Establishment and characterization of a rat model of scalp-cranial composite defect for multilayered tissue engineering
Yi Zhu, Ou Mei, Hui Zhang, Wulin You, Jiamin Zhong, Caralyn P. Collins, Guowei Shen, Changqi Luo, Xingye Wu, Jingjing Li, Yi Shu, Ya Wen, Hue H. Luu, Lewis L. Shi, Jiaming Fan, Tong-Chuan He, Guillermo A. Ameer, Cheng Sun, Liangyuan Wen, Russell R. Reid

TL;DR
This paper introduces a rat model for studying scalp-cranial composite defects, enabling long-term research on tissue engineering and healing.
Contribution
A novel rat model with a 3D-printed wound obturator to maintain chronic composite defects for tissue engineering studies.
Findings
The wound obturator prevents scalp healing for over 6 weeks while preserving the cranial defect.
The model shows minimal biotoxicity and avoids endocranium-granulation adhesion.
An autologous reconstruction model was developed as a positive control with reproducible healing.
Abstract
Composite cranial defects have individual functional and aesthetic ramifications, as well as societal burden, while posing significant challenges for reconstructive surgeons. Single-stage composite reconstruction of these deformities entail complex surgeries that bear many short- and long-term risks and complications. Current research on composite scalp-cranial defects is sparse and one-dimensional, often focusing solely on bone or skin. Thus, there is an unmet need for a simple, clinically relevant composite defect model in rodents, where there is a challenge in averting healing of the skin component via secondary intention. By utilizing a customizable (3D-printed) wound obturator, the scalp wound can be rendered non-healing for a long period (more than 6 weeks), with the cranial defect patent. The wound obturator shows minimal biotoxicity and will not cause severe…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
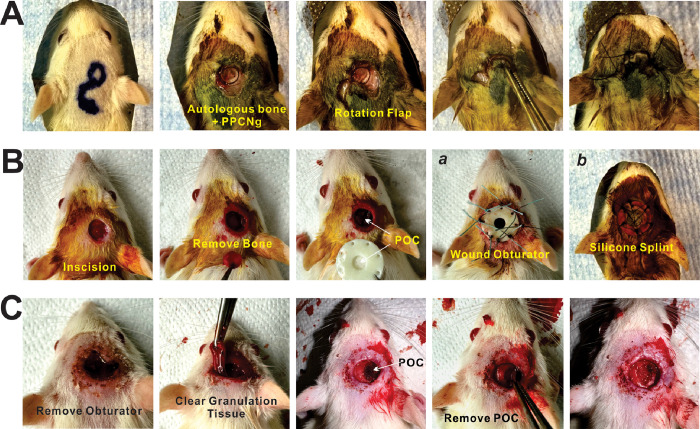 Figure 1
Figure 1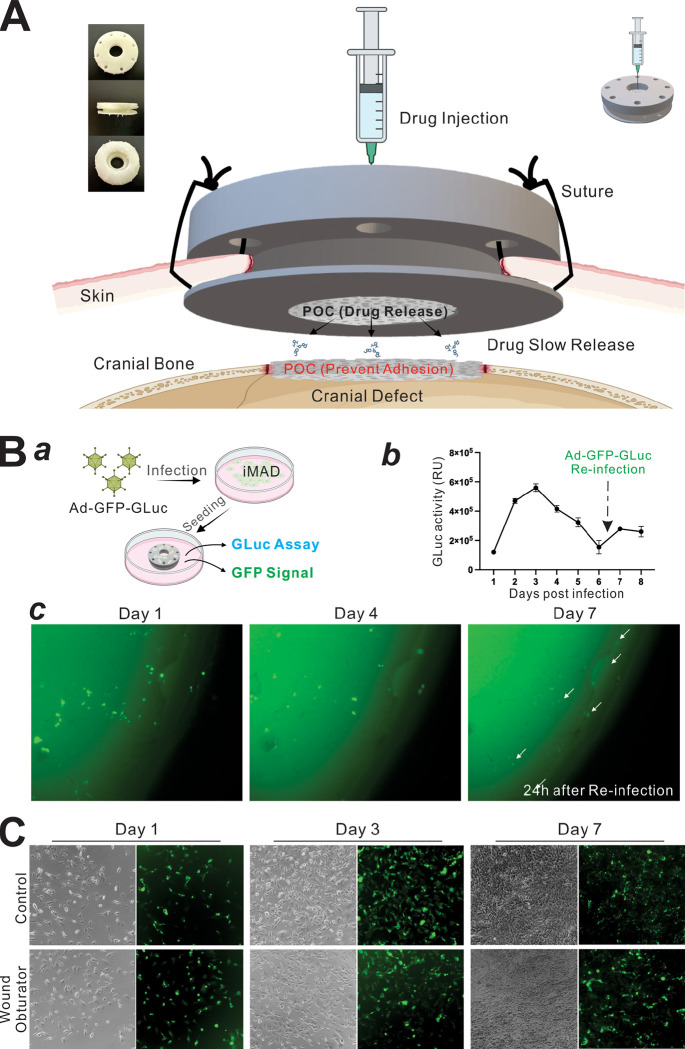 Figure 2
Figure 2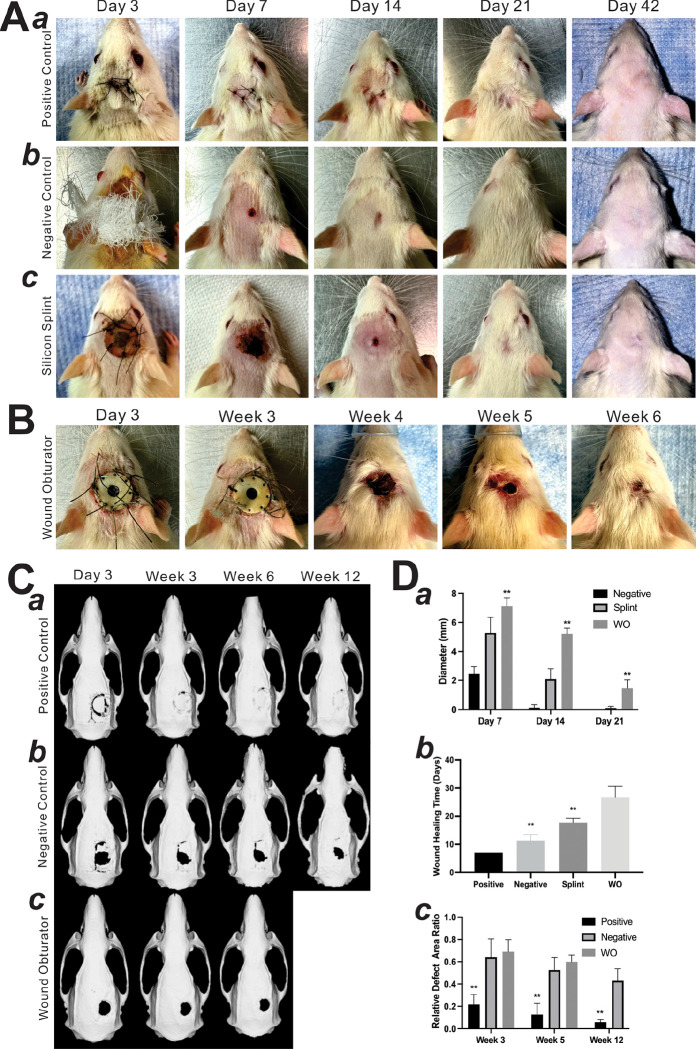 Figure 3
Figure 3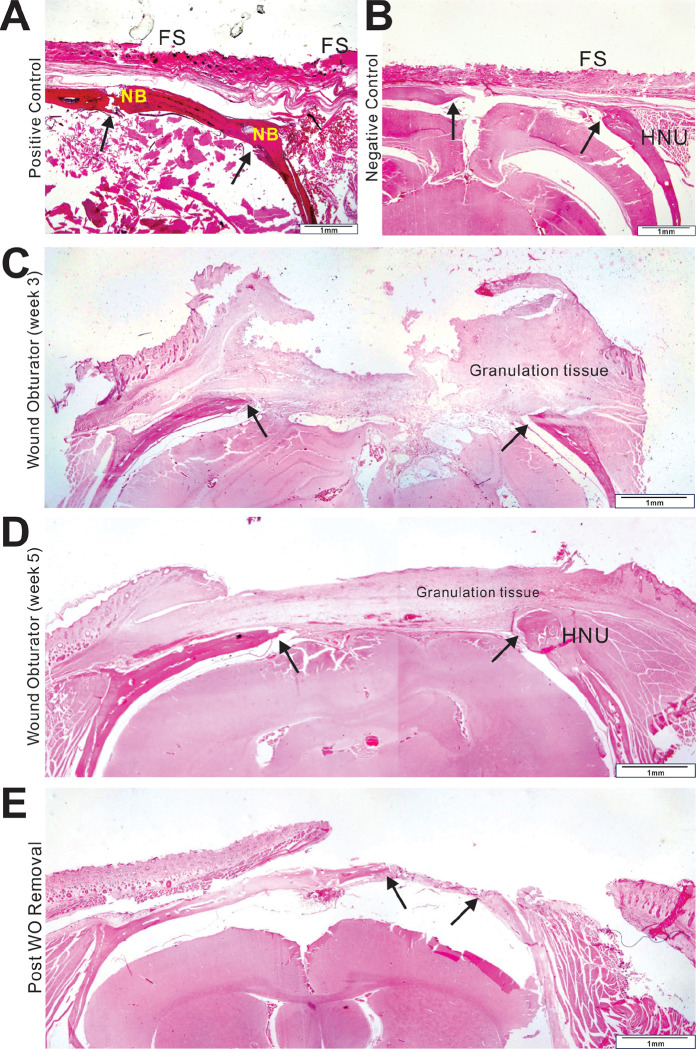 Figure 4
Figure 4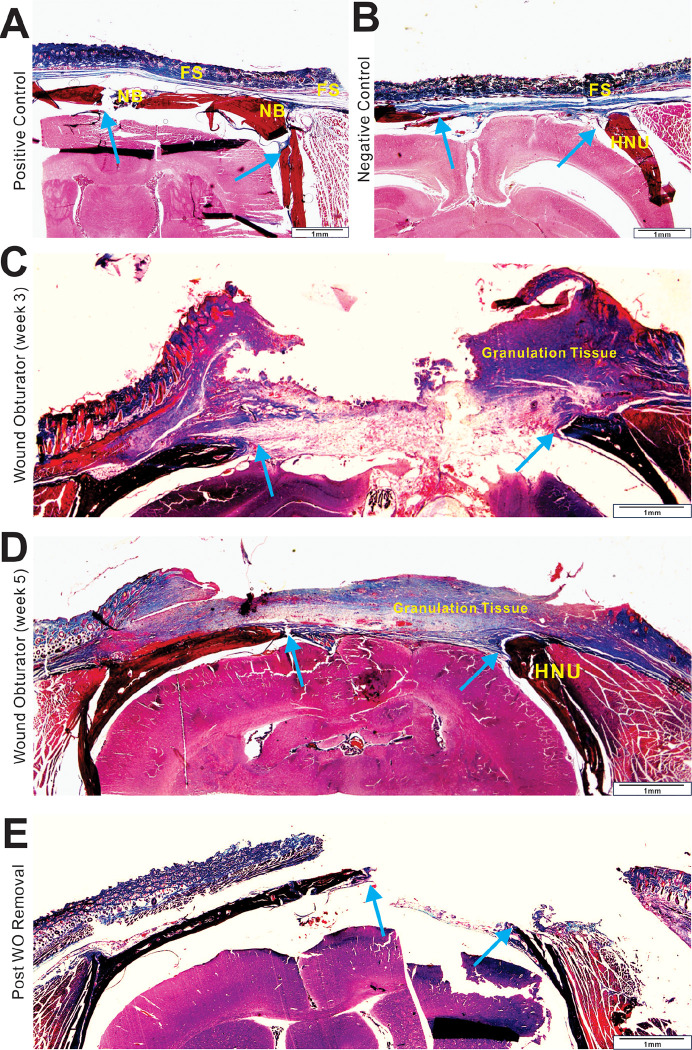 Figure 5
Figure 5Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsBone Tissue Engineering Materials · Tissue Engineering and Regenerative Medicine · Electrospun Nanofibers in Biomedical Applications
INTRODUCTION
Composite cranial defects, which affect multiple tissue types, pose significant challenges for reconstructive surgeons ^1^. Etiologies of composite cranial defects are diverse, including penetrating trauma, burns, tumor resections, radiation exposure, or infections ^2^. Often, many of these cases cannot undergo one-stage repair due to factors such as concurrent infections, polytrauma, ongoing radiation therapy, or prior cranioplasty failures, thereby leading to chronic defects ^3^. Furthermore, single-stage reconstructive measures, such as composite or chimeric free-flaps, involve extensive undertakings fraught with potential risks and complications (references). Notably, the transition from acute to chronic repair significantly impacts healing dynamics, most prominently observed as a deceleration in healing speed ^4^ and a reduced success rate of autologous bone and soft tissue reconstruction^5,6^.
In recent decades, biomaterial-based cranial or scalp repair through tissue engineering has emerged as a focal point in research ^7^. Rodents, valued for their small size and ease of maintenance, serve as effective animal models extensively used in studies of cranial defects and skin regeneration ^8–11^. However, composite defect models, particularly those that mirror chronic clinical conditions, are rarely reported. The primary challenge is the rapid rate of skin healing in rodents, which can culminate within two weeks ^12^. This rapid healing hinders the investigation of chronic defect regeneration.
Existing models for chronic skin defects in rodents include: 1) Pressure ischemia-reperfusion, which involves multiple cycles of ischemia and reperfusion using a steel plate and magnet ^13^. This method is cumbersome and the metal components interfere with micro-CT scans for studies involving cranial defects; 2) Diabetic rodents, which require a prolonged period to develop the diabetic condition and do not accurately replicate clinical scenarios ^14^; and 3) Infection-based models, which are difficult to control and may adversely affect regenerative outcomes ^15^. None of these models are ideally suited for studying composite cranial defects in rodents.
In this study, we developed a clinically relevant, chronic composite cranial defect model in rats. Specifically, we successfully established a rat model of a scalp-cranial composite defect along with a unique complementary positive control, providing a stable platform for subsequent tissue repair and bone regeneration studies. The experimental model effectively slowed the scalp healing process and preserved the cranial defect, embodying the characteristics of a “chronic composite defect”. The positive control exhibited reliable and reproducible healing through autologous reconstruction, mirroring current surgical practice. Collectively, our reported model provides a stable platform for subsequent research not only for composite tissue engineering and scaffold design but also for mechanistic studies of composite tissue healing.
MATERIALS AND METHODS
Cell Culture and Chemicals
Human HEK-293 cells were obtained from the American Type Culture Collection (ATCC, Manassas, VA). 293pTP, RAPA and 293GP cells were derived from HEK-293 cells as previously described ^16–18^. The mouse mesenchymal cell line iMAD was previously described ^19,20^. All cells were cultured in DMEM supplemented with 10% fetal bovine serum (FBS, Gemini Bio-Products), 100 U/ml penicillin, and 100μg/ml streptomycin at 37°C in 5% CO_2_ as described ^21–26^. Unless indicated otherwise, chemicals were obtained from Thermo Fisher Scientific (Waltham, MA) or Millipore Sigma (St. Louis, MO).
Construction and Amplification of the Recombinant Adenoviral Vector Ad-GFP-GLuc Expressing Both GFP and Gaussia Luciferase (GLuc)
Recombinant adenovirus Ad-GFP-GLuc was constructed by using either the AdEasy technology or the Gibson DNA Assembly-based OSCA system as previously described ^27–30^. Briefly, the coding region of Gaussia luciferase (GLuc) ^31–33^ was PCR amplified and subcloned into the adenoviral shuttle vector pAdTrack-CMV, followed by homologous recombination reactions with the adenoviral backbone vector pAdEasy1 in BJ5183 cells ^28,34^. The resultant recombinant adenoviral plasmid was used to generate adenovirus Ad-GFP-GLuc. Alternatively, the Ad-GFP-GLuc was constructed by using the Gibson DNA Assembly-based OSCA system as previously described ^30^. The recombinant adenovirus Ad-GFP-GLuc was packaged in 293pTP cells, and amplified to high titers in HEK-293, RAPA, 293pTP, or 293GP cells ^16–18^. The Ad-GFP-GLuc also co-expresses GFP marker gene. Polybrene (final concentration at 6μg/mL) was added to enhance adenoviral transduction efficiency in the iMAD cells as previously described ^35,36^.
Surgical Procedures of Initial Operation
The protocols of this study were approved by the Institutional Animal Care and Use Committee (IACUC) of The University of Chicago (ACUP #71445). All experiments were performed in accordance with relevant guidelines and regulations. Bone and soft tissue defects in rat models (8-week-old Sprague Dawley rats, weight range 200–350g; Envigo, Indianapolis, IN) were carried out following the approved guidelines.
Images of the surgical procedures are shown in Fig. 1. Briefly, anesthesia was induced in rats through isoflurane inhalation, complemented by intraperitoneal injection of ketamine (50–75 mg/kg) and xylazine (7–10 mg/kg). After prone positioning, the rat was prepared by scalp depilation, sterilization with iodine tincture, and application of a sterile drape. Using a biopsy punch, a 6 mm circular incision was made above the parietal cranium, and the pericranium was removed with a neuro spatula. A cranial defect was then carefully drilled in the parietal bone with a 6 mm trephine under continuous normal saline irrigation to prevent tissue thermal injury (Dremel^®^ USA, Robert Bosch Tool Corp). The bone disc was removed, and hemostasis was meticulously achieved.
In the positive control (autologous reconstruction) group (n = 6, three for histological staining at 5 weeks, three for long-term micro-CT scan), the excised bone was replaced as an autograft with 100μl of a biocompatible, thermosensitive polymer, polyethylene glycol citrate-co-N-isopropylacrylamide pre-mixed with gelatin (PPCNg) ^37,38^, and the overlying wound was reconstructed using a rotation flap (Fig. 1A). Conversely, the negative control group (n = 3, one for histological staining at 5 weeks, two for long-term micro-CT scan) was left with the bone and scalp defects untreated; the wound was merely wrapped in gauze to inhibit infection. For the experimental group, the incision was supplemented using either a standard silicone splint (Grace Bio-Labs; n = 4) or a wound obturator (n = 6, two for histological staining at 3 weeks, 4 for secondary operation) to counteract the rapid initial self-healing of the scalp post-trauma ^39^ (Fig. 1B). To prevent adhesion between the dura mater and granulation tissue, a citrate-based polymer poly (octamethylene citrate) (POC) disc ^40^ was implanted into the cranial defect. In the experimental group, 100 μL of an anti-inflammatory mixture (1 μM vincristine, 0.5 mg/mL kanamycin) were injected through the central opening of the wound obturator (WO), designed for absorption and gradual release by the POC within the obturator. Vincristine’s application was aimed at inhibiting the granulation tissue generation process. All groups received standard postoperative pain relief and monitoring per IACUC guidelines.
Surgical Procedures of Secondary Operation for Further Tissue Regeneration Study
Three weeks post-initial surgery, the experimental group (WO group) underwent a secondary operation (Fig. 1C). Following anesthesia and sterilization, all sutures were carefully removed along with the wound obturator. Mimicking clinical conditions, granulation and connective tissues were meticulously excised to refresh the margins of bone and scalp. This was achieved using hemostatic forceps, scissors, and scalpels in a layer-by-layer approach. Subsequently, the POC disc, which prevented adhesion between the dura mater and granulation tissue, was gently lifted and the margins of the cranial defect were cleared. By this secondary method, the surgically debrided defects are primed for skin-bone tissue engineering via regenerative scaffold placement.
Wound Obturator (WO) Design and 3-D Printing
The wound obturator utilized in the experimental group is depicted in Fig. 2A. This device, crafted from resin xFLEX475-white (NEXA 3D) through 3-D printing, comprises two rings that securely anchor the scalp, while an inner cylindrical wall offers mechanical resistance against centripetal scalp growth. A POC disc was placed within the central cavity. The upper ring features a central hole that facilitates both exudate drainage and serves as an access point for injecting therapeutics. Peripheral holes are designed for suturing. Both the POC and the obturator were sterilized via a two-hour immersion in PBS containing penicillin and streptomycin, followed by comprehensive UV post-curing.
Cell-Wound Obturator Co-Culture Cell Viability Assay
Exponentially growing iMAD cells were seeded at a low density (5 × 10^4^ cells/well) in 12-well plates and co-cultured with either the wound obturator (WO) or no WO control. Viable cells were visualized by using Calcein-AM staining and imaged at indicated time points as previously described ^41,42^.
Cell Biocompatibility Assay
Subconfluent iMAD cells were infected with Ad-GFP-GLuc for 16h. Cells were harvested, resuspended in DMEM, and seeded to the pre-treated obturators submerged in culture medium (approx. 1 × 10^4^ cells per seeding) (Fig. 2B–a). At 6 days post seeding, the cell-laden obturator was reinfected with Ad-GFP-GLuc. Both GFP fluorescence and the secreted Gaussia luciferase activity were monitored at the indicated timepoints as indicators of cell viability. Gaussia luciferase activity was quantified using the Secrete-Pair^™^ Gaussia Luciferase Assay Kit (GeneCopoeia, Rockville, MD) as previously described ^24,31,43^.
Micro-CT Imaging Analysis
Live rats were subjected to micro-CT scans at weeks 0 (three days post-operation), 3, 5, and 12, except for the WO group, which was scanned at weeks 0, 3, and 5, using the X-CUBE Preclinical CT Imager (Molecubes NV, Belgium) at The University of Chicago Integrated Small Animal Imaging Research Resource (iSAIRR) facilities. Spiral high-resolution CT acquisitions were performed with an x-ray source of 50 kVp and 200 μA. Volumetric CT images were reconstructed in a 350 × 350 × 840 format with voxel dimensions of 200 μm^3^. A few volumetric CT images were also reconstructed in a 700 × 700 × 374 format with voxel dimensions of 100 μm^3^ to evaluate the performance of bone healing. Reconstructions were performed using 3-D Slicer software (Version 5.4.0) as previously described ^44–50^. Defect areas were quantified using Image J (Version 1.53k). Relative Cranial Defect Area Ratio (RCDAR) was calculated to quantify the healing rate. RCDAR= (Area at each timepoint/Area at week 0) *100%.
Histological Evaluation
The retrieved cranial specimens were fixed in 10% PBS-buffered formalin for 2 days and decalcified in 5% nitric acid, followed by dehydration, paraffin embedding, and sectioning. Sections were deparaffinized and subjected to H & E staining (Volu-Sol) and Masson trichrome staining (Newcomer Supply) as previously described ^51–56^.
Statistical Analysis
All experiments were performed at least three times or repeated in three batches of independent experiments. Data were analyzed using GraphPad Prism 7 and presented as the mean ± standard deviations (SD). Statistical significance was determined by one-way ANOVA and the student’s t-test for the comparisons between groups. A value of p < 0.05 was considered statistically significant. The work has been reported in line with the ARRIVE criteria ^57^.
RESULTS
Rapid skin healing prevents the creation of a rat model of clinically relevant scalp-cranial composite defect
For the establishment of a reliable murine composite scalp-cranial defect model, we had to devise both clinically relevant positive and negative controls. (Fig. 1). In the positive control (autologous reconstruction) group, the excised bone was replaced as an autograft with 100μl of the biocompatible, thermosensitive polymer PPCNg^37^, and the overlying wound was reconstructed using a rotation flap (Fig. 1A). Conversely, the negative control group was left with the bone and scalp defects untreated; the wound was merely covered in gauze to prevent desiccation (Fig. 1B–ab).
For the experimental group, a citrate-based polymer poly (octamethylene citrate) (POC) disc ^40^ was first implanted into the cranial defect to prevent adhesion between the dura mater and granulation tissue (Fig. 1B–c). Our preliminary experiments indicated that the 6-mm circular scalp wound in rats healed effectively in 7–10 days. Thus, to produce a non-healing composite wound, we further supplemented the defect with either a homemade wound obturator (WO) (Fig. 1B–d) or a silicone splint (Fig. 1B–e). While the silicone splint is commercially available and somewhat widely used, our results demonstrated that our homemade 3D printed wound obturator provided more rigid fixation and thus more effective prevention of scalp healing.
To mimic clinical conditions, the experimental group (WO group) underwent a second “priming” operation to prepare the composite defect for composite reconstruction via tissue engineering strategies (Fig. 1C). This priming procedure involved removal of the wound obturator, followed by meticulous sharp debridement of granulation tissue to refresh the margins of the bone and scalp. Subsequently, the POC disc, which prevented adhesion between the dura mater and granulation tissue, was gently lifted and the margins of the cranial defect were cleared (Fig. 1C).
The 3-D printed Wound Obturator (WO) shows minimal biotoxicity and does not cause severe endocranium-granulation adhesion
As shown in Fig. 2A, the wound obturator device was crafted from resin xFLEX475-white (NEXA 3D) through 3-D printing, comprising two rings that securely anchor the scalp, while a inner cylindrical wall offers mechanical resistance against centripetal scalp growth. Within the central cavity, a POC disc was placed to serve the following functions: a) physically occupying space to stent the wound and prevent wound closure via contraction (“secondary intention”), and to minimize granulation tissue formation inside the central cavity; b) acting biochemically as a repository to absorb and gradually release medications, including antibiotics and agents that slow cell proliferation; and c) absorbing inflammatory exudates to protect against potential infections. The upper ring features a central hole that facilitates both exudate drainage and serves as an access point for injecting therapeutics. Peripheral holes are designed for suturing.
It is noteworthy that, to inhibit the granulation tissue generation process and prevent local infection, a mix of vincristine (1 μM) and kanamycin (0.5 mg/mL) was injected through the central opening for absorption and gradual release by the POC within the obturator (Fig. 2A). The POC was easily removable without any adhesion. Upon its removal, no invasion of fibrous tissue into the extradural space was observed, and the margins of the bone defect remained clear and clean, ideal for subsequent regenerative experimentation. In the 5-week histological section of the wound obturator group, the defect area remained protected by a distinct fibrous layer even after POC removal, preventing adhesion with granulation tissue after the secondary operation.
The biocompatibility assay demonstrated that Ad-GFP-Gluc infected iMAD cells could survive on the obturator for more than seven days (Fig. 2B–a). Upon reinfection with Ad-GFP-Gluc, Gaussia luciferase activity was partially restored (Fig. 2B–b) and emergent GFP signals were observed overnight (Fig. 2B–c). Furthermore, results from the cell-obturator co-culture assays revealed no significant differences in cell proliferation rates at days 3 and 7 (Fig. 2C), suggesting that the material used for 3-D printing of the wound obturator may exhibit little or no significant cytotoxicity.
Autologous reconstruction achieves variable cranial bone healing in 3 weeks
As shown in Fig. 3A–a and Fig. 3C–a, the wound in the positive control group achieved complete healing within one week post operation. By the end of week 3, the positive control group exhibited retained bone graft take with varying amounts of osseointegration/fibrous union (RCDAR = 0.22 ± 0.09 at week 3), with a decelerated healing speed over the following weeks (RCDAR = 0.13 ± 0.10 at week 5, 0.06 ± 0.02 at week 12) (Fig. 3D).
Histological evaluation indicated that in the positive group, bone healing was promoted by bone callus modeling, interspersed with fibrous connective tissue and nourishing blood vessels (Fig. 4A and Fig. 5A), characteristic of “secondary bone healing” ^57^. Regarding skin healing, the closure with a rotation flap resulted in complete coverage of the skin defect. No hypertrophic granulation tissue was observed.
Critical-sized cranial defects exhibit limited bone self-healing capacity
In terms of animals in the negative control group, one in the silicone splint group was sacrificed because of uncontrollable infection, others survived until the endpoint. Micro-CT scans and subsequent 3D reconstructions revealed distinct cranial bone healing patterns among the groups (Fig. 3A–b and Fig. 3C–b). In contrast to the positive control group, the negative control group demonstrated markedly slower healing, showing an RCDAR of 0.64 ± 0.17, 0.53 ± 0.11, and 0.43 ± 0.11 at week 3, week 5, and week 12, respectively. Similarly, the WO group paralleled the negative control, with an RCDAR of 0.68 ± 0.02 at week 3 and 0.58 ± 0.06 at week 5 (Fig. 3D). These findings underscore the limited self-healing capacity of 6 mm cranial defects in rats without treatment over 12 weeks.
Histological analysis shows that the bony margins of the osseous defects in the negative group expanded into a round shape reminiscent of “hypertrophic nonunion” in clinical scenarios (Fig. 4B and Fig. 5B), thereby delaying or inhibiting the self-healing process ^58^. In the experimental group (WO group), the hypertrophic bone margin was not fully evident at 3 weeks post-trauma but became pronounced and consistent with that of the negative group by 12 weeks, suggesting that the first 3 to 4 weeks post-trauma may be critical for rapid bone healing.
WO effectively delays skin self-healing capacity up to 5 weeks post surgery
Wound healing conditions are shown in Fig. 3B and Fig. 3C. In the negative control (non-splinted) group, the wound achieved complete healing by 11.33 ± 2.08 days (Fig. 3D–b). In the experimental group, a silicone splint was employed to keep the wound open but dislodged after around 6 days, resulting in healing within 17.67 ± 1.53 days post-operation (Fig. 3A–c and Fig. 3D–b). Compared to the negative group, wound healing of the silicone group was only delayed by about 6 days (Fig. 3A–c and Fig. 3D–a). In contrast, the wound obturator can be maintained for over 5 weeks. Additionally, after the removal of the obturator, wound healing duration was extended to 26.67 ± 4.04 days (Fig. 3D–b), which is approximately 15 days longer than the non-splinted control group, fitting the criteria of a non-healing, chronic wound.
Histological survey revealed that in the negative control group, the fibrous scar tissue significantly contracted into a smaller structure (Fig. 4B and Fig. 5B). For the wound obturator group at 3 weeks, the obturator had been freshly removed, thus presenting a chaotic histological phenotype, characterized by irregular fibrous scars and granulation tissue (Fig. 4C and Fig. 5C). By 5 weeks, however, the tissue appeared more organized and anatomically defined. The scalp defect was covered by granulation and fibrous tissue, with skin progressively enveloping this tissue, culminating in healing marked by a smaller wound (Fig. 4D and Fig. 5D).
DISCUSSION
In the clinical arena, composite scalp-cranial defects arising from penetrating trauma, burns, tumor resections, radiation, or infections significantly compromise patient function and aesthetics, while producing a huge societal burden ^59^. The heterogeneity of these conditions demands considerable resources and versatility from reconstructive surgical teams to manage such complex injuries ^5^. Currently, the gold standard for reconstruction involves the use of autologous materials such as nonvascularized bone grafts, free soft tissue transfers, or combinations of vascularized bone and soft tissue (free composite or chimeric flaps) ^60^.
However, many of these cases cannot undergo one-stage repair due to factors such as concurrent infections, polytrauma, ongoing radiation therapy, or prior cranioplasty failures, thereby leading to “chronic defects” ^3,60^. Furthermore, the concept of replacing “like-with-like” in these defects may demand a large donor-site burden. Biomaterial-based reconstruction with cellular-based tissue engineering strategies represents a viable alternative in such circumstances, but it requires extensive validation before clinical adoption ^61^. Despite the clinical impact, research on composite scalp-cranial defects is sparse, often focusing solely on bone or skin. Thus, there is a clear need for a simple, clinically relevant composite defect model to serve as a testbed for regenerative approaches.
We established an autologous reconstruction model as the positive control, closely aligned with clinical practice. After replanting the cranial bone and utilizing a rotational flap for wound closure, rapid multilayer healing was observed within 3 weeks postoperatively. PPCNg ^37^, a thermoresponsive biomaterial that transitions reversibly from liquid to solid at 37°C, was applied to provide semi-rigid fixation of the bone graft and potentially accelerate the healing process. The PPCNg has been shown to promote wound closure without inducing a significant inflammatory response ^62^. However, it is important to note that although composite wound healing is achieved under these conditions, variations in autologous bone graft “take” and osseointegration in our model, which mimics clinical conditions, demand regenerative strategies to improve composite tissue healing. Additionally, in the clinical realm, often autologous options are not available or feasible due to patient factors. Nevertheless, the creation of a rodent positive control that mimics the “gold standard” is a novel feature of our project and establishes a benchmark to which to compare all other therapeutic approaches.
The composite scalp-cranial defect model is a key focus of our study. The primary challenge is maintaining the scalp wound in an unhealed state for a longer duration. Previously, several approaches have been developed to establish chronic skin conditions in rodents. Chen et al. ^62^ created ischemic wounds within a bi-pedicled dorsal flap using six uniformly placed incisions, demonstrating that wounds in non-necrotic ischemic zones heal more slowly than those on normally perfused skin; however, these effects were transient, delaying only 4 days more than control group, and the technique is unsuitable for used on head. Peirce et al. ^13^ surgically implanted a metal plate beneath the skin and applied periodic compressions using an external magnet. This method allows control over the size and severity of the injury by varying the number and duration of compressions, replicating features of human chronic wounds such as reduced blood flow, hypoxia, and immune cell influx. However, this technique is unsuitable for cranial defect studies due to interference with micro-CT scans from the metal. While diabetes models are beneficial for studying diabetes-related wounds, they may not be appropriate for trauma studies ^14,63,64^. Infection models, although relevant, pose challenges in controlling outcomes and may negatively impact further regeneration studies ^15^.
Our approach employs mechanical resistance to counteract wound centripetal contraction. Over time, chronic wounds exhibit significantly elevated levels of proinflammatory cytokines and matrix metalloproteinases, whereas activities of matrix metalloproteinase inhibitors and growth factors are reduced, thereby decelerating the healing process ^65–67^. Compared to previously described methods, our method is simpler to implement, more closely aligns with trauma-related composite defects, and effectively extends the duration of a non-healing wound.
In addition to mirroring clinical practice, ease of operation is crucial for animal models; rodents provide this advantage, both in terms of husbandry and surgical procedures. Rodents also provide the advantage of being genetically modifiable and thus the opportunity to evaluate knockout or knock-in effects of essential signaling pathways on composite tissue healing and bone regeneration ^68–77^.
To inhibit the proliferation of adherent granulation tissue during the splinting process, we employed POC as a barrier and a bio-release medium, combined with Vincristine (cell proliferation decelerator) and Kanamycin (antibiotics). POC has been demonstrated to have minimal cytotoxicity and immune response but increased cell compatibility. In our study, POC did not elicit any related adverse reactions. Instead, it significantly reduced dural adhesions, thereby simplifying the surgical environment for subsequent research.
The longest remaining duration of WO tested was 5 weeks, which showed no difference in wound healing speed between the obturator removed at 5 weeks and those removed at 3 weeks. Thus, we surmise that 3 weeks is sufficient for the obturator to bypass the peak healing period of the skin. This model, capable of maintaining a non-healing state for extended periods, is suitable not only for the development of regenerative strategies but also for investigating inflammatory pathways, and repair mechanisms of chronic composite defects.
CONCLUSION
We have successfully established a rat model of a scalp-cranial composite defect along with a unique complementary positive control, providing a stable platform for subsequent research. The experimental model effectively slowed the scalp healing process and preserved the cranial defect, embodying the characteristics of a “chronic composite defect”. The positive control exhibited reliable and reproducible healing through autologous reconstruction, mirroring current surgical practice.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Lee J. C., Kleiber G. M., Pelletier A. T., Reid R. R. & Gottlieb L. J. Autologous immediate cranioplasty with vascularized bone in high-risk composite cranial defects. Plast Reconstr Surg 132, 967–975, doi:10.1097/PRS.0b 013e 31829 f 4b 59 (2013).24076686 · doi ↗ · pubmed ↗
- 2Soto E., Restrepo R. D., Grant J. H.3rd & Myers R. P. Outcomes of Cranioplasty Strategies for High-Risk Complex Cranial Defects: A 10-Year Experience. Ann Plast Surg 88, S 449–S 454, doi:10.1097/SAP.0000000000003019 (2022).34670972 PMC 8986876 · doi ↗ · pubmed ↗
- 3Fong A. J. Reconstructive approach to hostile cranioplasty: A review of the University of Chicago experience. J Plast Reconstr Aesthet Surg 68, 1036–1043, doi:10.1016/j.bjps.2015.04.014 (2015).25971417 · doi ↗ · pubmed ↗
- 4Han G. & Ceilley R. Chronic Wound Healing: A Review of Current Management and Treatments. Adv Ther 34, 599–610, doi:10.1007/s 12325-017-0478-y (2017).28108895 PMC 5350204 · doi ↗ · pubmed ↗
- 5Shonka D. C.Jr., Potash A. E., Jameson M. J. & Funk G. F. Successful reconstruction of scalp and skull defects: lessons learned from a large series. Laryngoscope 121, 2305–2312, doi:10.1002/lary.22191 (2011).22020883 · doi ↗ · pubmed ↗
- 6Shimizu F. Algorithm for reconstruction of composite cranial defects using the fascial component of free anterolateral thigh flaps. J Craniofac Surg 24, 1631–1635, doi:10.1097/SCS.0b 013e 3182999 a 33 (2013).24036741 · doi ↗ · pubmed ↗
- 7Szpalski C., Barr J., Wetterau M., Saadeh P. B. & Warren S. M. Cranial bone defects: current and future strategies. Neurosurg Focus 29, E 8, doi:10.3171/2010.9.FOCUS 10201 (2010).21121722 · doi ↗ · pubmed ↗
- 8Wang H. A 3D biomimetic optoelectronic scaffold repairs cranial defects. Sci Adv 9, eabq 7750, doi:10.1126/sciadv.abq 7750 (2023).36791200 PMC 9931229 · doi ↗ · pubmed ↗