A Case of Amiodarone-Induced Thyrotoxicosis Presenting With Methimazole-Induced Agranulocytosis
Neha Meda, Suhail Saad-Omer, Moises Matos, Mustafa Kinaan

TL;DR
A patient with amiodarone-induced thyrotoxicosis experienced complications from methimazole and was successfully treated with surgery and hormone replacement.
Contribution
This case highlights the challenges in managing AIT and the effectiveness of surgical intervention when medical therapy fails.
Findings
Methimazole treatment was stopped due to agranulocytosis.
Total thyroidectomy resolved persistent thyrotoxicosis.
The patient is now euthyroid with levothyroxine therapy.
Abstract
Amiodarone is a class III anti-arrhythmic drug found to be effective in treating multiple life-threatening arrhythmias, including paroxysmal atrial fibrillation. Despite its effectiveness, amiodarone has been found to result in thyroid dysfunction. Amiodarone-induced thyrotoxicosis (AIT) is classified as type 1, which often develops in those with autoimmune hyperthyroid conditions, or type 2, which occurs because of destructive thyroiditis in an apparently normal thyroid. Differentiating between both types often poses a clinical and therapeutic dilemma, as AIT 1 is treated with thionamides, whereas AIT 2 requires steroids for treatment. We present a case of a patient with AIT who was treated empirically for both subtypes with methimazole and prednisone without clinical improvement. Methimazole was later stopped due to concern for agranulocytosis, and the patient was then treated with…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
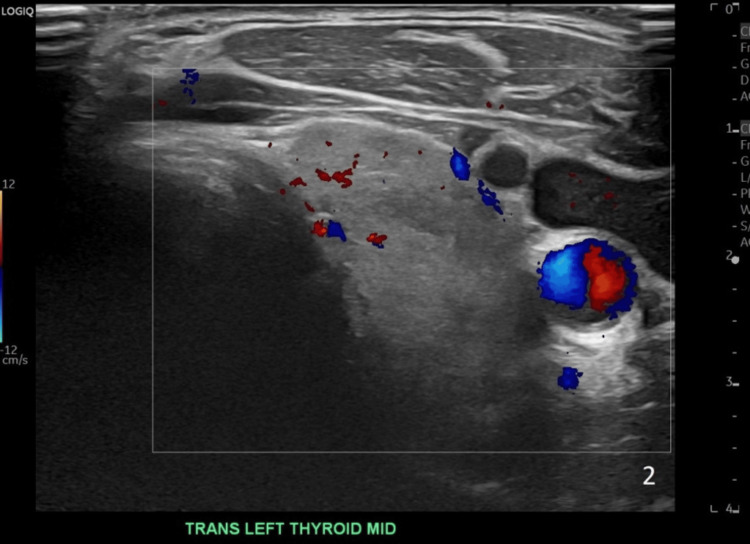 Figure 1
Figure 1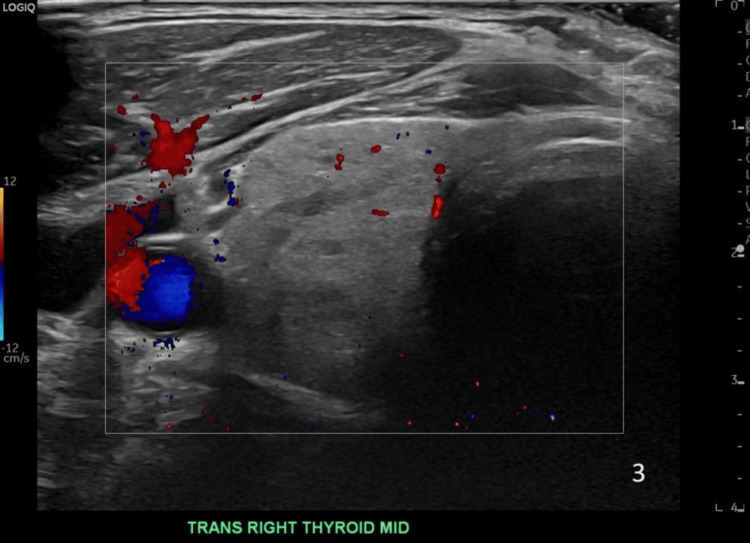 Figure 2
Figure 2| Test | Lab value | Normal range |
| TSH | <0.01 uIU/ml | 0.36-3.74 uIU/ml |
| Free T4 | 3.32 ng/dL | 0.76-1.75 ng/dL |
| Total T3 | 237 ng/dL | 86-192 ng/dL |
| Thyrotropin receptor-blocking antibodies | <1.10 IU/mL | 0.0-1.75 IU/mL |
| Thyroglobulin antibodies | <20 IU/mL | 0.0-40.0 IU/mL |
| Thyroid peroxidase antibodies | <10.0 IU/mL | 0.0-35I U/mL |
| WBC count | 8200 cells/mL | 4000-10000 cells/µL |
| ANC | 4887 cells/mL | 1780-5380 cells/mL |
| Test | Day 1 of admission | Day 2 of admission |
| White blood cell count | 4000 cells/mL | 2600 cells/mL |
| Absolute neutrophil count | 520c ells/mL | 62 cells/mL |
| Thyroid-stimulating hormone | <0.01 uIU/mL | - |
| Free T4 | 4.01 ng/dL | - |
| Total T3 | 146 ng/dL | - |
| IL-6 | 6.6 pg/mL (0.0-13.0) | - |
| Type 1 | Type 2 | |
| Mechanism | Excessive thyroid hormone production due to iodine overload | Destructive thyroiditis leads to release of preformed thyroid hormone into circulation |
| Pre-existing thyroid disease | Yes, patients may have latent autoimmune thyroid disease | No |
| Prevalence | Most common type in iodine-deficient regions | Most common type in the United States |
| Imaging | Normal or increased vascularity on USG | Decreased vascularity on USG |
| Labs | May have positive TSI, TRAB, no IL-6 elevation, normal/high thyroglobulin | No detectable thyroid antibodies, may have IL-6 elevation, low thyroglobulin |
| Treatment | Antithyroid medications | Steroids |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsThyroid Disorders and Treatments · Ion channel regulation and function · Blood disorders and treatments
Introduction
Amiodarone is a class III anti-arrhythmic drug found to be effective in treating multiple life-threatening arrhythmias including paroxysmal atrial fibrillation. Despite its effectiveness, amiodarone has been found to result in thyroid dysfunction. Amiodarone-induced thyrotoxicosis (AIT) is classified as type 1 which often develops in those with autoimmune hyperthyroid condition or type 2 which occurs because of destructive thyroiditis in an apparently normal thyroid. Differentiating between both types often poses a clinical and therapeutic dilemma as AIT 1 is treated with thionamides, whereas AIT 2 requires steroids for treatment. We present a case of a patient with AIT who was treated empirically for both subtypes with methimazole and prednisone without clinical improvement. Methimazole was later stopped given concern for agranulocytosis, and the patient was then treated with cholestyramine, metoprolol, and prednisone. Given persistent thyrotoxicosis, the decision was made to proceed with surgical intervention. The patient underwent a successful total thyroidectomy without complications. The patient‘s condition clinically improved post-surgery and was discharged home on post-operative day 2 in stable condition. Prednisone was tapered over two weeks, and he was started on a weight-based dose of levothyroxine. He continues to follow up in our clinic for postoperative hypothyroidism and is clinically and biochemically euthyroid.
This case was presented at the American Association of Clinical Endocrinology (AACE) annual meeting in 2023 and published as an abstract in Endocrine Practice in May 2023 [1].
Case presentation
A 67-year-old man presented to the hospital due to a two-week history of palpitations, elevated heart rate, and associated chest tightness. He reported mild tremors, diarrhea, and unintentional weight loss. His medical history was remarkable for hypertension, atrial fibrillation, and a prior cerebral vascular accident at the age of 40. The patient denied any personal or family history of thyroid disease. He was diagnosed with atrial fibrillation three years ago and treated with amiodarone for about two years. His initial examination was notable for an irregularly irregular heart rhythm, clear lungs to auscultation bilaterally, and a normal neck without jugular venous distension or goiter. His initial EKG on admission showed atrial fibrillation with rapid ventricular response and a heart rate of 120 bpm. Initial labs were notable for hyperthyroidism (Table 1).
Thyroid ultrasound showed a slightly enlarged and heterogeneous thyroid without discrete nodules and normal vascularity (Figures 1-2). A preliminary diagnosis of AIT was made. He was treated empirically for both AIT 1 and AIT 2 with methimazole 40 mg and prednisone 40 mg daily.
Image of the left lobe thyroid ultrasound
Image of the right lobe thyroid ultrasound
He presented to the hospital approximately one month later with similar complaints. He was again noted to be in atrial fibrillation with a rapid ventricular response. His Burch-Wartofsky score on presentation was 30, which is suggestive of an impending thyroid storm. Initial labs during his second admission were notable for agranulocytosis and persistent hyperthyroidism, despite methimazole and prednisone therapy for over a month (Table 2).
Methimazole was discontinued upon admission, and the patient was treated with cholestyramine, metoprolol, and prednisone. Given the persistent hyperthyroidism and the development of agranulocytosis, thyroidectomy was necessary. His agranulocytosis improved with the discontinuation of methimazole and resolved completely a day after administration of filgrastim 300 mcg. He was treated with potassium iodide (SSKI) in preparation for thyroidectomy to reduce vascularity and decrease intra-operative blood loss. Given his prolonged exposure to high-dose steroids for treatment of AIT, he was treated with hydrocortisone during the perioperative period. Early in the morning, cortisol was checked and found to be 7.35 mcg/dL. He was considered at risk for adrenal insufficiency from hypothalamic-pituitary axis suppression due to prolonged exposure to steroids. He underwent a successful total thyroidectomy without complications. He did well following his surgery and was discharged home in stable condition on postoperative day two. His prednisone was tapered off over two weeks, and he was started on a weight-based dose of levothyroxine. He continues to follow up in our endocrine clinic and is clinically and biochemically euthyroid.
Discussion
Amiodarone is a class III anti-arrhythmic drug that has been found to be effective in the treatment of multiple life-threatening arrhythmias, including paroxysmal atrial fibrillation, as well as in recurrent severe ventricular arrhythmias [2]. Despite its effectiveness, it has been found to frequently induce thyroid dysfunction in as many as 36% of patients who take this medication chronically [3]. This side effect is thought to be due to either excessive iodine overload related to its biochemical structure or to its direct cytotoxicity on thyrocytes [4]. AIT was found to develop in 3% of patients in North America, while those living in iodine-depleted areas were found to have a higher incidence of 10% [5]. Bogazzi et al. helped to classify AIT into two major categories: type 1 and type 2 (Table 3) [6,7].
AIT 1 typically occurs in patients with an underlying thyroid pathology such as Graves’ disease or multinodular goiter. In these patients, iodine overload secondary to amiodarone leads to follicular hyperreactivity. However, in AIT 2, thyrotoxicosis results from the cytotoxic effect of amiodarone and results in destructive thyroiditis, causing excess release of T3 and T4 into the circulation [6]. The effect of amiodarone may vary, taking several weeks to several years to manifest in some patients [3]. The majority of cases in North America are AIT 2, whereas AIT 1 predominates in iodine-deficient areas of the world [5]. The differentiation of these two types of AIT often poses a unique challenge for clinicians, as some patients may have a mixture of both mechanisms. Nevertheless, determining which type of AIT a patient has is imperative in deciding subsequent management and treatment. Patients with AIT may have typical hyperthyroid symptoms, including palpitations, tremors, and sweating, or be completely asymptomatic, likely due to the beta-adrenergic blockade of amiodarone [8]. This is why a thoroughly taken history and conducted physical examination are imperative to help determine whether the patient has a pre-existing thyroid condition. A physical exam may reveal a goiter or exophthalmos. Ultrasounds of the thyroid may show an enlarged gland or nodular goiter. Thyroid peroxidase may also be present. These features may sway the differential in favor of AIT 1. Inflammatory markers such as IL-6 may be elevated in AIT 2, indicating ongoing thyroiditis; however, some patients with AIT 2 have been found to have low IL-6 levels, likely due to the assay being used, limiting its overall usefulness [9]. One tool that is gaining favor to help in the rapid and early diagnosis of AIT is color flow Doppler sonography (CFDS). This test helps shed light on the morphology of the thyroid by determining the amount of blood flow within the organ. Several recent studies have shown that the absence of hyperflow on CFDS is suggestive of AIT 2, while an increase in vascularity supports a diagnosis of AIT 1 [10].
The treatment of AIT is often very challenging for the clinician, especially in cases where the type is uncertain. The first issue that must be addressed is the continuation or discontinuation of amiodarone. Patients with severe, resistant tachyarrhythmias would require amiodarone to be continued regardless of the risk of AIT aggravation or reoccurrence [6]. Some experts believe that due to amiodarone’s prolonged half-life of six months secondary to its lipo-solubility, continuing or discontinuing the drug would not influence AIT management [6]. Nevertheless, multiple studies have shown amiodarone continuation increased the rate of reoccurrence in patients with AIT 2 and also delayed the response of treatment to glucocorticoids and thionamides [11]. ATA recommends taking into consideration the cardiologist’s decision on whether an alternative to amiodarone is available [12].
AIT 1 is typically treated with antithyroid thionamides at high doses in order to overcome high iodine concentrations. Thionamides are typically continued for about three to six months until euthyroidism is restored [13]. Potassium perchlorate may also be started in the first few weeks of treatment to decrease thyroid uptake of iodine and make the thyroid more sensitive to the antithyroid medication (ATD); however, due to its toxicity and risk of aplastic anemia, its use is limited to short periods of time [14]. AIT 2 is usually self-limited and, in mild cases, can resolve spontaneously in about 20% of cases. However, due to the increased mortality associated with this condition in cardiac patients, treatment is typically started [15].
AIT 2 is treated with glucocorticoids for anti-inflammatory effects. Prednisone is started at 40 mg daily and tapered over two to three months [15]. In cases where AIT is mixed or unidentified, treatment should typically begin with ATD and oral corticosteroids [7]. A large cohort study revealed that the prevalence and incidence of ATD-AGRAN were higher in AIT patients compared with non-AIT patients [16]. Total thyroidectomy is usually considered under several circumstances, the most common being insufficient response to drug treatment with ATD and corticosteroids, with other indications being rapid deterioration of cardiac function as well as advanced heart disease and malignant arrhythmias [17]. In a recent observational study with 207 AIT patients, those who underwent thyroidectomy showed lower mortality and significant improvement in LVEF than those who were only treated medically, especially in patients with LVEF <40% [18]. Another smaller retrospective cohort study at Mayo Clinic revealed similar findings supporting the fact that thyroidectomy does help to rapidly resolve thyrotoxicosis and improve cardiac function, but that complications of the procedure in AIT were higher than those with other thyrotoxic etiologies [19]. Finally, plasmapheresis remains another interesting treatment modality that has shown promise, but so far evidence has only been limited to case reports [20].
Conclusions
This is a unique case of AIT that could not be classified into either type 1 or type 2 and was treated empirically for both types. These uncategorized cases of AIT are difficult to treat with medical therapy and likely require surgical management, as seen in this case. Further research is warranted into treatment and non-surgical options for treating AIT, along with guidelines on the treatment of uncategorized or mixed AIT.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Between a rock and a hard place: a case of amiodarone induced thyrotoxicosis presenting with methimazole induced agranulocytosis Endocr Pract Matos M Saad-Omer S Kinaan Kinaan 9192292023
- 2Practical guidelines for clinicians who treat patients with amiodarone. Practice Guidelines Subcommittee, North American Society of Pacing and Electrophysiology Arch Intern Med Goldschlager N Epstein AE Naccarelli G Olshansky B Singh B 1741174816020001087196610.1001/archinte.160.12.1741 · doi ↗ · pubmed ↗
- 3Incidence, predictability, and pathogenesis of amiodarone-induced thyrotoxicosis and hypothyroidism Am J Med Trip MD Wiersinga W Plomp TA 507511911991195141310.1016/0002-9343(91)90187-3 · doi ↗ · pubmed ↗
- 4The effects of amiodarone on serum thyroid hormones and hepatic thyroxine 5'-monodeiodination in rats Endocrinology Sogol PB Hershman JM Reed AW Dillmann WH 146414691131983661758110.1210/endo-113-4-1464 · doi ↗ · pubmed ↗
- 5Environmental iodine intake and thyroid dysfunction during chronic amiodarone therapy Ann Intern Med Martino E Safran M Aghini-Lombardi F 28341011984642829110.7326/0003-4819-101-1-28 · doi ↗ · pubmed ↗
- 6Approach to the patient with amiodarone-induced thyrotoxicosis J Clin Endocrinol Metab Bogazzi F Bartalena L Martino E 252925359520102052590410.1210/jc.2010-0180 · doi ↗ · pubmed ↗
- 72018 European Thyroid Association (ETA) guidelines for the management of amiodarone-associated thyroid dysfunction Eur Thyroid J Bartalena L Bogazzi F Chiovato L Hubalewska-Dydejczyk A Links TP Vanderpump M 5566720182959405610.1159/000486957 PMC 5869486 · doi ↗ · pubmed ↗
- 8Amiodarone-induced thyroid dysfunction S Afr Med J Ross IL Marshall D Okreglicki A Isaacs S Levitt NS 180183952005 http://www.samj.org.za/index.php/samj/article/view/158515832669 · pubmed ↗