Comparison of the Latarjet Procedure and Iliac Crest Bone Graft Transfer in Bone Bankart Lesions in Recurrent Anterior Shoulder Dislocations
Mahmut Tuncez, Ömer Berkay Bayraktar

TL;DR
This study compares two surgical procedures for treating bone injuries in recurring shoulder dislocations and finds that both are effective, though one takes longer to perform.
Contribution
The paper provides a direct comparison of clinical and radiological outcomes between the Latarjet procedure and iliac crest bone graft transfer for bony Bankart lesions.
Findings
Both procedures showed similar clinical and radiological outcomes in terms of age, motion, and scores.
The iliac crest bone graft transfer had a significantly longer operation time than the Latarjet procedure.
Abstract
Objective: There are various treatment modalities for bony Bankart lesions following glenohumeral joint dislocations. In this research, we aimed to compare the radiological and clinical results of patients who underwent the Latarjet procedure and iliac crest bone graft transfer. Materials and methods: Clinical and radiological data of 15 patients were retrospectively evaluated. Inclusion criteria were a history of at least two dislocations, being between 18-65 years of age and having at least 10% glenoid bone loss. The exclusion criteria were defined as follows: patients who underwent only soft tissue procedures, patients who did not attend the follow-up, patients with other pathology in the upper extremity (fracture, cuff tear, etc.), and patients with a follow-up period of less than 12 months time. Nine patients underwent the Latarjet procedure and six underwent iliac crest bone…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
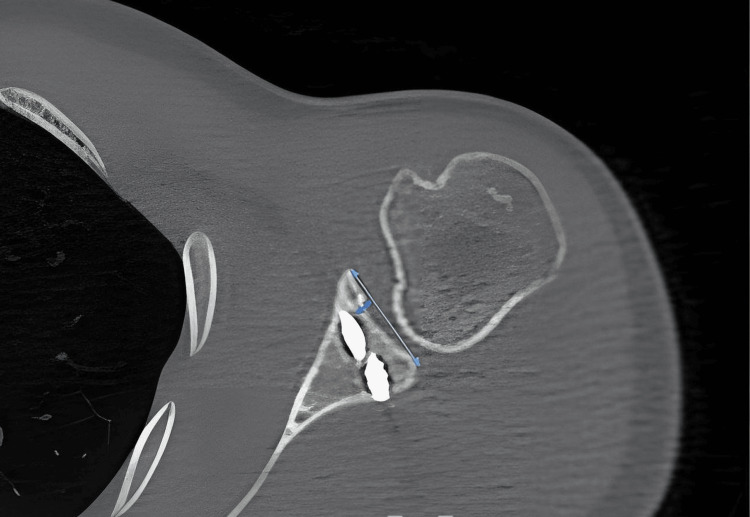 Figure 1
Figure 1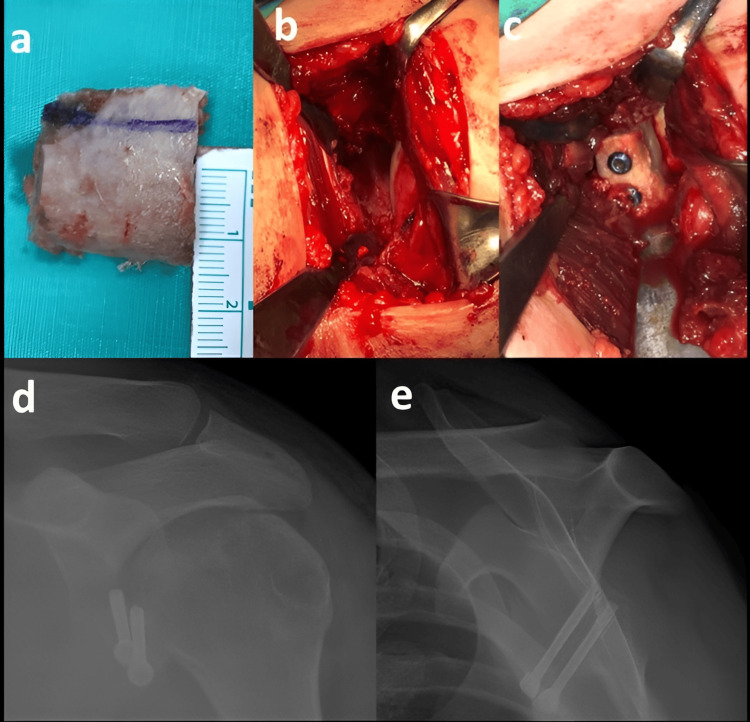 Figure 2
Figure 2| Parameters | Mean | Median | SD | Min | Max | IQR |
| Age (years) | 32.6 | 32 | 8.5 | 21 | 47 | 26-39 |
| Body mass index (kilogram/meter2) | 24.01 | 24.4 | 4.8 | 16.7 | 31.4 | 19-27 |
| Duration of surgery (minute) | 59.6 | 60 | 11.7 | 40 | 75 | 50-70 |
| Duration of hospital stay (day) | 2.9 | 3.0 | 0.79 | 2 | 4 | 2-4 |
| Total follow-up time (month) | 24.9 | 27 | 10.2 | 12 | 42 | 13-34 |
| Number of instability episodes | 5.06 | 5 | 2.4 | 2 | 11 | 3-7 |
| Glenoid cartilage Stepping (mm) | 0.06 | 0 | 0.16 | -0.2 | 0.3 | 0-0.2 |
| Glenoid Bone defect (%) | 15.2 | 15 | 2.9 | 10 | 22 | 13-17 |
| Constant score | 84.2 | 84 | 10.4 | 65 | 100 | 79-94 |
| QDASH | 15.1 | 6.8 | 14.2 | 2.3 | 36.4 | 4.5-36 |
| VAS | 2.8 | 3 | 1.7 | 1 | 8 | 1-3 |
| Forward elevation (degree) | 168 | 180 | 18.5 | 110 | 180 | 160-180 |
| Abduction (degree) | 154 | 160 | 15.9 | 100 | 170 | 150-160 |
| Internal rotation (degree) | 42.3 | 35 | 12.7 | 30 | 60 | 30-55 |
| External Rotation (degree) | 76.6 | 80 | 4.8 | 70 | 80 | 70-80 |
| Back to work (month) | 2.3 | 2 | 0.7 | 0.5 | 3.0 | 2-3 |
| Parameters | Latarjet (n=9) | ICBGT (n=6) | p |
| Age (years) | 34±8.4 | 30.6±9.1 | 0.483 |
| Body mass index (kilogram/meter2) | 23,9±5,3 | 24,1±4,4 | 0.944 |
| Duration of surgery (minute) | 54.4±6.8 | 67.5±13.6 | 0.028 |
| Duration of hospital stay (day) | 3±0,8 | 2,8±0,7 | 0.707 |
| Total follow-up time (month) | 23,1±12 | 27,6±6,9 | 0.419 |
| Number of instability episodes | 5,3±2,6 | 4,6±2,1 | 0.617 |
| Glenoid cartilage Stepping (mm) | 0±0,1 | 0±0,1 | 0.847 |
| Bone defect (%) | 15,3±3,6 | 15,1±1,7 | 0.918 |
| Constant score | 82,4±11,3 | 87±9,2 | 0.430 |
| QDASH | 11,3±11,6 | 20,8±17 | 0.301 |
| VAS | 2,2±1 | 3,6±2,3 | 0.157 |
| Forward elevation (degree) | 168,8±23,1 | 166,6±10,3 | 0.240 |
| Abduction (degree) | 150±19 | 160±6,3 | 0.158 |
| Internal rotation (degree) | 44,4±13 | 39,1±12,8 | 0.461 |
| External Rotation (degree) | 76,6±5 | 76,6±5,1 | >0.999 |
| Back to work (month) | 2,4±0,5 | 2±0,9 | 0.465 |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsShoulder Injury and Treatment · Shoulder and Clavicle Injuries · Orthopedic Surgery and Rehabilitation
Introduction
Nowadays, in the emergency department, half of the patients presenting with dislocations are shoulder dislocation patients. In 90% of shoulder dislocations, anterior shoulder dislocation occurs and is mostly treated with closed reduction. The pathology causing the dislocation is injury of the anterior glenoid labrum or Bankart lesion. However, an associated bone defect in the glenoid and/or humeral head may occur [1]. Soft tissue stabilisation procedures for the treatment of anterior shoulder instability have proven to be less effective in patients with extensive glenoid bone loss [2]. Therefore, in case of bone loss, bone tissue procedures are needed instead of soft tissue procedures. These procedures are of two types: coracoid transfer techniques and free bone grafting techniques. The commonly used coracoid transfer procedure is the modern type Latarjet procedure, which involves transferring the coracoid to the anterior glenoid rim through a permanent horizontal incision of the subscapularis muscle [3,4]. Other methods include the modern Eden-Hybinette procedure, a commonly used free bone transfer technique, or the iliac crest bone graft transfer (ICBGT), which involves harvesting an autologous bone graft from the iliac crest and transferring it to the anterior glenoid margin [5,6]. The aim of Latarjet and ICBGT is to create a mechanical block on the anterior glenoid margin. The aim of this research was to compare clinically and radiologically recurrent shoulder dislocation patients treated with these two techniques.
Materials and methods
Our research was conducted as a retrospective controlled study with approval from Izmir Katip Celebi Universıty Non-Interventional Clinical Studies Institutional Review Board (approval number 26). Of the 35 patients operated on for anterior shoulder dislocation in our clinic between January 2021 and May 2023, 15 patients operated on for bone Bankart lesions were included in the study. Inclusion criteria were a history of at least two dislocations, being between 18-65 years of age, and having at least 10% glenoid bone loss. Exclusion criteria were as follows: patients treated with only soft tissue procedure, patients who did not attend the follow-up, patients with other pathology in the upper extremity (old fracture, cuff tear, neurological deficit), and patients with a follow-up period of less than 12 months.
Nine patients were treated with the Latarjet procedure and six with ICBGT. Clinical evaluation was performed by age, gender, body mass index, range of motion, Quick Disabilities of the Arm, Shoulder and Hand (QDASH) score, Visual Analogue Scale (VAS) score and Constant score. Radiographic evaluation included preoperative and postoperative direct radiographs and computed tomography analysis. On computed tomography; bone defect percentage and postoperative glenoid cartilage stepping were measured. The glenoid bone defect was measured using the Pico method [7]. Glenoid cartilage stepping was measured between the intact glenoid and the graft using transverse computed tomography sections (Figure 1).
The mediolateral distance between the graft surface and the bony glenoid surface: glenoid cartilage stepping
Mann-Whitney U test, t-test, and Fisher exact test were used for group comparisons. In all reported tests, p<0.05 was considered statistically significant.
The Latarjet procedure was performed with a 6-8 cm incision between the coracoid and the anterior axillary line, leaving the pectoralis minor tendon-free. Conjoint tendon and coracoacromial ligaments were left intact and osteotomy of the coracoid near the base was performed. The glenohumeral joint was reached after vertical separation of the capsule with the transverse insertion of the subscapularis muscle. Then, the fibrous tissues in the anteroinferior part of the glenoid were removed and the blood supply of the glenoid bone with the burr was ensured. Following the transposition of the coracoid to the anterior glenoid margin flush with the glenoid articular surface and fixation to the glenoid with two screws, the procedure was terminated with anatomical closure of the subscapularis muscle. In the ICBGT technique, a rectangular (20x15 mm) tricortical bone graft was taken from the iliac crest, and the bone block was fixed to the anterior glenoid anteriorly in the same manner as the latarjet procedure (Figure 2).
Intraoperative images and postoperative radiographsa) Autogenous bone graft (20 x 15 mm) taken from the iliac crest. b) Preparation of the anterior glenoid rim. c) Fixation of the autogenous bone graft with two 3.5 mm cannulated screws. d-e) Postoperative direct radiographs.
Patients were followed up with passive shoulder movements between two and six weeks after two weeks in a shoulder arm sling. In the sixth week, active strengthening exercises were started.
Results
The mean age was 32.6 ± 8.5 years and the mean follow-up period was 24.9 ± 10.2 months. The mean Constant score was 84.2 ± 10.4, mean QDASH 15.1 ± 14.2, mean VAS 2.8 ± 1.7, mean internal rotation degree 42.3 ± 12.7 and mean glenoid bone defect percentage 15.2 ± 2.9%. Other categorical and demographic changes are shown in Table 1. These are the final follow-up results of all patients in both patient groups.
When the patients were analyzed as latarjet and ICBGT, no statistical difference was found in terms of age, gender, body mass index, range of motion, Constant score, VAS score, glenoid cartilage stepping, and bone defect (p>0.05) (Table 2). However, we found that the ICBGT group had a statistically longer operation time than the latarjet group (p<0.05) (Table 2). No postoperative complications were observed in either patient group (wound problem, infection, arthritis, neurological disorder, dislocation, etc.).
Discussion
The main finding of our study was that there was no difference between Latarjet and ICBGT clinically and radiologically. However, it was found that the operation time was statistically significantly prolonged in the ICBGT group compared to the Latarjet group. We attribute this difference to the prolonged operation time of the ICBGT group because two different incisions were used during the operation. In a previous prospective study by Moroder et al., the same two techniques were compared, and similar results were obtained with our study and it was shown that there was no difference in clinical outcome [8]. Moroder et al. obtained better results in shoulder internal rotation in the ICBGT group compared to the Latarjet group and attributed this to the permanent division of the subscapularis tendon in the latarjet procedure [8]. In our study, we did not find any statistical difference between the range of motion and internal rotation between both groups.
The two surgical techniques were performed by one senior surgeon with a special focus on shoulder surgery in our hospital. The duration of surgery was longer in the ICBGT group than in the latarjet group. We think that the reason for this is that the bone graft was taken from the iliac crest through a separate incision. In the literature, we could not find any study comparing the two groups in terms of surgical times. However, Razaenian et al. compared latarjet and arthroscopic ICBGT and found that arthroscopic ICBGT had a longer duration of surgery [9].
The selected cut-off value of 10% glenoid bone loss is not commonly accepted. A defect size of 13.5% has been referred to as "subcritical bone loss" by some authors [10,11]. These results show that when only soft tissue stabilization is performed, significantly worse results occur in patients with high activity in the presence of bone Bankart [10,11]. The mean age of our patient group was 32.6 years and mostly male patients with high activity. For these reasons, the authors used this cut-off value. When the two groups were evaluated in terms of postoperative instability, no postoperative subluxation was observed in any patient. We think that this is due to the fact that both techniques were successful in terms of stabilization [8,12-15].
The limitations of the study include the relatively small number of patients and its retrospective nature. However, we think that our study may contribute to the literature since these surgeries for bone defects in anterior shoulder dislocation are rarely performed routinely. In the future, prospective studies with a larger number of patients will be guiding to evaluate the effectiveness of both techniques in bone Bankart lesions.
Conclusions
There is still no gold-standard treatment for anterior shoulder instability with glenoid bone loss. Latarjet and ICBGT procedures do not show any difference in clinical and radiological outcomes except for a significantly longer operative time in the ICBGT group. Both procedures can be performed successfully in bone Bankart lesions.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Recurrent shoulder instability: current concepts for evaluation and management of glenoid bone loss J Bone Joint Surg Am Provencher MT Bhatia S Ghodadra NS 13315192 Suppl 220102112359710.2106/JBJS.J.00906 · doi ↗ · pubmed ↗
- 2Traumatic glenohumeral bone defects and their relationship to failure of arthroscopic Bankart repairs: significance of the inverted-pear glenoid and the humeral engaging Hill-Sachs lesion Arthroscopy Burkhart SS De Beer JF 6776941620001102775110.1053/jars.2000.17715 · doi ↗ · pubmed ↗
- 3A propos du traitement des luxations récidivantes de l’épaule Lyon Chir Latarjet M 994100349195413234709 · pubmed ↗
- 4Open Latarjet procedure for management of bone loss in anterior instability of the glenohumeral joint J Shoulder Elbow Surg Young AA Maia R Berhouet J Walch G 0920201110.1016/j.jse.2010.07.02221145262 · doi ↗ · pubmed ↗
- 5Open reconstruction of large bony glenoid erosion with allogeneic bone graft for recurrent anterior shoulder dislocation Am J Sports Med Weng PW Shen HC Lee HH Wu SS Lee CH 179217973720091948307610.1177/0363546509334590 · doi ↗ · pubmed ↗
- 6The J-bone graft for anatomical glenoid reconstruction in recurrent posttraumatic anterior shoulder dislocation Am J Sports Med Auffarth A Schauer J Matis N Kofler B Hitzl W Resch H 6386473620081800667310.1177/0363546507309672 · doi ↗ · pubmed ↗
- 7Intra-observer and interobserver reliability of the 'Pico' computed tomography method for quantification of glenoid bone defect in anterior shoulder instability Skeletal Radiol Magarelli N Milano G Sergio P Santagada DA Fabbriciani C Bonomo L 107110753820091946640610.1007/s 00256-009-0719-5 · doi ↗ · pubmed ↗
- 8Neer Award 2019: Latarjet procedure vs. iliac crest bone graft transfer for treatment of anterior shoulder instability with glenoid bone loss: a prospective randomized trial J Shoulder Elbow Surg Moroder P Schulz E Wierer G Auffarth A Habermeyer P Resch H Tauber M 129813072820193112901710.1016/j.jse.2019.03.035 · doi ↗ · pubmed ↗