century, when enterococci have emerged as a significant cause of nosocomial infections, bacteria have become the second most common nosocomial pathogen and the third leading cause of nosocomial bloodstream infections [14]. Enterococcal infections can include serious life-threatening disorders, especially in children, such as meningitis, septicemia, and infective endocarditis [15]. However, few studies have been conducted on enterococci isolated from children in Iran. In our study, E. faecium and E. faecalis comprised 71.3 and 25.5% of the Enterococcus spp. isolated from pediatric patients, respectively. This observation is similar to reports from other regions of Iran and other countries, in which the distribution of enterococcal species derived from clinical samples, such as blood, urine, pleural fluid, cerebrospinal fluid, sputum, ascites, and hydrothorax, changed in favor of E. faecium [16–19]. In contrast, some studies have shown that the frequency of E. faecalis isolates in clinical specimens is usually two to three times higher than that of E. faecium isolates [20, 21]. This difference may be due to the different origins of the collected samples and different geographical regions. Furthermore, the increase in the prevalence of E. faecium species may be due to the common resistance of enterococci to antienterococcal drugs such as ampicillin, aminoglycosides, and glycopeptides [22, 23]. In our study, the highest vancomycin resistance was found in E. faecium isolates. The occurrence of VRE diverges in different countries, with a high frequency described in VRE in the US, the UK, Saudi Arabia, Ireland, and Turkey, whereas a low percentage is specific to some European countries such as Italy and France [24, 25].
Invasive enterococcal infections pose a significant challenge due to the emergence of drug-resistant strains. The standard treatment of vancomycin, ampicillin, and aminoglycoside antibiotics is becoming less effective as resistance to these antibiotics grows [26]. Vancomycin-resistant Enterococcus (VRE) and high-level gentamicin-resistant (HLGR) strains are particularly concerning, as they are responsible for a rising number of nosocomial infections in both adults and children [27]. Identifying alternative treatment options for these drug-resistant enterococci is crucial for the effective management and treatment of such infections [28]. Little data are available on the epidemiology and impact of VRE and HLGR infections in Iranian children. In this survey, we investigated the epidemiology and prevalence of clinical isolates of enterococci among the pediatric patients during the five years. Approximately one-third of the enterococcal strains were isolated from urology and PICU wards. Previously, a similar distribution was reported among hospitalized children in the urology ward located at the Children's Medical Center by Pourakbari et al.[29] and Sabouni et al. [30]. The high frequency of enterococcal strains isolated from the urology ward demands more attention to infection prevention and control (IPC) programs than in other units [31].
Enterococci are typically antibiotic-resistant. Owing to the intrinsic and acquired resistance to most antibiotics, the addition of vancomycin resistance meant that many enterococcal infections have become untreatable [32]. The high isolation rate (49.3%) of clinical VRE in our study raised significant concerns. It was found that the majority of VRE isolates were obtained from inpatients, with a lower percentage originating from outpatients. However, the prevalence of VRE in a specific population can vary significantly due to factors such as geographical location, duration of hospital exposure, usage of medical devices, sample size, and others [33].
To date, this is the largest high-risk pediatric population screened for VRE infections. A lower distribution of VRE (16%) was observed in another study conducted in children at the Children's Medical Center [29]. In this study, E. faecium was the predominant VRE isolate (45.30%), which is consistent with the results of similar studies [34, 35]. In contrast, E. faecalis is the predominant VRE, which has been reported in other studies [36]. Based on these findings, a substantial increase in the hospitalization rate for VRE infection among pediatric patients has been observed over the last few years, paralleling the increase observed in the hospitalized adult population [37]. The reason for this increase in VRE incidence may be the amalgamation of the same factors, including selective pressure from broad-spectrum antimicrobial agents, an increasing number of critically ill and immunosuppressed at-risk patients, and increased nosocomial transmission owing to deficiencies in hospital infection control practices [38]. In addition, it has been reported that long-term use of vancomycin and cephalosporins can potentially lead to the selection of intestinal carriage of vancomycin-resistant enterococci (VRE) [39]. It is important to remember that VRE infections are associated with high morbidity and mortality rates as well as increased duration and cost of hospitalization [40]. Owing to the excellent performance of hospital infection control and accuracy in prescribing antibiotics in developed countries, a very low prevalence of VRE has been reported in countries such as Japan and the United States [37, 41]. The majority of isolates showed more than 80 percent resistance to high levels of gentamicin in vitro. In numerous studies conducted both in Iran and other countries, a high prevalence of HLGR has been reported in E. faecalis [42, 43]. This may be attributed to its higher prevalence in clinical settings. However, our report deviates from this trend, as we observed a higher frequency of HLGR in E. faecium, aligning with the findings of Hayakawa et al. [36]. This divergence highlights the need for further research to understand the varying patterns of HLGR in different Enterococcus species. As well as, it is necessary to consider the origin of the clinic (inpatient or outpatient) when assessing resistance rates. Our study revealed that HLGR was significantly more common among inpatients compared to outpatients. This disparity in resistance rates among E. faecium isolates could potentially be attributed to this difference in clinical settings [19].
Overall, the isolation rate of HLGR was greater than that of VRE in our study, which is similar to the findings of other studies [44]. The treatment of HLGR enterococci poses a significant challenge in healthcare settings. Recent reports have suggested the use of an antipeptidoglycan active agent in combination with a membrane-active agent to address this problem [45]. Despite the predominance of HLGR enterococci in our region, vancomycin continues to demonstrate antimicrobial efficacy against such strains. However, the emergence of VRE isolates is a cause for concern and warrants continuous surveillance using both genetic and phenotypic methods to address this type of resistance. This “red alarm” highlights the importance of proactive measures in our health system to effectively manage and mitigate the impact of HLGR enterococci [46].
In our surveillance, a high prevalence of multidrug-resistant (MDR) enterococcal isolates, defined as resistance to three or more antibiotic classes, was observed among pediatric patients. The prevalence of MDR enterococci was more common in E. faecium (54.2%) compared to E. faecalis (11.7%), which is in concordance with previous studies [33, 47]. In addition, the MDR phenotypes were significantly higher for both E. faecium and E. faecium of inpatient isolates compared to those from outpatients.
It has been shown that the majority of VRE isolates had additional resistance to penicillin G, ampicillin, ampicillin-sulbactam, and gentamicin. However, the resistance to these antibiotics was significantly lower than that in the non-VRE isolates. Generally, E. faecium is less susceptible to β-lactam agents than E. faecalis because their penicillin-binding proteins (PBPs) have lower affinities for these antibiotics [48]. In addition, resistance mechanisms to other antibacterial agents, except β-lactams, could be encoded by conjugative transposons, and the presence of MDR isolates may facilitate the increase, transmission, and spread of drug resistance in hospital wards [49]. Previously, clinical isolates of MDR enterococci have been frequently reported in several studies. In developing countries, unreasonable administration of antimicrobial agents, especially beta-lactam antibiotics, may be responsible for developing MDR enterococci [47].
Linezolid is used as the first-line treatment for infections caused by VRE. The potential coexistence of linezolid and vancomycin resistance among enterococcal strains also raises concerns, considering the importance of these drugs in the treatment of MDR enterococcal isolates [50].
In the present study, the rate of linezolid resistance was 2%, whereas various studies have reported 100% sensitivity to linezolid [51]. An intriguing aspect of this study was the identification of four VRE strains from pediatric patients who were not susceptible to linezolid. Our results were similar to those of a recent study that found four clinical isolates of E. faecium that were resistant to both linezolid and vancomycin [52].
Limited treatment options are available for linezolid resistance VRE (LRVRE) with difficult-to-treat infections. Current treatment options such as linezolid, daptomycin, quinupristin/dalfopristin, and tigecycline have shown promising efficacy against VRE infections [53]. Moreover, combination therapy may offer a distinct advantage over monotherapies due to their broad spectrum and synergistic effect [54]. The use of quinupristin/dalfopristin (Q/D) in combination with rifampin or doxycycline and daptomycin and/or linezolid in combination with ampicillin, tigecycline, doxycycline, rifampin, and fluoroquinolones has been reported in some literature for the treatment of VRE infections [55].
Although molecular typing was not performed in this study to determine the potential clonality of the linezolid-nonsusceptible VRE strain from the same region, this was a possibility, as the nosocomial spread of linezolid- and vancomycin-resistant enterococci has been previously described [56].
While linezolid nonsusceptibility remains sporadic among enterococci, constant surveillance of linezolid activity is required to control these opportunistic pathogens.
5. Conclusion
To our knowledge, this study is among the few to show the prevalence of VRE and linezolid nonsusceptible enterococcal isolates in pediatric patients. Therefore, efficient and accurate epidemiological typing methods such as pulsed-field gel electrophoresis (PFGE) have been suggested for surveillance and to limit the occurrence and spread of epidemic clones within and between hospitals and community settings. Our study showed a rise in resistance to gentamicin and vancomycin, highlighting the need for a reassessment of antibiotic treatments in Iran. Moreover, to prevent the spread of VRE and linezolid nonsusceptible strains in healthcare settings, resistance measures derived from those used in many hospitals were implemented. Consequently, antimicrobial susceptibility testing is essential for managing enterococcal infections, and antibiotics should be prescribed carefully. Continuous monitoring of HLGR and VRE prevalence and drug susceptibilities for both inpatient and community isolates is highly recommended.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Krawczyk B. Wityk P. Gałęcka M. Michalik M. The many faces of Enterococcus spp.—commensal, probiotic and opportunistic pathogen Microorganisms 2021991525623457679610.3390/microorganisms 9091900 PMC 8470767 · doi ↗ · pubmed ↗
- 2Ramos S. Silva V. Igrejas G. Poeta P. Enterococci, from harmless bacteria to a pathogen Microorganisms 20208811210.3390/microorganisms 8081118 PMC 746379232722391 · doi ↗ · pubmed ↗
- 3Guzman Prieto A. M. van Schaik W. Rogers M. R. C. Global emergence and dissemination of enterococci as nosocomial pathogens: attack of the clones? Frontiers in Microbiology 20167 MA Yp. 78810.3389/fmicb.2016.007882-s 2.0-84973443007 PMC 488055927303380 · doi ↗ · pubmed ↗
- 4Gold H. S. Vancomycin-resistant enterococci: mechanisms and clinical observations Clinical Infectious Diseases 20013322101910.1086/3218152-s 2.0-003587951211418881 · doi ↗ · pubmed ↗
- 5Shepard B. D. Gilmore M. S. Antibiotic-resistant enterococci: the mechanisms and dynamics of drug introduction and resistance Microbes and Infection 2002422152410.1016/s 1286-4579(01)01530-12-s 2.0-003618905611880055 · doi ↗ · pubmed ↗
- 6Bhatt P. Patel A. Sahni A. Emergence of multidrug resistant enterococci at a tertiary care centre Medical Journal Armed Forces India 20157121394410.1016/j.mjafi.2014.08.0072-s 2.0-8493072894225859076 PMC 4388963 · doi ↗ · pubmed ↗
- 7Haghi F. Lohrasbi V. Zeighami H. High incidence of virulence determinants, aminoglycoside and vancomycin resistance in enterococci isolated from hospitalized patients in northwest Iran BMC Infectious Diseases 2019191 p. 74410.1186/s 12879-019-4395-32-s 2.0-85071637500 PMC 671282231455296 · doi ↗ · pubmed ↗
- 8Moghimbeigi A. Moghimbeygi M. Dousti M. Prevalence of vancomycin resistance among isolates of enterococci in iran: a systematic review and meta-analysis Adolescent Health, Medicine and Therapeutics 201891778810.2147/ahmt.s 18048930532606 PMC 6241717 · doi ↗ · pubmed ↗