A Survey of the Estimated Cost of Surgical Consumable Items Within Trauma and Orthopaedic Departments
Omkaar Divekar, Krushi Pandya, Anand B Divekar, Rahul Kanegaonkar

TL;DR
This study shows that Trauma and Orthopaedic department staff have limited knowledge about the actual costs of surgical consumables, with only a small percentage of cost estimates being accurate.
Contribution
The paper provides a survey-based assessment of cost-awareness among T&O staff, revealing a lack of knowledge about consumable item costs.
Findings
Only 7.1% of all item cost estimates were correct.
Kenalog 1 mL ampoule had the highest estimation accuracy (13%), while kirschner wires and 3.2 drill bit had the lowest (4% each).
Tourniquet cuffs were the most underestimated item, with a median estimate/actual cost ratio of 0.16.
Abstract
Introduction The impact of the current economic and environmental climate, both nationally and globally, is further straining the NHS. This has led to scrutiny of high-expenditure areas, including consumables. Clinician’s knowledge surrounding health economics is sparse, and we conducted this survey to assess cost-awareness within the Trauma and Orthopaedic (T&O) departmental staff. Methods A questionnaire was digitally distributed to T&O staff in the East Kent Hospitals Trust. This included demographic data and to make estimations of the cost of 10 specialty-specific items. The data were analysed to determine the average, median, and interquartile range (IQR) of the estimated prices and compared to the actual costs. Results Approximately 7.1% of all item estimates were deemed ‘correct’. No correlation was seen between years of staff experience and the accuracy of estimates.…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
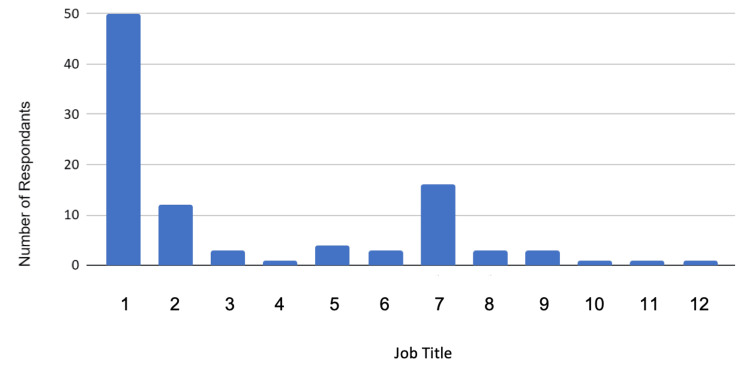 Figure 1
Figure 1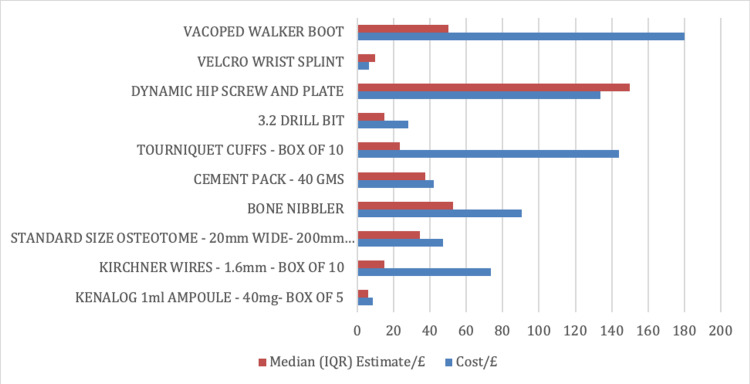 Figure 2
Figure 2| Item | Quantity | Actual Cost/£ |
| Kenalog 1 mL ampoule | 40 mg, box of 5 | 8.31 |
| Kirschner wires, 1.6 mm | Box of 10 | 73.68 |
| Standard size osteotome, 200 mm x 20 mm | One (1) | 47.25 |
| Bone nibbler | One (1) | 90.56 |
| Cement pack | 40 grams | 42.00 |
| Tourniquet cuffs | Box of 10 | 144.18 |
| 3.2 mm drill bit | One (1) | 28.00 |
| Dynamic hip screw and plate | One (1) | 44.00 + 90.00 |
| Velcro wrist splint | One (1) | 6.35 |
| VACOped walker boot | One (1) | 180.00 |
| Distribution of Practitioners | Number of Respondents (% of total practitioners) |
| Theatre Practitioner | 2 (12.5%) |
| Senior Orthopaedic Surgical Care Practitioner | 1 (6.25%) |
| Orthopaedic Practitioner | 2 (12.5%) |
| Scrub Practitioner | 1 (6.25%) |
| Operating Department Practitioner | 10 (62.5%) |
| Total Practitioners | 16 |
| Distribution of Coordinators | Number of Respondents (% of total coordinators) |
| Clinical Trauma Coordinator | 1 (33.3%) |
| Orthopaedic Theatre Lead/Theatre Coordinator | 1 (33.3%) |
| Theatre Emergency Coordinator | 1 (33.3%) |
| Total Coordinators | 3 |
| Item | Quantity | Cost/£ | Median (IQR) Estimate/£ | Median Estimate/Actual Cost | Percentage of Respondents Within 20% |
| Kenalog 1 mL ampoule | 40 mg – box of 5 | 8.31 | 6.00 (12) | 0.72 | 13 |
| Kirschner wires - 1.6 mm | Box of 10 | 73.68 | 15.00 (42.25) | 0.20 | 4 |
| Standard size osteotome – 200 mm x 20 mm | One (1) | 47.25 | 34.50 (62.00) | 0.73 | 9 |
| Bone nibbler | One (1) | 90.56 | 52.50 (102.50) | 0.58 | 6 |
| Cement pack | 40 grams | 42.00 | 37.50 (72.50) | 0.90 | 11 |
| Tourniquet cuffs | Box of 10 | 144.18 | 23.50 (50.00) | 0.16 | 5 |
| 3.2 mm drill bit | One (1) | 28.00 | 15.00 (40.00) | 0.54 | 4 |
| Dynamic hip screw and plate | One (1) | 44.00 + 90.00 | 150.00 (250.00) | 1.12 | 7 |
| Velcro wrist splint | One (1) | 6.35 | 10.00 (20.00) | 1.57 | 6 |
| VACOped walker boot | One (1) | 180.00 | 50.00 (75.00) | 0.28 | 6 |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsHealthcare cost, quality, practices · Health Systems, Economic Evaluations, Quality of Life · Healthcare Policy and Management
Introduction
The impact of the current economic and environmental climate, both nationally and globally, is further straining an issue-saturated NHS [1]. With these rising concerns, interest has been generated surrounding high-expenditure specialities, namely surgical specialities and in particular Trauma and Orthopaedic (T&O) departments [2].
Operating theatres are acknowledged to be one of the largest expenditures within a hospital, with operating costs estimated to be approximately £1,200/hour [3]. Specifically, the use of sterilised surgical equipment has been long debated, with infection control being favoured over the fiscal and environmental impact of the implementation of disposable tools [4]. The risks to patients' health because of contamination have led to medical practice using single-use disposable equipment, increasing wastage. Studies have confirmed that the vast differences in equipment used from trust to trust, if more well-informed, may lead to a reduction in waste and expenditure [5].
This disparity has spurred a drive for medical schools across the country to embed sustainable healthcare teaching into their curricula, with a drive for high-quality care to prevent costly intervention in the future [6]. Whilst decision-making regarding waste reduction policies is centralised, all healthcare professionals have an ethical obligation to reduce their carbon footprint, whilst primarily providing an efficient and effective service [7].
This paper aims to further elucidate primarily the awareness of the cost of consumables within the T&O department and further ascertain if there are links between experience, geographical distribution, and job role. Furthermore, we have aimed to qualitatively identify whether T&O departments believe that the price of a consumable item should influence its use.
This article was previously presented as a poster at the Association of Surgeons in Training (ASIT) held in Bournemouth in March 2024.
Materials and methods
This paper was approved by the Research and Innovation Department of East Kent Hospitals and contributed to a broader regional survey of NHS clinicians, varying in specialty. A digital questionnaire was generated using Microsoft Forms (Microsoft® Corp., Redmond, WA), including demographic data (e.g., age, gender, job title, years of experience). In the second section, participants were asked to estimate the cost of 10 general medical equipment items, followed by 10 T&O-specific consumables, in pounds and pence (Table 1). All items included in the survey had illustrations attached.
This online survey was distributed within the East Kent Hospitals Trust. Responses were included as valid entries if they fulfilled the inclusion criteria, which were as follows: response within the stipulated six-week time frame (October 14-November 30, 2022) and the participant working within a T&O department. To have control for the quantitative analysis, the actual costs of the items were sourced from the online East Kent Hospital Procurement Department [8]. Data analysis focused on comparisons between the actual and estimated price (average, median, and interquartile range (IQR)). An answer was deemed ‘correct’ if it was within 20% of the actual price. This was mimicked from previous studies to give a standardised results section [2].
Results
One hundred and five responses were recorded, with 98 being analysed after applying the inclusion/exclusion criteria. Demographic data are considered first. The distribution of job roles within the respondents is shown in Figure 1. Figure 2 gives a visual representation of the accuracy of estimated median costs compared to actual costs.
Distribution of survey respondents categorised by job titleJob Titles: (1) Consultants, (2) Nurses, (3) Registrars, (4) Specialty Grade Doctor, (5) Associate Specialist, (6) Advanced Practice Physiotherapist, (7) Practitioners, (8) Coordinators, (9) Theatre Support Workers, (10) Day Surgery Manager, (11) Medical Secretary, (12) Theatre Audit Clerk
Accuracy of estimated median item costs compared to actual item costs
Table 2 shows job titles that were grouped together in Figure 1.
The sex distribution of respondents was reported as 51 (52%) ‘Male’, 46 (47%) ‘Female’, and one (1%) ‘Preferring not to say’. Table 3 illustrates the following results. Approximately 7.1% of all item estimates were deemed ‘correct’. No correlation was seen between years of staff experience and the accuracy of estimates. Kenalog 1 mL ampoule (Kenalog, Bristol-Myers Squibb, NJ) had the highest accuracy of estimation across all responses with 13 (13%), respondents whilst both ‘kirschner wires’ and ‘3.2 drill bit’ had the lowest accuracy with only four (4% each) respondents correctly estimating the cost. The median estimated cost was closest to the actual cost for the ‘cement pack’ (median estimate/actual cost = 0.9). The median estimated cost was furthest from the actual cost for ‘tourniquet cuffs’ (median estimate/actual cost = 0.16). ‘Velcro wrist splint’ was the item that was the most overestimated (median estimate/actual cost = 1.57), with only two of the 10 items meaning overestimated (‘velcro wrist splint’ and ‘dynamic hip screw and plate’). The most underestimated item was ‘tourniquet cuffs’ (median estimate/actual cost = 0.16).
The question ‘Should the cost of an item influence its use?’ showed 60 (61.2%) participants answering with ‘Yes’ and 38 (38.8%) with ‘No’.
Discussion
With the expenditure of the NHS overshadowing the growth of the country’s economy, the ever-surmounting financial pressure is significantly rising because of the cost-of-living crisis, following the pandemic. The NHS ‘Long Term Plan’ stipulates that the ‘key’ to ‘sustainable development and reducing the use of natural resources in line with government commitments’ lies in the ‘ reductions [of] single-use plastics, throughout the NHS supply chain’ [9]. With the ongoing drive to shift towards sustainable healthcare, the focus must be directed towards the utilisation of single-use disposable items. Hence, we conducted this survey to ascertain the cost-awareness of T&O staff, as this department is often under scrutiny for the overuse of consumables. Overall, this study shows a paucity of data pertaining to the cost-awareness of T&O specialists in the United Kingdom.
Only 7.1% of all estimates for all items were deemed ‘correct’, with the price of two out of 10 items in the questionnaire being overestimated. This indicates an underestimation of the cost of consumables and could be extrapolated to other equipment and services as well. If T&O staff believe that their equipment is cheaper than it is, then this suggests that there is an ability for intervention to have better outcomes both financially and economically. For example, if a department were to relate the cost or environmental impact to each misuse of a consumable, it may result in staff reconsidering their options when using consumables and consequently reduce overall waste and, therefore, money. This would be an example of a micro-allocation (varies from individual to individual). Considering the significance of macro-allocation (wider policies focussing on a wider scope), studies such as this one could highlight the disparities nationally between different specialities and create more specific plans for containing costs in relation to consumables [10].
One of the interventions employed currently in other countries in a bid to reduce wastage is price transparency [11]. Staff in these surgical specialities agreed that knowing the cost of items would cause them to reconsider their usage and, more importantly, wastage [12]. This is aligned with our study, where 60 (61.2%) participants replied with ‘Yes’ to the question ‘Should the cost of an item influence its use?’, suggesting that there is a need for this information to be distributed. However, certain methods of price transparency that may be fruitful in other countries may not work in the United Kingdom because of the public funding of the NHS. With the NHS treating all patients freely and equally at the point of care, this may have led staff to a feeling of non-responsibility pertaining to the cost of treatment, as it is not considered at the time of treatment and therefore not tangible. By reminding clinicians of their ethical duty not only through patient care but also through the effective use of taxpayer money and duty to the environment, it may be possible to decrease the impact of consumables.
To draw conclusions about the factor of experience in relation to cost awareness, the question ‘What is your job title?’ was asked and the time period the participants had been in the role; however, this did not account for previous experience before the current role respondents were in. This is a limitation of the study as the full extent of the subjects was not ascertained, and it is difficult to quantify as non-medical experience may also increase cost awareness. This is something that would be modified in future studies to allow full saturation of this factor in determining if experience had an effect on cost awareness.
The relevance of surveying all T&O staff must also be questioned. Whilst all medical professionals must have a basic duty towards reducing economic and environmental waste, doctors and nurses are often the ones who decide on which consumables to use. If health economics is taught throughout all healthcare curricula, but not applied in practice, it may lead to students adversely, giving health economics less importance because of being classed as ‘low yield’. This is a small tweak that can be made for future studies if it is deemed important to focus on a specific subgroup of staff.
The sample size was relatively small as it focused purely on the T&O department in one trust. This may not be a true representation of the national population we are trying to draw conclusions from and would need multiple trusts across the country to partake in this. It is difficult to link the success of education in varying curricula to job titles, as professionals come from a multitude of institutions, hospitals, and previous jobs.
Conclusions
The awareness of the costing of equipment and price transparency to hospital staff in an attempt to combat the ever-rising financial strain have been key interventions highlighted by NHS England. Coupled with the global progression to sustainable healthcare (benefits patients and the environment, focussing on early intervention) being the golden standard, the usage and impact of disposable products must be scrutinised.
We hope this will provide a baseline for further studies in different geographical areas and initiate a push for better practice at national and trust levels.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Helen Salisbury: the NHS is not unsustainable BMJ Salisbury H 99138120233713060410.1136/bmj.p 991 · doi ↗ · pubmed ↗
- 2Awareness of surgical expenditure amongst UK trainees and consultants: a questionnaire study Int J Surg Povey M Francis N Healy R Blacker S Vimalachandran D Sutton PA 8126720193102251810.1016/j.ijsu.2019.04.008 · doi ↗ · pubmed ↗
- 3Improving theatre turnaround time BMJ Qual Improv Rep Fletcher D Edwards D Tolchard S Baker R Berstock J 6201710.1136/bmjquality.u 219831.w 8131 PMC 530668428243441 · doi ↗ · pubmed ↗
- 4Reducing the environmental impact of sterilization packaging for surgical instruments in the operating room: a comparative life cycle assessment of disposable versus reusable systems Sustainability Friedericy HJ van Egmond CW Vogtländer JG van der Eijk AC Jansen FW 430142022
- 5Protecting resources, promoting value: a doctor’s guide to cutting waste in clinical care 7 2024 2014 https://networks.sustainablehealthcare.org.uk/sites/default/files/resources/Promoting%20value%20FINAL.pdf
- 6Education for sustainable healthcare 7 2024 EDUCATION FOR SUSTAINABLEHEALTHCARE 2022 https://www.medschools.ac.uk/media/2949/education-for-sustainable-healthcare_a-curriculum-for-the-uk_20220506.pdf
- 7Greener NHS campaign to tackle climate “health emergency” 7 2024 2020 https://www.england.nhs.uk/2020/01/greener-nhs-campaign-to-tackle-climate-health-emergency/
- 8NHS supply chain 7 2024 2017 https://www.supplychain.nhs.uk/