Dacryoadenitis associated with linear scleroderma en coup de sabre: A case report and review of literature
Eva Oustabassidis, Shay Keren, Joel David, Jonathan H. Norris

TL;DR
This case report describes a rare instance of dacryoadenitis occurring alongside linear scleroderma en coup de sabre, a skin condition, and shows successful treatment with methotrexate.
Contribution
This is the first documented case linking dacryoadenitis with linear scleroderma en coup de sabre.
Findings
Dacryoadenitis was diagnosed alongside linear scleroderma en coup de sabre in a 42-year-old woman.
Oral methotrexate effectively reduced symptoms of dacryoadenitis and scleroderma without steroid use.
Histological and clinical findings confirmed the coexistence of both conditions.
Abstract
Dacryoadenitis in the setting of linear scleroderma en coup de sabre (LScs) is an association that has not previously been described in the scientific literature. The purpose of this case report is to describe the co‐existence of LScs and chronic dacryoadenitis and how it was managed. We report the case of a 42‐year‐old woman who presented with a 4‐month history of left upper eyelid swelling with radiological enlargement of the left lacrimal gland on orbital CT and MRI imaging. Clinical examination revealed a left erythematous, swollen upper eyelid with lateral conjunctival injection and a palpable left lacrimal gland. An ipsilateral band‐like cutaneous depression in the fronto‐temporal region was also noted, which extended to the ipsilateral upper eyelid and brow. Serology revealed nucleolar antinuclear antibodies. A further incisional biopsy of the lacrimal gland confirmed chronic…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
 FIGURE 1
FIGURE 1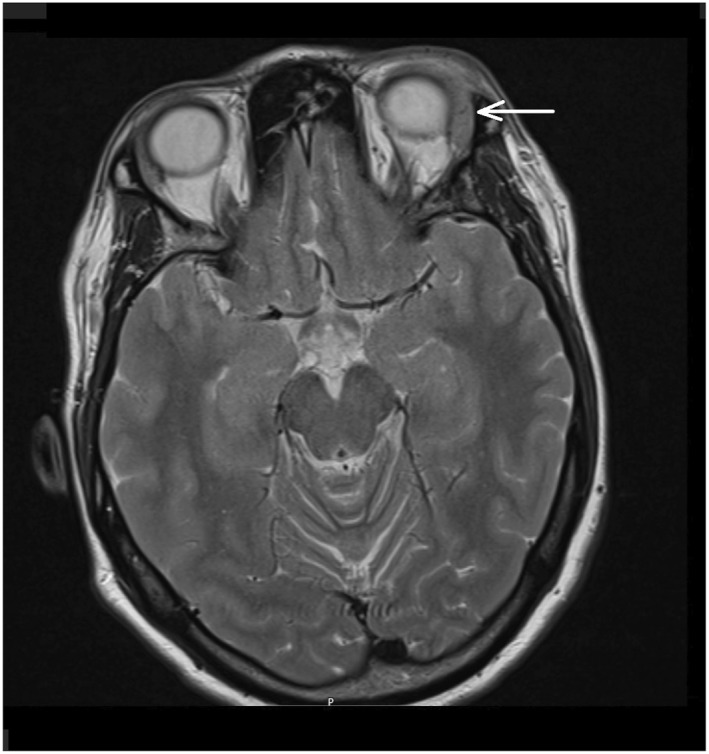 FIGURE 2
FIGURE 2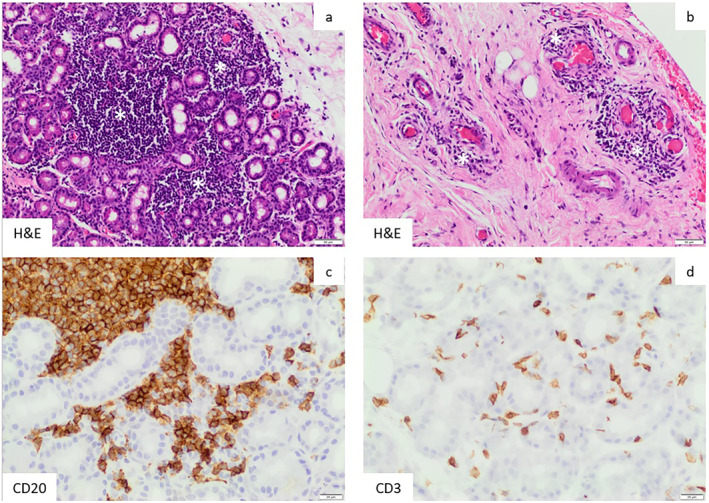 FIGURE 3
FIGURE 3- —This research received no specific grant from any funding agency in the public, commercial, or not‐for‐profit sectors
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsSystemic Sclerosis and Related Diseases · Autoimmune Bullous Skin Diseases · Dermatologic Treatments and Research
INTRODUCTION
1
Linear scleroderma, a subtype of localized scleroderma, is a condition of unknown origin1 in which an area of skin and subcutaneous tissue and occasionally deeper tissue become thickened and scarred with increased collagen deposition. Linear scleroderma en coup de sabre (LScs) is a subset of linear scleroderma and is characterized by a scar‐like band of skin predominantly affecting the scalp and upper face.2 Several ophthalmological findings in scleroderma have been previously reported.3 Fibrotic eyelid skin changes leading to thickening, tightness, telangiectasia, blepharophimosis or lagophthalmos have been reported. Other ocular manifestations include keratoconjunctivitis sicca, episcleritis, uveitis, and dacryocystitis. We present a unique case of chronic dacryoadenitis associated with linear scleroderma en coup de sabre which to our knowledge has not been reported. Written consent from patient was obtained for publication. This case report follows the CARE Guidelines.4
NARRATIVE
2
A 42‐year‐old healthy female presented to the Oculoplastic clinic with a 4‐month history of left upper eyelid swelling associated with ipsilateral conjunctival redness. History revealed investigation in relation to a history of fever, joint pain, head rash, and a left forehead scar that followed an episode of right lateral upper eyelid swelling. She described left periocular pain extending to the ipsilateral forehead. On examination, visual acuity was 6/6 in both eyes and ocular movements were full with normal optic nerve function. On the left side, there was a lateral upper eyelid oedema associated with lateral bulbar conjunctival injection. The left lacrimal gland was palpable and enlarged. A linear depression of the skin was noted to be extending from the lateral left upper eyelid, through the lateral eyebrow to the fronto‐temporal hairline. The skin changes were suggestive of an en coup de sabre seen in linear scleroderma (Figure 1).
Left‐sided fronto‐temporal band‐like skin changes suggestive of linear scleroderma ‘en coup de sabre’.
Blood work showed normal full blood count, CRP, ESR, and ACE. Immunoglobulin blood levels, IgG4 subclass, as well as serum protein electrophoresis were normal. ENA, ANCA, and dsDNA antibodies were negative. ANA was positive with a titre of 320 (laboratory standards 0–80) and a nucleolar pattern on immunofluorescence. Orbital CT and MRI demonstrated an enlarged left lacrimal gland (Figure 2).
MRI T2‐weighted, axial plane. Enlargement of left lacrimal gland.
Initial management by the referring hospital included oral Co‐amoxiclav and IV methylprednisolone 500 mg for 3 days followed by oral prednisone on a tapering regimen which improved eyelid inflammation. Any dosage of prednisolone below 30 mg resulted in recurrence of symptoms.
A left lacrimal gland biopsy via an anterior orbitotomy was performed under general anaesthesia. Oral prednisolone was progressively reduced to 10 mg a day prior to surgery to reduce the steroid masking effect of histopathological signs. Histopathology (Figure 3) revealed a patchy chronic lymphoplasmacytic inflammation of the lacrimal gland with no lymphoid cell atypia or granuloma. The infiltrate comprised a mixture of CD20 positive B‐cells and CD3 positive T‐lymphocytes. There was no evidence of IgG4 expression. The inflammation extended into adjacent fibrous tissue and orbital muscle with a perivascular pattern; there was no vasculitis.
Histopathology. Biopsy tissue demonstrates lymphocytic dacryoadenitis (a, c, d) with the inflammation extending into adjacent fibrotic soft tissues in a perivascular pattern (b). White asterisks in (a) and (b) indicate collections of lymphocytes. The brown reaction product in (c) and (d) highlights individual B‐cells (CD20+) and T‐cells (CD3+), respectively.
In the first year following the lacrimal biopsy, the patient remained relatively asymptomatic, bar persistent left upper eyelid oedema without tenderness. At 12 months, however, she developed a left‐sided sectoral episcleritis in conjunction with eyelid swelling and left‐sided headaches and so was commenced on oral methotrexate (MTX) 15 mg once per week for 2 weeks then increased to 20 mg once per week with folic acid 5 mg per week. The patient was reviewed 3 months later and reported a sustained reduction in the left periocular pain as well as less frequent episodes of eyelid swelling. There was no evidence of episcleritis or dacryoadenitis. The en coup de sabre scar showed no sign of active inflammation. She was maintained on MTX 20 mg per week and the steroid successfully weened.
PATIENT PERSPECTIVE
3
Before the diagnosis, I used to have a constant pain to my left eye with headaches. I needed to regularly take ibuprofen and omeprazole which upset my stomach. I felt relieved when doctors found out what was the underlying issue and also why I had this scar on my forehead. Thankfully, once I started taking MTX, my headache and my eyelid swelling reduced and I was able to enjoy my activities again.
DISCUSSION
4
Localised scleroderma is a non‐hereditary, autoimmune condition of unknown aetiology. The pathogenesis is still not fully understood. Immune activation is thought to be the initial step in the pathological process and is targeted against the endothelium of small blood vessels.5 This process results in tissue fibrosis and vascular structural changes such as destructive vasculopathy and proliferative obliterative vasculopathy. Similar perivascular changes and fibrosis were also seen in the lacrimal gland specimen in this case. The area of dermal inflammation and subsequent fibrosis leads to palpable thickening and hyperpigmentation.6 Changes also affect the deeper layers of the subdermis, fat, fascia, muscle, and can lead to bone damage and atrophy of the tongue and jaw deformity.7
Scleroderma en coup de sabre refers to ‘the blow of a sword’ and is a subset of localised scleroderma usually manifesting as a unilateral linear atrophic depressed cutaneous band with possible sclerosis localised on the forehead or scalp. It affects children more commonly and is more predominant in females than males (3:1).6
Ocular and orbital manifestations in linear scleroderma observed so far are poorly described in the literature. Reported findings include atrophy of the eyelid, eyelashes and eyebrow which may be associated with enophthalmos. These manifestations are thought to result from late trophic changes in the overlying skin sclerosis.8 Ipsilateral episcleritis, such as in our patient, anterior uveitis, and extraocular muscles involvement (thinning and fibrosis) may occasionally occur. Refractive changes and pseudopapilloedema have also been reported in the paediatric community.9 Dry eye is a less well reported association with LScs.10 One report describes tear secretion deficiency related to scleroderma without knowing the exact pathological mechanism.11 It may be that this was related to low‐grade dacryoadenitis.
One paper describes LScs with associated nasolacrimal duct obstruction and prolonged dacryocystitis12 occurring as a result of occlusive fibrosis. The finding of dacryoadenitis in our case report suggests deep organ involvement in the context of LScs and identifies an ophthalmological association of the disease which has not previously been described in literature. Dacryoadenitis refers to the inflammation of the lacrimal gland which is located supero‐temporally to the globe. Clinical manifestation is with a painful red enlarged lacrimal gland associated with an S‐shape deformity of the upper eyelid. Biopsy of the lacrimal gland is key if an underlying immune disease is suspected. Inflammatory causes may respond to steroids or demonstrate a chronic relapsing course requiring long‐term immunomodulatory therapy to maintain remission.13
Methotrexate has been extensively studied for the treatment of LScs and 100% responding rate has been reported.14
CONCLUSION
5
This case illustrates for the first time the finding of chronic dacryoadenitis in the context of LScs. Recognising the association and investigation with slit lamp examination, imaging, and histopathology is key to enhance optimum care of patients and reduces the risk to develop long‐term ocular dryness form scarred lacrimal gland which could lead to corneal infection and ulceration. Methotrexate can effectively and safely manage both conditions and should be considered as an early therapy to avoid exposing patients to the detrimental side‐effects of steroids.
AUTHOR CONTRIBUTIONS
Eva Oustabassidis: Conceptualization (lead); writing – original draft (lead); writing – review & editing (lead). Shay Keren: Writing – review & editing (supporting). Joel David: Writing – review & editing (supporting). Jonathan H. Norris: Supervision (lead); writing – review & editing (supporting).
CONFLICT OF INTEREST STATEMENT
None to declare.
ETHICS STATEMENT
Not applicable.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Katz KA . Frontal linear scleroderma (en coup de sabre). Dermatol Online J. 2003;9(4):10. 10.5070/d 335z 8t 4ms 14594583 · doi ↗ · pubmed ↗
- 2Varga J , Denton CP , Wigley FM , et al. Scleroderma: from pathogenesis to comprehensive management. Springer International Publishing; 2016.
- 3Gomes B de AF , Santhiago MR , Magalhães P , de Azevedo MNL , Moraes HV . Ocular findings in patients with systemic sclerosis. Clinics. 2011;66(3):379–385. 10.1590/s 1807-59322011000300003 21552659 PMC 3071995 · doi ↗ · pubmed ↗
- 4Riley DS , Barber MS , Kienle GS , Aronson JK , von Schoen‐Angerer T , Tugwell P , et al. CARE guidelines for case reports: explanation and elaboration document. J Clin Epidemiol. 2017;89:218–235. 10.1016/j.jclinepi.2017.04.026 28529185 · doi ↗ · pubmed ↗
- 5Asano Y . Systemic sclerosis. J Dermatol. 2018;45(2):128–138. 10.1111/1346-8138.14153 29226387 · doi ↗ · pubmed ↗
- 6Careta MF , Romiti R . Localized scleroderma: clinical spectrum and therapeutic update. An Bras Dermatol. 2015;90(1):62–73. 10.1590/abd 1806-4841.20152890 PMC 432370025672301 · doi ↗ · pubmed ↗
- 7Dixit S , Kalkur C , Sattur AP , Bornstein MM , Melton F . Scleroderma and dentistry: two case reports. J Med Case Rep. 2016;10(1):297. 10.1186/s 13256-016-1086-1 27776552 PMC 5078903 · doi ↗ · pubmed ↗
- 8Fledelius HC , Danielsen PL , Ullman S . Ophthalmic findings in linear scleroderma manifesting as facial en coup de sabre. Eye. 2018;32(11):1688–1696. 10.1038/s 41433-018-0137-9 29973692 PMC 6224534 · doi ↗ · pubmed ↗