Spontaneous Pneumothorax in a Term Neonate
Badar Al Dhouyani, Amal R Al-Naimi

TL;DR
A full-term baby girl developed a rare spontaneous pneumothorax with no known risk factors and recovered without surgery.
Contribution
This case report highlights a rare occurrence of primary spontaneous pneumothorax in a term neonate with successful conservative treatment.
Findings
The neonate had a primary spontaneous pneumothorax with no identifiable risk factors.
Conservative management successfully resolved the pneumothorax without surgical intervention.
Abstract
Pneumothorax is a rare cause of respiratory distress in the newborn. We report our experience with a full-term female neonate who had primary spontaneous pneumothorax. No risk factors were identified. The pneumothorax was resolved completely with conservative management.
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
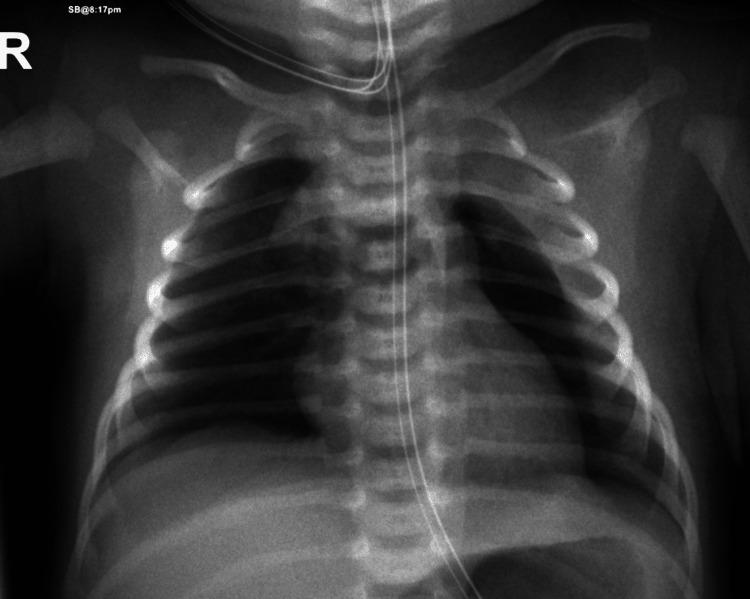 Figure 1
Figure 1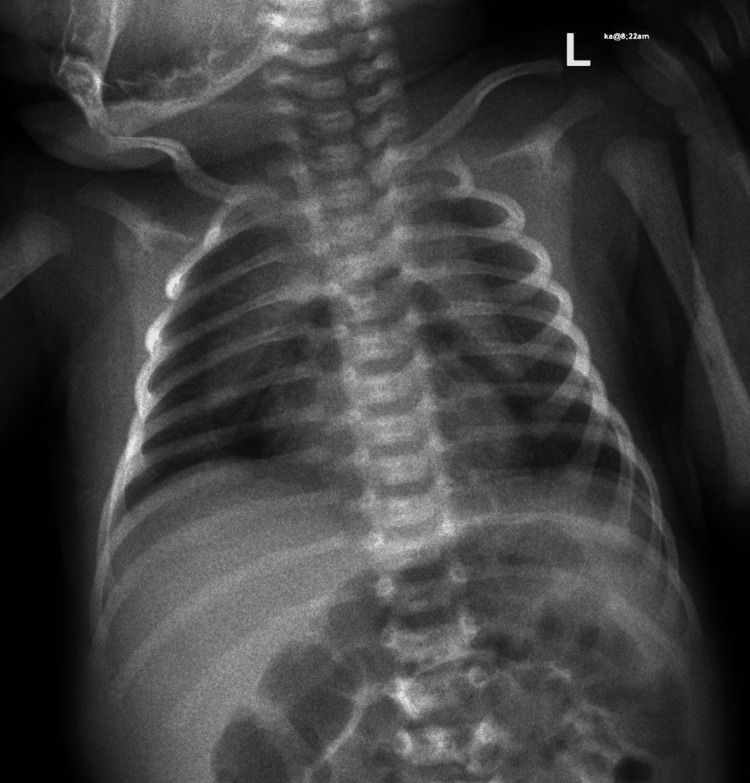 Figure 2
Figure 2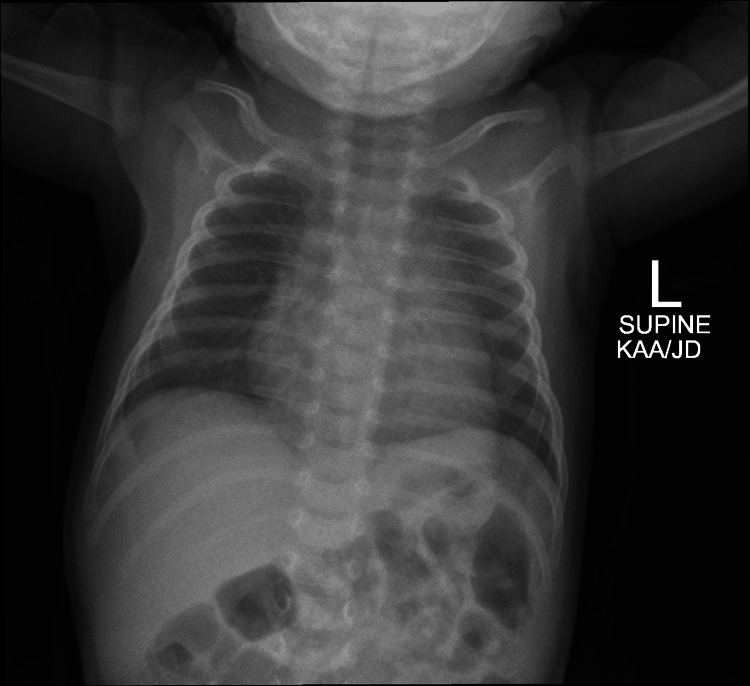 Figure 3
Figure 3| Variables | pH | pCo2 (mmHg) | HCO3 (mmol/L) | BE | Lactate |
| VBG at birth | 7.28 (7.31 - 7.41) | 53 (41 - 51) | 16 (23 - 28) | -7.9 (-2 - 3) | 6.6 |
| VBG after two hours | 7.34 (7.31 - 7.41) | 42 (41 - 51) | 22 (23 - 28) | -3 (-2 - 3) | 3.3 |
| Author | Gestational age | Gender | Age at presentation | Presenting symptoms | Management | outcome |
| Adekoya et al. [ | 38 weeks | Male | At birth | Tachypnea with increased work of breathing | Oxygen | Resolved spontaneously |
| Gharibvand et al. [ | Term | Male | At birth | Respiratory failure and shock | Intubated with no intervention | Extubated within two days and pneumothorax resolved spontaneously |
| Rocha et al. [ | 39 weeks | Male | Four hours of life | Grunting with subcutaneous emphysema | Oxygen | Resolved spontaneously at day nine |
| Karthikeyan et al. [ | 40 weeks | Male | At birth | Desaturation to 85% with increased work of breathing | Intubated with a chest tube. Antibiotic | Improved after 10 days |
| Haley et al. [ | 40 weeks | Male | At birth | Desaturation to 80% with tachypnea | Oxygen | Resolved spontaneously |
| Huseynov et al. [ | 36+5 weeks | Male | 24 hrs | Respiratory distress | Chest tube with blood patch | Improved after 2 days |
| James et al. [ | Term | Female | Within 1 hour of birth | Respiratory distress with desaturation 70% | Bilateral needle thoracentesis | Resolved completely |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsCongenital Diaphragmatic Hernia Studies · Neonatal Respiratory Health Research · Pleural and Pulmonary Diseases
Introduction
Pneumothorax is the presence of air between the parietal and visceral pleura of the thoracic cavity, with a consequent increase in intrapulmonary pressure. Like the Hermansen study [1], Lorah et al. found the incidence of spontaneous pneumothorax is 1-2% in term neonates, but it increases to about 6% in premature neonates. Pneumothorax can be secondary to infection, meconium aspiration, or ventilation barotrauma. The identified risk factors that can contribute to neonatal pneumothorax are male gender, low birth weight, prematurity, post-maturity, and aggressive resuscitation at birth [2]. Usually, affected neonates will develop acute respiratory distress soon after birth. Early suspicion and diagnosis are important. Management rarely exceeds conservative measures [2].
Case presentation
A full-term female neonate was delivered via spontaneous vaginal delivery with unremarkable antenatal history. There was no history of prolonged rupture of membrane or meconium-stained liquor, and she cried immediately. Apgar scores at birth were 8 and 9 at the first and fifth minutes, respectively. She started to have cyanosis and grunting at 10 minutes of life. On examination, she was a healthy baby with no dysmorphic features. Her birth weight was 2730g. The respiratory rate was 60 cycles per minute and the heart rate was 160 beats per minute. There was respiratory distress with nasal flaring and mild subcostal recession. Breath sounds were decreased bilaterally without any crepitations or wheezing. Other systemic examinations were unremarkable. Non-invasive ventilation (continuous positive airway pressure (CPAP): positive end-expiratory pressure (PEEP) 5, FiO2 30%) was initiated, and venous blood gas was done in Table 1. The first chest X-ray is shown in was obtained on the first day of life, which showed left-sided pneumothorax (Figure 1).
Left-sided pneumothoraxLeft-sided pneumothorax associated with a moderate amount of left-sided pleural effusion with a complete collapse of the left lung
Echocardiography was normal with no signs of pneumopericardium. The sepsis screen was negative. CPAP was applied for around nine hours then as her respiratory distress was improving, she was weaned to low flow oxygen 0.1-1 liters per minute via nasal cannula for 24 hours, then weaned to room air. Repeated chest X-ray after six days (Figure 2) showed evidence of pneumomediastinum.
PneumomediastinumShowed evidence of pneumomediastinum (air below the thymus)
On day nine, the CT chest showed mild-to-moderate anterior pneumomediastinum inferior to the thymus.
She was discharged home on day nine because she remained stable with no signs of respiratory distress. She did not require any surgical intervention in the form of chest tube placement or needle thoracentesis. After one month she was seen in the pulmonology clinic. She was active with no respiratory distress. Her O2 saturation was 99% on room air. She was thriving well; her weight was 3.9 kg (Z-score -0.67). Chest exam revealed equal vesicular breath sound bilaterally with no added sound. Repeated chest X-ray was normal (Figure 3).
Normal chest X-ray
Discussion
Respiratory distress is common in the early neonatal period. Multiple conditions can cause respiratory distress in term infants. The most common causes are Transient tachypnoea of the newborn, meconium aspiration syndrome, cardiac failure, pneumonia, and pneumothorax. Pneumothorax can be spontaneous or secondary to an underlying lung disease such as pneumonia, meconium aspiration, or mechanical ventilation [2].
Currently, there are no guidelines for effectively managing spontaneous pneumothorax in full-term neonates. The management of this condition can vary depending on the severity of the case. In less severe cases, careful observation may be employed, while more severe cases may require intercostal drainage to relieve the respiratory distress. Early detection is crucial, and aspiration of persistent pneumothoraxes in symptomatic infants should be considered [2]. Diagnosis can be delayed, especially if not suspected. In one study, it was shown that it takes between 0.5 and 27 hours before the clinical diagnosis is made. In that study, 46% of the neonates with pneumothorax displayed specific radiological signs such as the double diaphragm sign, enhanced cardio-mediastinal sharpness, deep sulcus sign, and basilar hyperlucency. These radiological signs can be helpful for early diagnosis [3].
Most cases won't require intervention, but chest tube insertion should be considered to allow lung expansion in symptomatic infants. Only 7.5% of symptomatic term infants with spontaneous pneumothorax would require chest tube insertion or thoracentesis [4]. The chest tube can be clamped for at least 24 hours after cessation of air leak. If there is no recurrence of pneumothorax, the chest tube can be removed [5]. In full-term or near-term neonates with spontaneous pneumothorax, the overall outcome is generally good. Infants who require prolonged oxygen therapy or positive pressure ventilation will have higher morbidity. In rare cases, subcutaneous emphysema and pulmonary hemorrhages may occur. Late complications such as bronchopulmonary dysplasia and neurodevelopmental impairment have also been documented. Neonates with primary lung disorders, such as congenital pneumonia or meconium aspiration syndrome at a high risk of developing pneumothorax and its associated complications [6]. It is crucial to closely monitor these cases and provide appropriate treatment and care to ensure the best possible outcomes. The goal is to optimize treatment approaches and minimize complications associated with this condition. Early detection and timely intervention are key factors in achieving better outcomes and reducing long-term morbidity [5,6].
The following table summarizes previously reported cases of term neonates with spontaneous pneumothorax without underlying conditions (Table 2).
Conclusions
Spontaneous pneumothorax in term is rare but a well-recognized cause of respiratory distress in the newborn. Timely diagnosis and adequate management reduce morbidity. Chest X-rays need to be considered in newborns with respiratory distress to rule out spontaneous pneumothorax because early recognition is lifesaving. Most cases resolve with conservative treatment and intervention is rarely required. Close and direct observation is the key to monitoring any respiratory deterioration. Spontaneous pneumothorax might require chest tube insertion if it causes severe respiratory distress or hemodynamic instability, which was reported in some cases.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Using the modified Delphi method to develop a tool to assess pediatric residents supervising on inpatient rounds Acad Pediatr Miller KA Collada B Tolliver D Audi Z Cohen A Michelson C Newman LR 89962020203140470610.1016/j.acap.2019.07.012 · doi ↗ · pubmed ↗
- 2Overview of respiratory care of the neonate, review article Arch Pharm Pract Alanazi SM 153162142023
- 3Pneumothorax and nasal continuous positive airway pressure ventilation in premature neonates: a note of caution ASAIO J Makhoul IR Smolkin T Sujov P 4764794820021229656510.1097/00002480-200209000-00006 · doi ↗ · pubmed ↗
- 4Pigtail catheters used in the treatment of pneumothoraces in the neonate Adv Neonatal Care Cates LA 71692009 https://journals.lww.com/advancesinneonatalcare/abstract/2009/02000/pigtail_catheters_used_in_the_treatment_of.10.aspx 1921215910.1097/01.ANC.0000346089.97615.71 · doi ↗ · pubmed ↗
- 5Epidemiologic survey of 196 patients with congenital central hypoventilation syndrome Pediatr Pulmonol Vanderlaan M Holbrook CR Wang M Tuell A Gozal D 2172293720041496681510.1002/ppul.10438 · doi ↗ · pubmed ↗
- 6Adopting a palliative approach to dementia care in the community: a participatory action research Singapore Med J Tan LL Ng WF Sim AC Rahim SB 2402436220213440947510.11622/smedj.2021064 PMC 8801855 · doi ↗ · pubmed ↗
- 7The association of cardiometabolic disorders with sleep duration: a cross-sectional study Afr Health Sci Prakaschandra DR Naidoo DP 27328322202210.4314/ahs.v 22i 4.32PMC 1011747937092078 · doi ↗ · pubmed ↗
- 8Spontaneous pneumomediastinum in a term neonate - case report Clin Case Rep Rocha G Guimarães H 314316620182944546910.1002/ccr 3.1352 PMC 5799620 · doi ↗ · pubmed ↗