Investigation of Rate and Effective Factors on Discharge against Medical Advice in Psychiatric Patients Over a 10-Year Period
Zahra Ebnehoseini, Hediye Khorasani, Zahra Koohjani, Mina Zibaei, Amir Deghatipour, Ali Saghebi, Ali Reza Ebrahimi, Masoumeh Boroujerdi, Mohammad Reza Mehri, Hamed Tabesh

Abstract
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
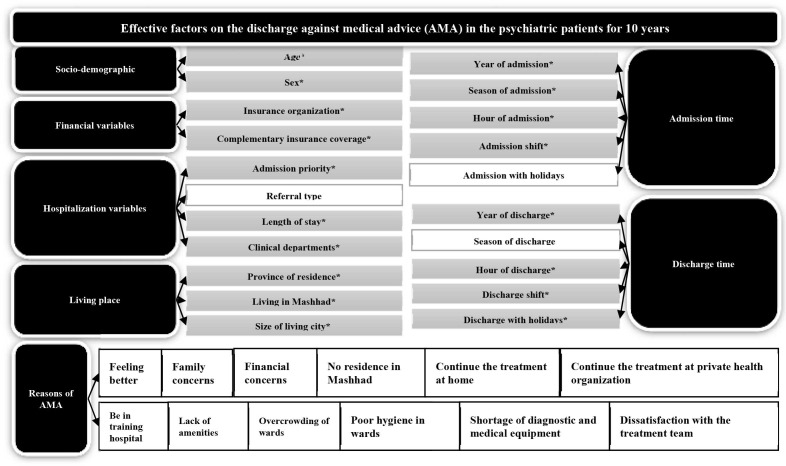 Figure 1
Figure 1Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsHealthcare Decision-Making and Restraints
Dear Editor
Discharge against medical advice (AMA) has a higher rate in the psychiatric ward than in other clinical wards. Discharge AMA increases both the patient’s and the hospital’s costs of delivering clinical care. In the present study, the frequency and effectiveness of discharge AMA factors were identified in the first encounter during a 10-year period using a large sample size.
This study used a cross-sectional design with retrospective hospital information system (HIS) data that was collected from Ibn-e-Sina Psychiatric Teaching Hospital in Mashhad, Iran, between 2010 and 2020 (research plan code: 951350). The present study was approved by the Ethical Committee of Mashhad University of Medical Sciences (code: IR.MUMS.MEDICAL.REC.1398.913). All first encounters with hospitalized patients in the HIS were extracted. The dependent variable was discharge AMA. The independent variables were socio-demographic, admission and discharge time, living place, hospitalization, and reasons for discharge AMA.
The demographics were obtained using descriptive statistics. The patients’ characteristics were compared using the Chi square test. Odds ratios (ORs) with a 95% confidence interval (CI) were reported for each independent variable. Most P values were two-sided, and P<0.05 was considered statistically significant.
During the study period, discharge AMA discharge accounted for 17% (3823 patients) of the total discharges (22468 patients) from the case hospital. Being male was associated with an increased risk for discharge AMA (OR=0.508, 95% CI=0.480-0.538). Age was significantly associated with discharge AMA (P<0.001).
The variables including admission time, admission shift, and season of admission were higher in discharge AMA than in non-discharge AMA (P<0.001). However, there was no statistically significant positive relationship between discharge AMA and admission with holidays.
The results showed a significant relationship between discharge AMA and discharge year (P<0.001). There was a considerable growth in the rate of discharge AMA. A significant difference was found between discharge AMA and discharge with holidays. The discharge AMA had a significant relationship with season of discharge (P<0.001), hour of discharge (P<0.001), and discharge shift (P<0.001).
The results indicated a significant one-sided relationship between the “province of residence” and discharge AMA (P=0.007). “Living in Khorasan province” was associated with an increased risk for discharge AMA ([OR=1.202, 95% CI=1.021-1.108] versus [OR=0.995, 95% CI=0.965-0.980] for non-discharge AMA). Moreover, “living in Mashhad” had a higher risk of discharge AMA ([OR=1.222, 95% CI=1.151-1.084] versus [OR=0.984, 95% CI=0.961-0.972] for non-discharge AMA).
Moreover, the findings of the present study demonstrated a positive relationship between the size of the city in which the patient lived and discharge AMA. The patients residing in large cities and towns experienced the most frequent discharge AMA.
Besides, a statistically significant relationship was found between insurance organizations and discharge AMA (P<0.001).
The most frequent discharge AMA was related to Health Service and Armed Forces Insurance Organizations. Complementary insurance coverage was associated with an increased risk of discharge AMA ([OR=1.911, 95% CI=1.386-1.628] versus [OR=0.927, 95% CI=0.822-0.873] for non-discharge AMA).
There was a significant difference between “admission priority” and discharge AMA. Discharge AMA rate in emergency admission (n=2215, 57.90%) was higher than non-emergency admission (n=1608, 42.10%). There was a significant relation between discharge AMA and “clinical departments” (P<0.001). The majority of the discharge AMA was discharged from the adult-male psychiatry department (41.5%), followed by adult-female psychiatry, girls’ pediatric psychiatry, and quit addiction. There was no significant difference between “Referral type” and discharge AMA. The risk of discharge AMA increased with length of stay <6 hours compared to ≥6 hours ([OR=3.167, 95% CI=2.3871-3.494] versus [OR=0.576, 95% CI=0.521-0.637] for non-discharge AMA). Figure 1 shows the effective factors on discharge AMA in psychiatric patients during a 10-year period.
The figure illustrates the effective factors of the discharge against medical advice in psychiatric patients for 10 years.
The findings of the present study highlighted the characteristics of psychiatry patients who were discharged from the hospital with discharge AMA. The frequency of discharge AMA was 17%. In contrast to the findings of the present study, the rate of discharge AMA was reported as 34% in a psychiatric hospital in northern Iran. ^ 1 ^ It seemed that the discharge AMA rate was different in various populations. ^ 2 ^ In addition, it was found that there was a significant association between discharge AMA and male sex as well as young age. This finding was consistent well with previous studies. ^ 3 , 4 ^ A rising rate of discharge AMA was observed. The prevalence of mental disorders increased from 1999 to 2014, by about 1.12-fold, ^ 5 ^ which might have contributed to discharge AMA in the study population.
The results of this research indicated a positive relationship between discharge AMA, admission, and discharge time. Brook and colleagues reported night and evening shifts were associated with discharge AMA. ^ 2 ^
Moreover, the present findings indicated a significant relationship between discharge AMA and the type of the patient’s insurance. It was found that the place of living and discharge AMA were associated with each other. However, the findings were not significant. Furthermore, clinical wards of “quit addiction” had a large number of discharge AMA.
The majority of grounds for the discharge AMA were related to the patients, including feeling better, financial problems, family issues, the physical condition of the hospital, and ineffective therapy.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Sheikhmoonesi F Khademloo M Pazhuheshgar S Patients discharged against medical advice from a psychiatric hospital in Iran: a prospective study Glob J Health Sci 201462138[ PMC Free Article ]10.5539/gjhs.v 6n 3p 21324762365 PMC 4825465 · doi ↗ · pubmed ↗
- 2Brook M Hilty DM Liu W Hu R Frye MA Discharge against medical advice from inpatient psychiatric treatment: a literature review Psychiatr Serv 2006571192810.1176/ps.2006.57.8.119216870972 · doi ↗ · pubmed ↗
- 3Alfandre DJ “I’m going home”: discharges against medical advice Mayo Clin Proc 20098425560[ PMC Free Article ]10.4065/84.3.25519252113 PMC 2664598 · doi ↗ · pubmed ↗
- 4Hayat AA Ahmed MM Minhas FA Patients leaving against medical advice: an inpatient psychiatric hospital-based study J Coll Physicians Surg Pak 201323342623673174 · pubmed ↗
- 5Noorbala AA Damari BRIAZIIS Evaluation of mental disorders incidence trend in Iran 2014;21:1-10