A Case Report on the Utilization of a Hemostasis Analyzer System in the Management of a Patient With Essential Thrombocythemia
Tomohiro Nakajima, Kei Mukawa, Yutaka Iba, Yu Iwashiro, Nobuyoshi Kawaharada

TL;DR
This case report describes the use of a hemostasis analyzer system to manage a patient with essential thrombocythemia during heart surgery.
Contribution
Demonstrates the practical application of hemostasis analyzers in monitoring coagulation in a complex ET patient undergoing cardiac procedures.
Findings
The patient's coagulation profile showed hypercoagulability during surgery.
Use of the hemostasis analyzer enabled tailored transfusion and coagulation management.
The patient had no bleeding or thrombotic complications post-surgery.
Abstract
Essential thrombocythemia (ET) is a myeloproliferative neoplasm characterized by persistent elevation of platelet count due to abnormal proliferation of megakaryocytes. While some cases may be asymptomatic, the condition is associated with an increased risk of complications such as thrombosis and bleeding tendencies, necessitating appropriate management tailored to individual cases. Hemostasis analyzer systems are automated analytical devices designed for comprehensive evaluation of blood coagulation function. These systems enable rapid and accurate measurement of multiple parameters, including coagulation time, platelet function, and fibrin formation, thus facilitating a holistic assessment of hemostatic function. A 76-year-old male patient presented to our hospital. At the age of 65, he received treatment for promyelocytic leukemia and achieved remission. At 75 years, he developed…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
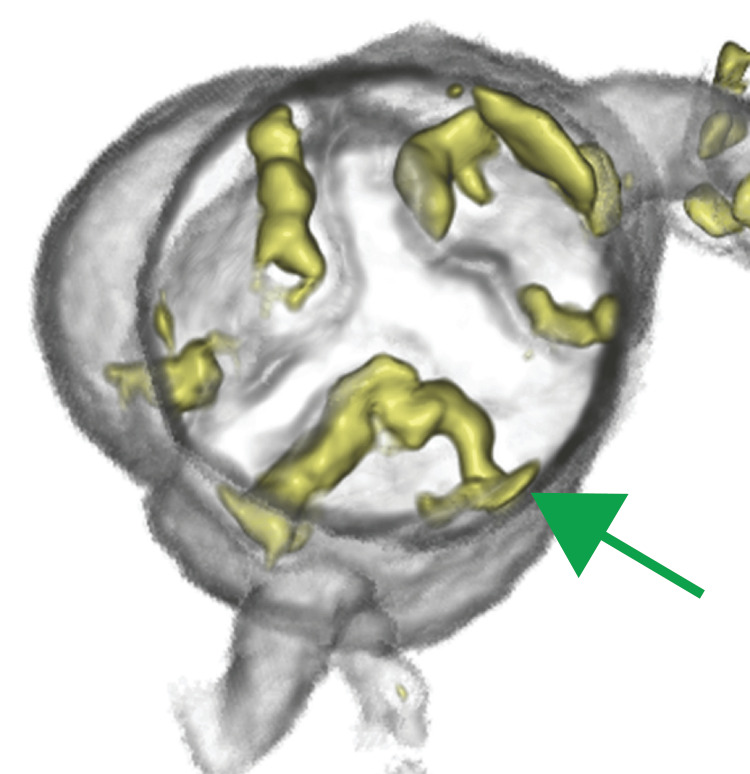 Figure 1
Figure 1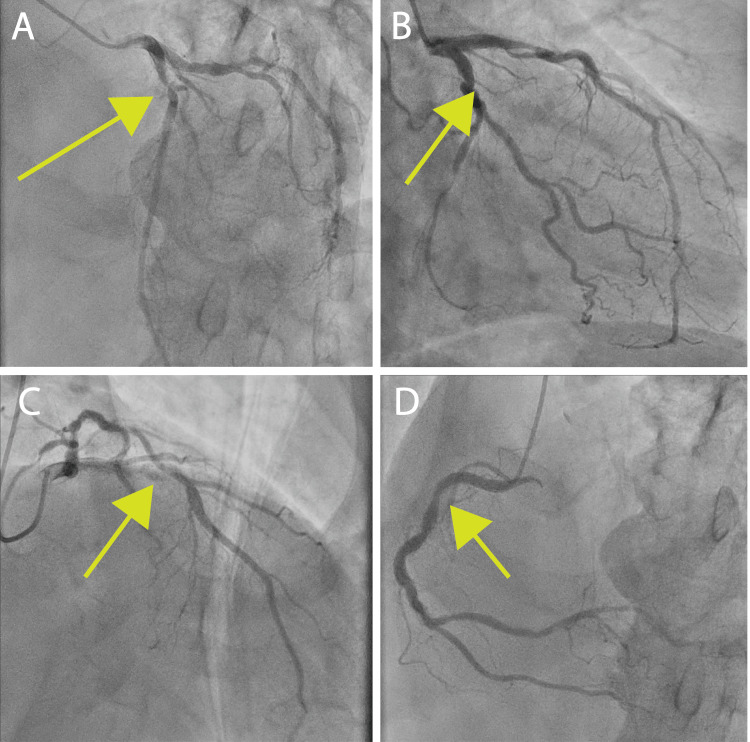 Figure 2
Figure 2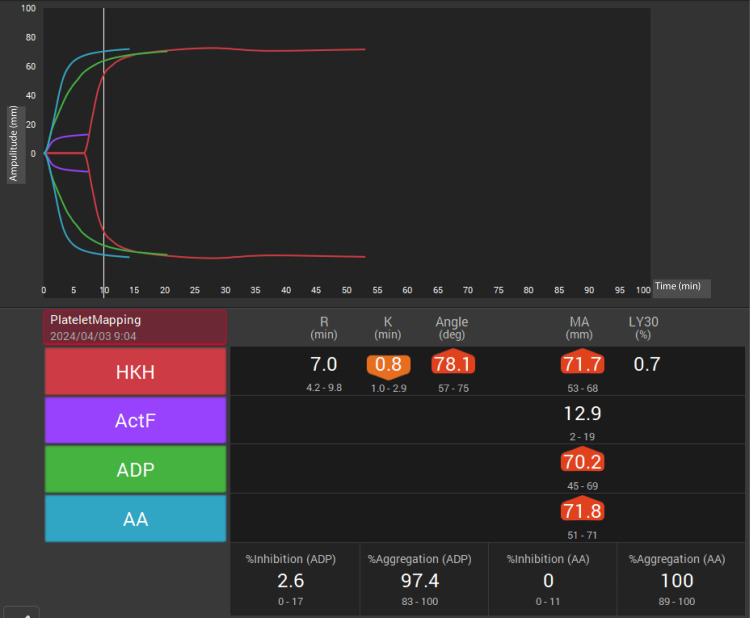 Figure 3
Figure 3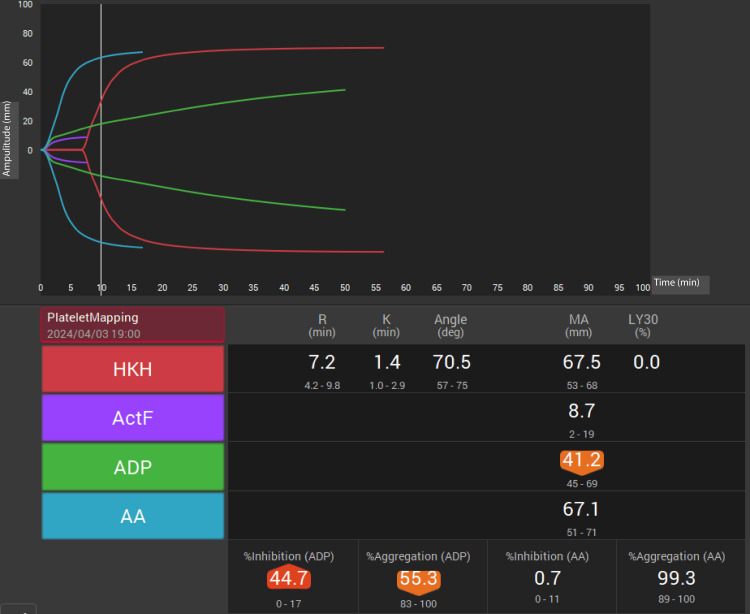 Figure 4
Figure 4Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsMyeloproliferative Neoplasms: Diagnosis and Treatment · Platelet Disorders and Treatments · Chronic Myeloid Leukemia Treatments
Introduction
Essential thrombocythemia (ET) is a subtype of myeloproliferative neoplasm (MPN), a hematopoietic tumor characterized by excessive platelet production that leads to thrombotic and hemorrhagic complications [1]. This disease has a complex pathophysiology with contradictory tendencies, including a propensity for thrombosis and bleeding diathesis, both of which stem from persistent peripheral blood thrombocytosis and platelet dysfunction. The prognosis is largely determined by these secondary complications. Reports of artificial valve replacement and coronary artery bypass grafting in patients with ET are extremely rare, with concerns regarding intraoperative bleeding tendencies and postoperative thrombosis due to the nature of this disease [2]. Herein, we report a case of aortic valve and coronary artery stenosis complicated by ET, which was successfully treated with bioprosthetic aortic valve replacement and coronary artery bypass grafting [3].
Case presentation
A 76-year-old man with a history of promyelocytic leukemia, who was treated and achieved remission at the age of 65 years, was under outpatient follow-up. At the age of 75 years, blood tests revealed leukocytosis, thrombocytosis, and anemia. Considering the possibility of leukemia relapse or myeloproliferative disorder, comprehensive evaluations including bone marrow biopsy and genetic testing were performed. Bone marrow findings were normal, but genetic testing revealed a JAK2 mutation, leading to the diagnosis of ET. Given the high thrombotic risk associated with this subtype, the patient was administered 100 mg aspirin daily.
At the age of 76 years, he developed exertional dyspnea. Blood tests showed leukocytosis (16,500/μL), mild anemia (hemoglobin 9.3 g/dL), and thrombocytosis (933 × 10³/μL). Echocardiography revealed severe aortic valve stenosis (0.78 cm²; mean PG, 40.8 mmHg; and aortic valve orifice area 0.83 cm²) (Figure 1).
Preoperative images of 3D enhanced computed tomographyThe aortic valve was observed from the cephalic side. This figure demonstrates the preoperative state of the aortic valve with tricuspid morphology and severity (green arrow).
Coronary angiography revealed 90% stenosis of the left anterior descending artery (LAD), 90% stenosis of the left circumflex artery (LCx), and 50% stenosis of the diagonal branches (Figures 2A-2C). Surgical intervention was deemed necessary, and bioprosthetic aortic valve replacement with coronary artery bypass grafting (left internal thoracic artery (LITA)-LAD; SVG-diagonal branch-posterolateral branch) was planned. Following the hospital safety protocol, aspirin was discontinued one week preoperatively and heparin bridging was initiated. In consultation with anesthesiologists, thromboelastography 6s (TEG6s, Haemonetics, Braintree, MA, USA) was employed intraoperatively to monitor coagulation status.
Preoperative coronary angiography(A) Left anterior descending artery (LAD) with 90% stenosis (green arrow). (B) Left circumflex artery (LCx) with 90% stenosis (green arrow). (C) Diagonal branch with 50% stenosis (green arrow). (D) Right coronary artery branch with 25% stenosis (green arrow).
Preoperative TEG6s measurements (MAHKH and early parameters: R, K, and angle) were obtained under general anesthesia (Figure 3). Both HKH-MA and ACT-F were above the reference range, indicating adequate overall clot strength. Following median sternotomy, LITA and left great saphenous vein were harvested. Cardiopulmonary bypass (CPB) was performed with an ascending aortic inflow and bicaval venous drainage. After aortic cross-clamping and antegrade cardioplegia, cardiac arrest was maintained with retrograde cardioplegia every 25 min. The posterior lateral branches of the left circumflex coronary artery and diagonal branch were anastomosed with a saphenous vein graft, followed by LITA-LAD anastomosis. The tricuspid aortic valve was excised, the annular calcification was debrided, and a 23 mm Inspiris bioprosthesis was implanted. After aortic closure and proximal SVG anastomosis, the aortic cross-clamp was released.
Preoperative thromboelastography (TEG6s) with HKH assayPreoperative coagulation profile using TEG6s with HKH assay This assay provides a comprehensive assessment of clot formation, strength, and stability. The overall clot strength (HKH-MA) is 71.7 mm (reference range: 52–70 mm) and fibrinogen contribution to clot strength (ActF-MA) is 12.9 mm (reference range: 7–22 mm).
During CPB weaning, repeated TEG6s measurements showed high HKH-MA and ACT-F, but low ADP-MA (42.2 mm; reference range: 45-69 mm), suggesting platelet dysfunction. Post-CPB, 10 units of FFP and 20 units of platelets were transfused. Hemostasis was achieved without difficulty. Preclosure TEG6s again showed low ADP-MA (41.2 mm), prompting an additional 20 units of platelets (Figure 4). Aortic cross-clamp, CPB, and total operative times were 224, 307, and 524 min, respectively.
Postcardiopulmonary bypass thromboelastography (TEG6s) with HKH assayPostcardiopulmonary bypass (CPB) coagulation profile using TEG6s in the HKH assay. The assay was performed prior to intensive care unit transfer.Overall, clot strength (HKH-MA) is 67.5 mm (reference range: 52–70 mm)Fibrinogen contribution to clot strength (ActF-MA) is 8.7 mm (reference range: 7–22 mm). Platelet function (ADP-MA) is 41.2 mm (reference range: 45–69 mm).
Postoperatively, bleeding in the intensive care unit was minimal. The total perioperative transfusion included 1,120 mL of RBCs, 960 mL of FFP, and 400 mL of platelets. On postoperative day 1, heparin infusion (10,000 units/day), aspirin, and warfarin (target PT-INR 2.0) were initiated. Postoperative echocardiography revealed an effective aortic valve area of 1.75 cm², and graft patency was confirmed angiographically. Predischarge blood tests were similar to preoperative values (WBC 16,400/μL, Hb 8.5 g/dL, and platelets 682 × 10³/μL). On day 21, the patient experienced lower gastrointestinal bleeding with progressive anemia progression (PT-INR 2.01 and stable platelets), attributed to an ascending colon diverticulum, and was successfully treated with endoscopic clipping. The patient was transferred to another hospital 28 days postoperatively.
Discussion
ET is a rare disorder within the spectrum of chronic MPNs, characterized by persistent peripheral blood thrombocytosis and platelet dysfunction, leading to a paradoxical tendency for both thrombosis and hemorrhage [4,5]. Here, we report a case of aortic valve and coronary artery stenosis complicated by ET managed with bioprosthetic aortic valve replacement and coronary artery bypass grafting.
Reports on open heart surgery in patients with ET are scarce. Gurrieri et al. documented a 28% perioperative complication rate in 25 ET patients undergoing cardiac surgery, with 80% of those experiencing complications having preoperative platelet counts exceeding 800 × 10³/μL [2]. The preoperative platelet count of our patient was 933 × 10³/μL, suggesting a heightened predisposition to complications.
In this case, we used the MAHKH and early parameters of the HKH assay to guide transfusion decisions perioperatively [6]. Preoperative assessments indicated adequate coagulation function, consistent with the patient's JAK2 mutation-positive status, a subtype associated with a high thrombotic risk. Postoperatively, the HKH assay revealed platelet dysfunction, prompting additional platelet transfusions, after which no pericardial bleeding occurred.
Three weeks after surgery, the patient developed anemia due to lower gastrointestinal bleeding [7]. With a therapeutic range PT-INR and stable platelet count, this event was more likely attributable to an ascending colon diverticulum than to ET or postoperative sequelae.
Conclusions
Herein, we present the case of a patient with ET who underwent aortic valve replacement and coronary artery bypass grafting. Intraoperative coagulation function was assessed using TEG6s, which enable targeted transfusion therapy. Lower gastrointestinal bleeding on postoperative day 21 was not associated with ET.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Essential thrombocythemia: 2024 update on diagnosis, risk stratification, and management Am J Hematol Tefferi A Vannucchi AM Barbui T 6977189920243826957210.1002/ajh.27216 · doi ↗ · pubmed ↗
- 2Essential thrombocythemia and cardiac surgery: a case series and review of the literature Ann Thorac Surg Gurrieri C Smith BB Nuttall GA Pruthi RK Said SM Smith MM 48249010620182970536910.1016/j.athoracsur.2018.03.057 · doi ↗ · pubmed ↗
- 3Thrombocytapheresis: managing essential thrombocythemia in a surgical patient Ann Thorac Surg Das SS Bose S Chatterjee S Parida AK Pradhan SK 0692201110.1016/j.athoracsur.2011.02.05021718822 · doi ↗ · pubmed ↗
- 4Efficacy of point-of-care thromboelastography 6s to evaluate platelet function in a patient with pseudothrombocytopenia undergoing cardiopulmonary bypass: a case report JA Clin Rep Chiba Y Otsuka Y Lefor AK Sanui M 8820223507678210.1186/s 40981-022-00496-6PMC 8789975 · doi ↗ · pubmed ↗
- 5A novel approach to essential thrombocythemia and cardiac surgery Ann Thorac Surg Smith BB Nuttall GA Pruthi RK Joyce DL Schuldes MS Smith MM 050103201710.1016/j.athoracsur.2016.08.06528219560 · doi ↗ · pubmed ↗
- 6Validity and utility of early parameters in TEG 6s platelet mapping to assess the coagulation status during cardiovascular surgery with cardiopulmonary bypass Cureus Yoshikawa Y Maeda M Ohno S 015202310.7759/cureus.38044 PMC 1020800837228566 · doi ↗ · pubmed ↗
- 7Postoperative bleeding in essential thrombocytosis patients with colorectal cancer: case report and literature review Int J Surg Case Rep Varela C Nassr M Razak A Yang SY Kim NK 1063748620213450719010.1016/j.ijscr.2021.106374 PMC 8433273 · doi ↗ · pubmed ↗