Long story short
Murad Almasri, Nirbhay Parashar, Jeffrey Orcutt

Abstract
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
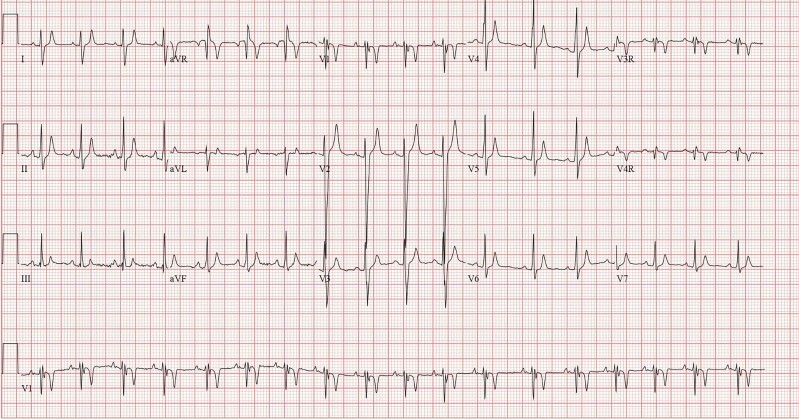 Figure 1
Figure 1Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsCardiac electrophysiology and arrhythmias · Ion channel regulation and function · Cardiac Arrhythmias and Treatments
Clinical vignette
A 13-year-old lady is followed periodically in the paediatric cardiology clinic. The patient suffered from a cardiac arrest when she was 2 years old and had a dual-chamber implantable cardioverter-defibrillator (ICD) implanted then. Her echocardiogram showed a normal heart structure and function. She had no further cardiac arrest episodes following her implantation and is seen regularly in the clinic with electrocardiograms (ECGs), Holters, and device checks. She is compliant with her Sotalol.
What is the diagnosis based on the clinical picture and ECG findings?
- Complete heart block
- Hypokalaemia
- Long QT syndrome
- Short QT syndrome
- Brugada syndrome
The correct answer is D.
Short QT syndrome (SQTS) is a rare, inherited channelopathy which is a known cause of sudden cardiac death due to increased risk of atrial and ventricular arrhythmias.^1^ Diagnosis is established based on ECG findings of an abnormally short QT interval (Figure 1). Short QT syndrome is usually defined as QTc < 330 ms or QT interval <360 ms and one or more of the following: history of cardiac arrest or syncope, family history of sudden cardiac death at age 40, or younger or a family history of SQTS.^2^ This patient has a QT interval of 240 ms and QTc 245 ms and has a history of cardiac arrest.
The patient's ECG showing normal sinus rhythm with a QT interval of 240 ms and a QTc of 245 ms.
- Which of the following is a known strong predictor for risk of recurrent ventricular arrhythmias over the course of time for a patient with this diagnosis?
- Positive genotype
- History of survived cardiac arrest at initial presentation
- History of anorexia
- Family history of arrhythmia
- Associated structural heart disease
The correct answer is B.
Short QT syndrome diagnosing criteria by Gollob et al.^2^ are composed of four components: ECG, clinical history, family history, and genotype. At least one point should be from ECG criteria. Four points or more indicate high probability, 3 points intermediate, and 2 points or fewer low probability of diagnosis of SQTS. Risk stratification remains a challenge. Gollob or modified Gollob score does not correlate with adverse cardiac events. However, history of survived cardiac arrest at initial presentation is a strong predictor of recurrent ventricular arrhythmias as two-thirds of them had a recurrence at follow-up. This strongly supports ICD implantation in cardiac arrest survivors.
- What is the most common complication for an ICD use in paediatric patients with this diagnosis?
- Non-capture
- Inappropriate ICD shocks
- AICD pocket infection
- Lead fracture
- Lead dislodgement
The correct answer is B.
Implantable cardioverter-defibrillator is recommended in symptomatic SQTS patients who are either survivors of sudden cardiac arrest and/or have documented spontaneous sustained ventricular tachyarrhythmias with or without syncope (Class I recommendation).^3^ Implantable cardioverter-defibrillator use for primary prevention should be limited, especially in young patients. There is an unusually high incidence of inappropriate ICD shocks in patients with SQTS.^4^ This may be due to oversensing of short-coupled and prominent T-waves, resulting in T-wave oversensing. There is also a high prevalence of ventricular lead fracture in paediatric patients, with most resulting in inappropriate ICD shocks.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Rudic B , Schimpf R, Borggrefe M. Short QT syndrome—review of diagnosis and treatment. Arrhythm Electrophysiol Rev 2014;3:76–79.26835070 10.15420/aer.2014.3.2.76PMC 4711567 · doi ↗ · pubmed ↗
- 2Gollob MH , Redpath CJ, Roberts JD. The short QT syndrome: proposed diagnostic criteria. J Am Coll Cardiol 2011;57:802–812.21310316 10.1016/j.jacc.2010.09.048 · doi ↗ · pubmed ↗
- 3Priori SG , Wilde AA, Horie M, Cho Y, Behr ER, Berul C, et al Executive summary: HRS/EHRA/APHRS expert consensus statement on the diagnosis and management of patients with inherited primary arrhythmia syndromes. Heart Rhythm 2013;10:e 85–e 108.23916535 10.1016/j.hrthm.2013.07.021 · doi ↗ · pubmed ↗
- 4Villafañe J , Atallah J, Gollob MH, Maury P, Wolpert C, Gebauer R, et al Long-term follow-up of a pediatric cohort with short QT syndrome. J Am Coll Cardiol 2013;61:1183–1191.23375927 10.1016/j.jacc.2012.12.025 · doi ↗ · pubmed ↗