Preductal Hemodynamic Redistribution in Preterm Infants with Patent Ductus Arteriosus
Aimann Surak

TL;DR
This paper examines how an open blood vessel in preterm infants affects blood flow to the upper body.
Contribution
It presents case reports highlighting abnormal blood flow patterns in preterm infants with patent ductus arteriosus.
Findings
Three patients showed abnormal Doppler flow patterns in the brachiocephalic artery.
The study emphasizes the need for further research on preductal hemodynamics in preterm infants with PDA.
Abstract
A patent ductus arteriosus is a common entity in preterm infants. Literature is lacking regarding physiological effects on preductal circulation. This report describes 3 patients with abnormal flow Doppler pattern in brachiocephalic artery. Further research is warranted to better understand the impact of PDA on preductal circulation.
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
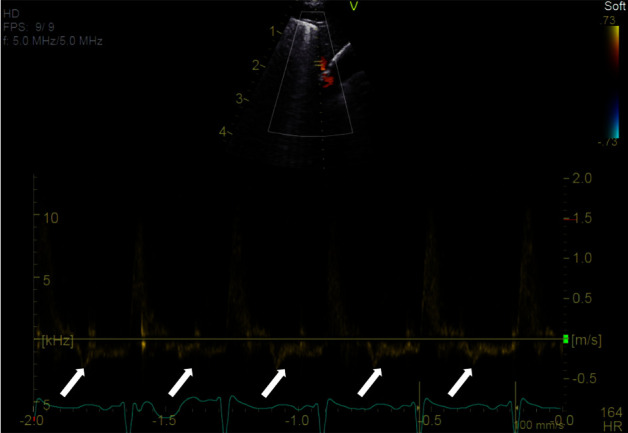 Figure 1
Figure 1Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsCardiovascular Conditions and Treatments · Congenital Heart Disease Studies · Cardiovascular and Diving-Related Complications
1. Introduction
A patent ductus arteriosus (PDA) is a common entity in preterm infants. Unlike in the term population, 57–70% of preterm infants weighing less than 1000 grams will still have an open PDA at 7–10 days of age [1]. Numerous studies described the physiological effects of the PDA, particularly a hemodynamically significant one. When hemodynamically significant, the immature pulmonary vascular bed in this population is exposed to variable degrees of volume overload. This contributes to neonatal morbidities including bronchopulmonary dysplasia, pulmonary haemorrhage, necrotizing enterocolitis, and life-threatening complications [2–5].
PDA is also associated with extra-pulmonary morbidities [5–7]. Historically, it was thought that preductal vessels were protected from the effects of left-to-right ductal shunting. This theory, however, is being re-examined. Lemmers et al. suggest that a persistent PDA may influence brain growth because of insufficient cerebral oxygenation thus affecting neurodevelopmental outcomes [8]. Breatnach et al. found that the brachiocephalic artery tended to have reversal of flow in infants with a PDA at 5 to 7 days of age, whereas those without a PDA had forward flow in this artery postulating that reversal of flow may be an early indicator of impaired cerebral circulation [9]. Sellmer et al. showed that a large PDA early on is associated with a 6-fold increase in the development of an intraventricular haemorrhage (IVH) [10].
The definition of hemodynamically significant PDA has not been standardized [11, 12]. However, it appears that detailed echocardiographic assessment looking at multiple indices is the key to assessing the hemodynamic significance using TnECHO.
2. Case Report
We are reporting 3 cases of preterm infants with hemodynamically significant PDAs confirmed by targeted neonatal echocardiogram (TnECHO), presenting with abnormal brachiocephalic artery flow Doppler pattern. Table 1 summarizes the patients' clinical characteristics, and Table 2 summarizes their PDA characteristics. From the arch view, the brachiocephalic artery was visualized and Dopplered during the echocardiogram. Each of these patients had abnormal Doppler flow pattern in the brachiocephalic artery shown as reversal of diastolic flow (Figure 1).
3. Discussion
In this clinical case, we report on three preterm infants with hemodynamically significant PDAs beyond the first week of life. All three infants were noted to have a reversal of diastolic blood flow in the brachiocephalic artery upon assessment by TnECHO, and all were found to have varying degrees of intraventricular hemorrhage. Those scans were the first scans for those infants when they were diagnosed with hemodynamically significant PDA with different ages at the diagnosis for the infants. Also, unfortunately, the subsequent follow-up scans did not interrogate the brachiocephalic flow Doppler pattern. Infants developed mild BPD diagnosed at 36 weeks corrected, but all infants came off respiratory support and were discharged home between 38 and 40 weeks corrected gestation. There are no other insignificant morbidities.
Establishing the impact of the PDA and its significance is a comprehensive process combining clinical, radiological, chemical, and echocardiographic assessment. While a causal relationship cannot be established based on this case report, it appears that a hemodynamically significant PDA might be associated with abnormal Doppler flow patterns in the brachiocephalic artery of preterm infants. Whether this is related to flow redistribution or steal phenomenon remains unclear. There is a paucity of literature on this subject, and therefore, further studies investigating the relationship between abnormal brachiocephalic artery Doppler flow, hemodynamically significant PDAs, and the development of IVH are warranted. As the brachiocephalic artery is easily interrogated and easy to Doppler, if abnormal, this should alert clinicians to the possibility of developing an IVH.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Gillam-Krakauer M. Reese J. Diagnosis and management of patent ductus arteriosus Neo Reviews 2018197 e 394e 40210.1542/neo.19-7-e 3942-s 2.0-8505175689230505242 PMC 6269146 · doi ↗ · pubmed ↗
- 2Weisz D. E. Mirea L. Rosenberg E. Association of patent ductus arteriosus ligation with death or neurodevelopmental impairment among extremely preterm infants JAMA Pediatrics 2017171544344910.1001/jamapediatrics.2016.51432-s 2.0-8501878894628264088 PMC 5470355 · doi ↗ · pubmed ↗
- 3Reese J. Shelton E. L. Slaughter J. C. Mc Namara P. J. Prophylactic indomethacin revisited The Journal of Pediatrics 20171861114.e 110.1016/j.jpeds.2017.03.0362-s 2.0-8501713028428396028 PMC 5520627 · doi ↗ · pubmed ↗
- 4Semberova J. Sirc J. Miletin J. Spontaneous closure of patent ductus arteriosus in infants ≤1500 g Pediatrics 2017140210.1542/peds.2016-42582-s 2.0-8502667194428701390 · doi ↗ · pubmed ↗
- 5Palder S. B. Schwartz M. Z. Tyson K. R. T. Marr C. C. Association of closure of patent ductus arteriosus and development of necrotizing enterocolitis Journal of Pediatric Surgery 198823542242310.1016/s 0022-3468(88)80439-12-s 2.0-00239125143379548 · doi ↗ · pubmed ↗
- 6de Waal K. Phad N. Collins N. Boyle A. Cardiac remodeling in preterm infants with prolonged exposure to a patent ductus arteriosus Congenital Heart Disease 201712336437210.1111/chd.124542-s 2.0-8501343649228225202 · doi ↗ · pubmed ↗
- 7Vaisbourd Y. Sharif D. Riskin A. The effect of patent ductus arteriosus on coronary artery blood flow in premature infants: a prospective observational pilot study Journal of Perinatology 20204091366137410.1038/s 41372-020-0622-432080335 PMC 7222133 · doi ↗ · pubmed ↗
- 8Lemmers P. M. A. Benders M. J. N. L. D’Ascenzo R. Patent ductus arteriosus and brain volume Pediatrics 2016137410.1542/peds.2015-30902-s 2.0-8496248441227030421 · doi ↗ · pubmed ↗