Complete percutaneous coronary revascularization: An elegant solution to left ventricular dysfunction caused by severe coronary artery disease
Stefan Milutinovic, Kamaldeep Singh, Stevan Oluic, Juan C. Lopez‐Mattei, Ricardo O. Escárcega

TL;DR
This paper discusses how Impella-assisted complex PCI can successfully treat severe coronary artery disease in high-risk patients.
Contribution
The study highlights the effectiveness of Impella-assisted PCI in improving outcomes for surgically turndown patients.
Findings
Impella-assisted PCI achieves high technical success in complex cases.
It improves quality of life and angina scores in high-risk patients.
There is potential improvement in left ventricular ejection fraction.
Abstract
With increased complexity in both medical comorbidities and coronary anatomy, the proportion of surgically turndown patients and high‐risk PCI will continue to rise. Impella‐assisted complex PCI can be performed with high technical success and can improve quality of life, angina score, and potentially left ventricular ejection fraction. Coronary angiogram pre‐ and post‐ protected percutaneous coronary intervention in a surgical turndown with a multivessel coronary artery disease.
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
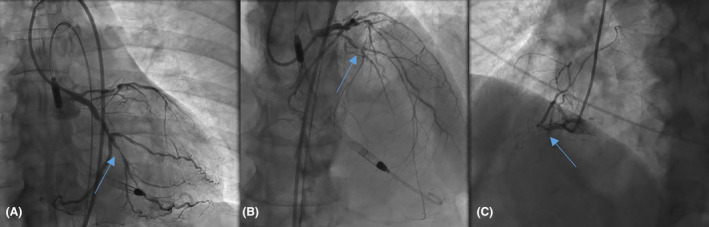 FIGURE 1
FIGURE 1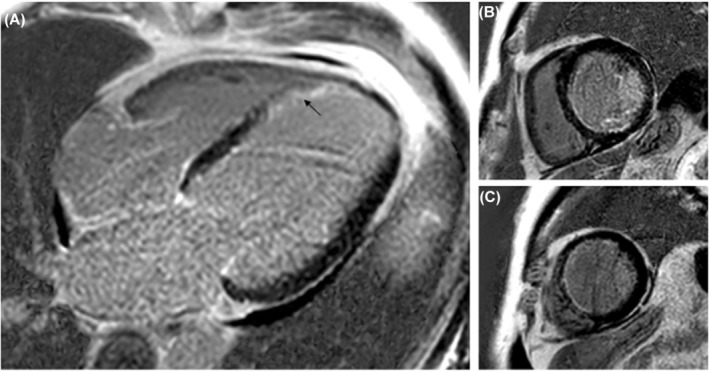 FIGURE 2
FIGURE 2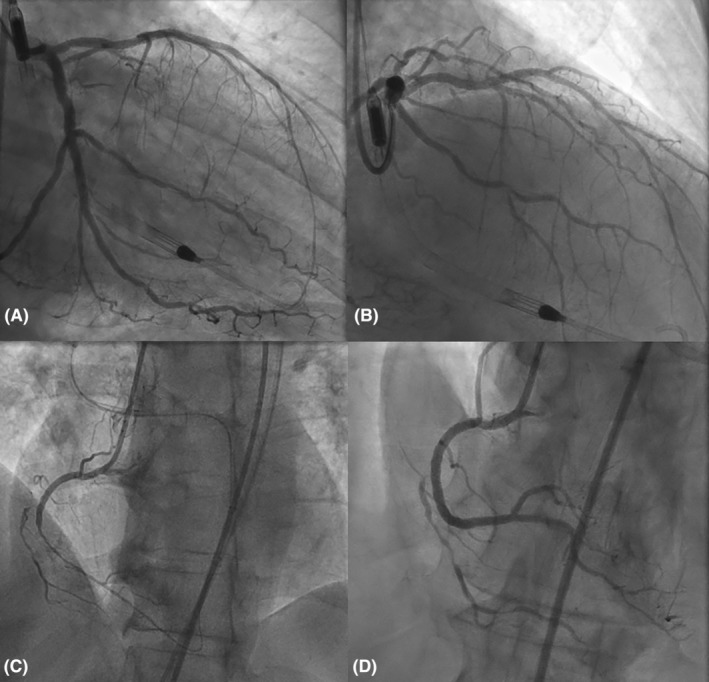 FIGURE 3
FIGURE 3Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsCoronary Interventions and Diagnostics · Cardiac Imaging and Diagnostics · Cardiac, Anesthesia and Surgical Outcomes
INTRODUCTION
1
Many patients with heart failure (HF) also have coronary artery disease (CAD), with an estimated prevalence of 50%–65%.1 Recent data indicate that CAD has become the most common cause of HF, surpassing hypertension and valvular heart disease.2 CAD significantly increases the risk of developing HF, whether it presents with reduced or preserved ejection fraction.3 Despite limited evidence regarding the risk of all‐cause and cardiovascular mortality, the 2021 Expert Consensus Pathway for Optimization of Heart Failure Treatment recommends coronary revascularization for appropriate patients.4, 5 Whether percutaneous coronary intervention (PCI) or coronary artery bypass surgery (CABG) is preferred, patients with complex coronary occlusions who are not suitable surgical candidates are increasingly referred for hemodynamic‐supported complex percutaneous revascularization.
CASE PRESENTATION
2
Case history
2.1
A 64‐year‐old male patient with hypertension, smoking, and alcohol use was admitted to the hospital with worsening scrotal and lower extremity swelling.
Differential diagnosis, investigations, and treatment
2.2
An initial cardiac evaluation revealed elevated troponin and pro‐BNP levels. The echocardiogram showed severe global hypokinesis with a left ventricular ejection fraction (LVEF) of 20%. Coronary angiography revealed multivessel coronary artery disease, including chronic total occlusion (CTO) of the right coronary artery with collaterals from the left coronary system (Figure 1). To fully characterize the territories needing revascularization, MRI viability study was obtained, cardiac magnetic resonance (CMR) showed viable myocardium at RCA, circumflex, and predominantly viable left anterior descending coronary artery (LAD), except for distal apical septal segment. (Figure 2). Due to the severity of CAD, the patient was referred for CABG. However, given the risk for surgery in the setting of poor left ventricular function and poor target arteries for bypass surgery, he was deemed not a good candidate by the heart team.
Left (A, B) and right (C) coronary systems showing multivessel coronary artery disease, including chronic total occlusion of the right coronary artery, which fills with collaterals from the left coronary system, subtotally occluded proximal calcified LAD, 70%–80% proximal and 70% mid left circumflex stenosis.
Viability assessment with cardiac MRI: Panel (A) shows late gadolinium enhancement (LGE) acquisition in four Chamber plane with a transmural infarction at distal apical septal segment (see arrow). Panel (B) shows LGE images in short axis plane with mid inferoseptal and mid inferior subendocardial infarction. Panel (C) shows proximal apical septal segments with subendocardial infarction. These findings were consistent with viable RCA and circumflex territories and predominantly viable LAD, with non‐viable distal apical septal segment.
Outcome and follow‐up
2.3
After a thorough evaluation of his anatomy, the patient underwent percutaneous revascularization in two settings: first, multivessel PCI with Impella CP (Abiomed, Danver, Massachusetts) support (Figure 3A,B) of LAD and Circumflex. Furthermore, the patient subsequently underwent CTO PCI to achieve complete revascularization. The CTO PCI of the right coronary artery was performed via a primary retrograde approach with the placement of two drug‐eluting stents (Figure 3C,D). After complete revascularization, the patient's symptoms have improved significantly with the marked reduction in his NYHA class. Three months later, the patient was NYHA Class I and his echocardiogram showed a significant recovery in LVEF to 45%–50% (Video 1).
(A, B) Successful multivessel PCI with Impella support, PCI of proximal to distal circumflex with two drug‐eluting stents, and successful rotational atherectomy of proximal LAD with two drug‐eluting stents. (C, D) Successful CTO PCI in retrograde fashion of the right coronary artery.
Improvement in LVEF status‐post‐multivessel PCI and CTO revascularization of RCA: Panel (A) shows a 2D Echo clip where significant segmental hypokinesis can be appreciated prior to complex coronary intervention (LVEF was 20%–25%). Panel (B) shows significant improvement in hypokinetic segments, with an LVEF of 45%–50%.
DISCUSSION
3
Surgical revascularization is a favorable strategy for patients with diabetes, left main disease, and multivessel coronary artery disease. However, approximately 20% of these patients may not qualify for surgery due to various reasons, such as subjective decision‐making by operators, inadequately accounted factors in surgical risk models (e.g., poor targets), exclusion from clinical trials, a historical preference for PCI as the primary treatment, and limited recommendations from societal guidelines.4 The main goal of the surgical approach is to ensure complete revascularization, particularly in patients receiving three or more grafts, as this has been associated with improved survival compared to those receiving fewer than three grafts.6 This goal has been extrapolated to percutaneous revascularization, but its applicability to stable coronary disease remains controversial due to inconsistent data. However, in patients with acute coronary syndromes and ST‐segment elevation, complete percutaneous revascularization has been shown to improve outcomes.7 During PCI, the completeness of revascularization is crucial, as a higher residual SYNTAX score is associated with worse 5‐year mortality.8
CTO is defined as the complete non‐acute occlusion of the coronary artery for at least 3 months. Coronary CTO PCI is a complex procedure that requires additional training and a deep understanding of various techniques. It involves multiple radial and/or femoral access points, adding to the complexity. There are four main strategies for crossing the CTO lesion: anterograde wire escalation, anterograde dissection and re‐entry, retrograde wire escalation, and retrograde dissection and re‐entry.9 Multiple wires, each with different degrees of stiffness, coating, and maneuverability, can be used to navigate through the true lumen or subintimal space. The retrograde approach involves accessing the lesion distally via collaterals and is used in more complex anatomical settings or when the anterograde approach has failed. However, it carries a higher risk of periprocedural complications. Meta‐analysis has found that PCI of CTO lesions has higher odds of in‐hospital cardiac death and cardiac tamponade compared to PCI of non‐CTO lesions.10 Additionally, the same meta‐analysis reported that the CTO group had a lower procedural success rate and higher major adverse cardiac outcomes during clinical follow‐up. An important limitation of CTO PCI is that procedural outcomes can be operator and center‐dependent. Higher‐volume operators (>60 CTO PCI) tend to perform this high‐complexity procedure with higher technical and procedural success rates.11 Nonetheless, CTO PCI is considered an essential part of complex high‐risk intervention procedures for indicated patients and is increasingly viewed as an alternative to coronary artery bypass graft surgery. Mechanical circulatory support (MCS), specifically the Impella device, has been used to facilitate complex PCI.12, 13
Hemodynamically supported revascularization is commonly performed in patients with an LVEF of ≤35%, but it is not exclusive to this group. Despite advancements in procedural techniques, equipment, and the implementation of a systematic hybrid approach, CTO PCI still faces challenges due to the high‐risk characteristics of many patients, particularly those with impaired left ventricular function.14, 15 Different technical success rates for CTO PCI have been reported in the literature. The 2021 PROGRESS‐CTO Registry demonstrates a high technical success rate of 85% and a low incidence of in‐hospital major adverse cardiac events (MACE) at 2.1%.16 Data have also shown that the retrograde technique, as in our case, can increase the technical success rate, but it is associated with increased rates of complications.17, 18
The effectiveness of CTO PCI in relieving angina has been well established. Following the procedure, our patient reported significant symptomatic relief at a three‐month follow‐up visit. Several studies have demonstrated improved angina symptoms following successful CTO PCI.19, 20 Compared to patients with unsuccessful CTO PCI, the OPEN‐CTO registry reported statistically significant improvements in the Seattle Angina Questionnaire Quality of Life Score and Rose Dyspnea Scale score.21 Similarly, the European CTO Club reported improvements in dyspnea and angina after a follow‐up period of 23 months.22
Although data has significant limitations, CTO PCI does not appear to affect all‐cause mortality (one‐year relative risk [RR] 1.70, 95% CI 0.50–5.80, and four‐year RR 1.77, 95% CI 0.19–16.06), myocardial infarction (one‐year RR 1.01, 95% CI 0.43–2.36, and four‐year RR 1.46, 95% CI 0.75–2.87), or cardiovascular disease mortality (one‐year RR 1.14, 95% CI 0.38–3.40, and four‐year RR 2.05, 95% CI 0.8–5.28) when compared to optimal medical management.22 This finding aligns with the limited benefits of PCI revascularization in stable coronary artery disease.23 It is important to note that this population, not eligible for surgery, has a high comorbidity burden that impacts mortality. Another consideration is that revascularization with hemodynamic support may be associated with a higher occurrence of in‐hospital major adverse cardiac and cerebrovascular events (MACCE), which is likely due to the selective use of mechanical support in patients with higher risk profiles.24
Data regarding LV systolic function is also inconsistent. The recent REVIVED‐BCIS2 trial failed to show benefits in all‐cause mortality (HR 0.99, 95% CI 0.78–1.27) or LV systolic function at 6 months (mean difference, −1.6 percentage points; 95% CI, −3.7 to 0.5) and at 12 months (mean difference, 0.9 percentage points; 95% CI, −1.7 to 3.4) compared with optimal guideline‐directed medical therapy, regardless of baseline viability characteristics.25 Notably, about 30% of modalities used to assess viability were other than CMR. In contrast, the RESTORE‐EF observational study reported significant improvement in LVEF at 90 days, from 35 ± 15% to 45 ± 14% (p < 0.0001).26 Additionally, this study revealed a substantial relative reduction of 76% in NYHA class III/IV heart failure symptoms and an impressive relative reduction of 97% in CCS angina class III/IV symptoms from baseline to the post‐PCI period. The improvement in LVEF was observed exclusively in patients with LVEF below 45%, whereas the improvement in heart failure and anginal symptoms was noted across the entire spectrum of LVEF. The disparity between these two trials is likely due to differences in the study populations. In the later trial, patients had higher rates of left main disease and more extensive coronary disease. Angina was also more frequent and severe. Additionally, in the REVIVED‐BCIS2 trial, two‐thirds of the patients had not been hospitalized in the previous 2 years, and there were no cases of non‐ST elevation myocardial infarction.
In conclusion, our case highlights the potential benefits of complex high‐risk PCI with mechanical support and the potential benefits of CTO PCI to improve LV function.
AUTHOR CONTRIBUTIONS
Stefan Milutinovic: Conceptualization; resources; writing – original draft. Kamaldeep Singh: Resources; supervision; writing – review and editing. Stevan Oluic: Conceptualization; resources; writing – original draft. Juan C. Lopez‐Mattei: Supervision; visualization; writing – review and editing. Ricardo O. Escárcega: Supervision; writing – review and editing.
FUNDING INFORMATION
None.
CONFLICT OF INTEREST STATEMENT
The authors report no relationships that could be construed as a conflict of interest.
CONSENT
Written informed consent was obtained from the patient to publish this report in accordance with the journal's patient consent policy.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Doshi D , Ben‐Yehuda O , Bonafede M , et al. Underutilization of coronary artery disease testing among patients hospitalized with new‐onset heart failure. J Am Coll Cardiol. 2016;68(5):450‐458. doi:10.1016/j.jacc.2016.05.060 27470451 PMC 9135048 · doi ↗ · pubmed ↗
- 2Lloyd‐Jones DM , Larson MG , Leip EP , et al. Lifetime risk for developing congestive heart failure: the Framingham Heart Study. Circulation. 2002;106:3068‐3072.12473553 10.1161/01.cir.0000039105.49749.6f · doi ↗ · pubmed ↗
- 3John JE , Claggett B , Skali H , et al. Coronary artery disease and heart failure with preserved ejection fraction: the ARIC study. J Am Heart Assoc. 2022;11(17):e 021660. doi:10.1161/JAHA.121.021660 36000416 PMC 9496411 · doi ↗ · pubmed ↗
- 4Maddox TM , Januzzi JL Jr , Allen LA , et al. 2021 update to the 2017 ACC expert consensus decision pathway for optimization of heart failure treatment: answers to 10 pivotal issues about heart failure with reduced ejection fraction: a report of the American College of Cardiology Solution set Oversight Committee. J Am Coll Cardiol. 2021;77(6):772‐810. doi:10.1016/j.jacc.2020.11.022 33446410 · doi ↗ · pubmed ↗
- 5Waldo SW , Secemsky EA , O'Brien C , et al. Surgical ineligibility and mortality among patients with unprotected left main or multivessel coronary artery disease undergoing percutaneous coronary intervention. Circulation. 2014;130(25):2295‐2301. doi:10.1161/CIRCULATIONAHA.114.011541 25391519 PMC 4276481 · doi ↗ · pubmed ↗
- 6Bell MR , Gersh BJ , Schaff HV , et al. Effect of completeness of revascularization on long‐term outcome of patients with three‐vessel disease undergoing coronary artery bypass surgery: a report from the Coronary Artery Surgery Study (CASS) Registry. Circulation. 1992;86:446‐457.1638714 10.1161/01.cir.86.2.446 · doi ↗ · pubmed ↗
- 7Mehta SR , Wood DA , Storey RF , et al. Complete revascularization with multivessel PCI for myocardial infarction. N Engl J Med. 2019;381(15):1411‐1421. doi:10.1056/NEJ Moa 1907775 31475795 · doi ↗ · pubmed ↗
- 8Farooq V , Serruys PW , Bourantas CV , et al. Quantification of incomplete revascularization and its association with five‐year mortality in the synergy between percutaneous coronary intervention with taxus and cardiac surgery (SYNTAX) trial validation of the residual SYNTAX score. Circulation. 2013;128(2):141‐151. doi:10.1161/CIRCULATIONAHA.113.001803 23766350 · doi ↗ · pubmed ↗