Laryngitis Caused by Mycobacterium abscessus Subspecies massiliense Infection
Yu Kurahara, Yasuaki Shimatani

Abstract
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
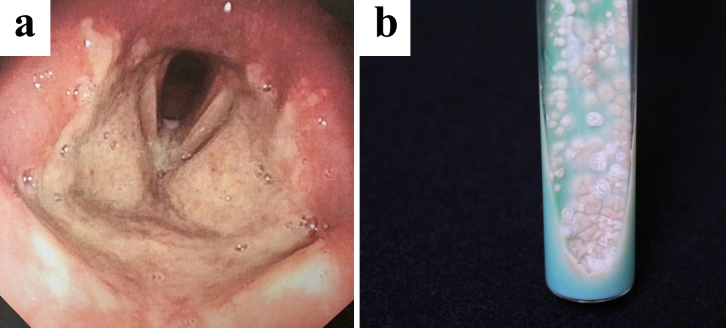 Figure 1
Figure 1Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsMycobacterium research and diagnosis · Infectious Diseases and Tuberculosis · Tuberculosis Research and Epidemiology
A 23-year-old woman visited our hospital with a 1-month history of laryngitis and presented with a sore throat 3 weeks after being diagnosed with COVID-19. Laryngoscopy revealed extensive erosion and a white coating in the larynx (Figure 1a). Rapidly growing mycobacteria were isolated from laryngeal tissue on 2% Ogawa egg medium (Figure 1b) and identified as Mycobacterium abscessus subspecies massiliense (Mma) using MALDI-TOF MS (Bruker Daltonics, Billerica, MA, USA) and DNA Chromatography MABC/erm(41) (Kaneka, Osaka, Japan). The patient’s skin did not show any signs of Mma infection, and no lung lesions were identified. She was later diagnosed with HIV infection. Her CD4 count was 376 cells/mm^3^.
This patient’s main symptom was initially suspected to be a sequela of COVID-19, but the eventual diagnosis was Mma laryngitis associated with HIV infection. Mma infections in the head and neck are rare ^(1)^. Clinicians should be aware that laryngitis that is resistant to therapy may in fact be a laryngeal nontuberculous mycobacterial infection, especially in immunocompromised patients. Furthermore, bacteriological investigation aimed at identifying specific pathogens is crucial for patients with atypical laryngitis.
Article Information
Conflicts of Interest
None
Author Contributions
YK wrote the draft of the manuscript and contributed to patient care. YS contributed to bacteriological examinations.
Informed Consent
Written informed consent was obtained from the patient by the corresponding author. The signed consent forms have been retained by the patient. Details of the patient have been anonymized as much as possible.
Approval by Institutional Review Board (IRB)
This report did not require IRB approval.
The reference list from the paper itself. Each links out to its DOI / PubMed record.