Steps to improve the teaching of clinical reasoning in dermatology: A scoping review and proposal
Aliya Rodriguez, Christopher Farkouh, Rebecca Raszewski, Claudia Hernandez

TL;DR
This paper reviews how clinical reasoning is taught and assessed in dermatology and suggests ways to improve training and evaluation methods.
Contribution
The paper proposes evidence-based strategies to enhance clinical reasoning teaching and assessment in dermatology.
Findings
Most studies on dermatology clinical reasoning use single interventions with small sample sizes.
Simulation-based studies are common, but process-based clinical reasoning interventions are rare.
Longitudinal data and work-based assessments are needed to improve dermatology training programs.
Abstract
Clinical reasoning (CR) is an area of active interest since faults in the diagnostic process can result in errors and possibly delays in care or even patient harm. The purpose of this scoping review was to collect information from the medical literature on approaches utilized to teach and assess CR in dermatology, identify gaps, and prepare a proposal on how to enhance the speciality's ability to develop trainee CR skills. We conducted a review of the published literature (1990–2020) from four databases. The initial search yielded 780 papers, and 42 relevant CR publications met inclusion criteria. Demographic, thematic content, theoretical frameworks, continuum of authenticity, competency/milestone, and assessment/educational intervention data were recorded by two screeners. Trainees at different educational levels from 17 different countries have been assessed in the dermatology…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
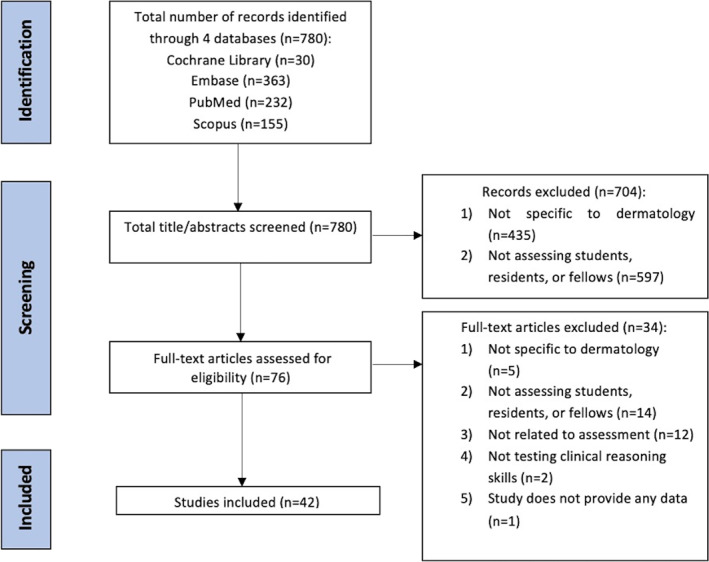 FIGURE 1
FIGURE 1| First author (year); location | Population & sample size | Duration | Study aim | Dermatology focus area | Thematic content coding | Continuum of authenticity | ACGME |
|---|---|---|---|---|---|---|---|
| Baker (2014); United States | First year medical students ( | 3 years | To report student survey results of an activity that provides a realistic setting in which students perform skin biopsies and learn about skin histology. | Medical dermatology & dermatopathology | Decision making | WBA | Patient care |
| Berger (2017); United States | Dermatology residents and pathology residents & fellows ( | Not specified | To determine whether examination scores would be equivalent when tested using two microscopy formats (glass slides & virtual). | Dermatopathology | Decision making | NWBA | Patient care |
| Brick (2013); United States | Dermatology residents ( | 1 academic year | To evaluate diagnostic accuracy and attitudes between virtual microscopy and glass slides. | Dermatopathology | Decision making | NWBA | Patient care |
| Cervantes (2017); United States | First and second year medical students ( | 1 month | To investigate the use of a cadaver to provide both cognitive and technical evaluations of skin biopsies. | Medical dermatology | Assess novel CR | Simulation | Medical knowledge |
| Cervantes (2019); United States | First and second year medical students ( | 2 weeks | To investigate the usefulness of computer‐based video instruction in dermatologic procedure training on a cadaver. | Procedural dermatology | Assess novel CR | Simulation | Patient care |
| Chaudhary (2017); India | 6th semester medical students ( | 6 months | To compare the effectiveness of computer assisted OSCE | Medical dermatology | Assess novel CR | Simulation | IPCS |
| Choi (2019); United States | Preclinical medical students ( | 4 weeks | To evaluate the effectiveness of a technology‐based visual perception training system for melanoma detection with an image‐based assessment of retention. | Medical dermatology | Decision making | NWBA | Medical knowledge |
| Cipriano (2013); United States | Fourth year medical students ( | 2 weeks | To determine the impact of the integration of the American Academy of dermatology online curriculum into a 2‐week dermatology clerkship by comparing scores on MCQ | Medical dermatology | Course/curriculum (>1 session); decision making | NWBA | Medical knowledge; patient care |
| Dietricha (2021); France | Dermatology residents ( | 6 months | To investigate the benefits of simulation training in the disclosure of melanoma diagnosis or treatment. | Medical dermatology | Assess existing CR | Simulation | IPCS |
| El Miedany (2010); England | Dermatology trainees ( | Not specified | To assess the efficacy of a simulated problem‐based learning educational activity for scoring the psoriasis area and severity index. | Medical dermatology | Assess novel CR | Simulation | Medical knowledge |
| Enk (2003); Israel | Sixth year medical students ( | 9 months | To determine the efficacy of a 2‐week dermatology elective by administering Kodachrome slide‐based MCQ | Medical dermatology | Course/curriculum (>1 session); decision making | NWBA | Medical knowledge |
| Fox (2017); United States | Second year medical students ( | 1 week | To determine the effectiveness of flipped classroom versus traditional classroom methodology by comparing MCQ | Medical dermatology | Course/curriculum (>1 session); decision making | NWBA | Medical knowledge |
| Garg (2010); United States | Second year medical students ( | 3 months | To determine the effectiveness of teaching with 3D prosthetic models of skin lesions versus 2D images by comparing MCQ | Medical dermatology | Education class (1 session); decision making; assess existing CR | NWBA | Medical knowledge; patient care |
| Garg (2015); United States | Third year medical students ( | 1 year | To develop an OSCE | Medical dermatology | Decision making; assess existing CR | Simulation | Medical knowledge; patient care |
| Goodyear (2005); United Kingdom | Senior hour officers ( | Not specified | To compare learning outcomes for a problem‐based learning course versus a traditional didactic course with an OSCE | Paediatric dermatology | Course/curriculum (>1 session); decision making | NWBA | Medical knowledge; patient care |
| Goulart (2012); United States | Second year medical students ( | 3 months | To evaluate recognition and response to a prosthetic melanoma placed on a standardized patient. | Medical dermatology | Decision making; assess existing CR | NWBA | Medical knowledge |
| Grover (2012); India | Sixth semester medical students ( | 4 months | To develop a computer assisted OSCE | Medical dermatology | Decision making; assess novel CR | Simulation | Medical knowledge; patient care |
| Hartmann (1998); United States | Second year medical students ( | Not specified | To develop interactive teaching mechanisms for a dermatology course and assess its effectiveness with a Kodachrome slide and MCQ | Medical dermatology | Course/curriculum (>1 session); decision making | NWBA | Medical knowledge |
| Hazan (2018); United States | Dermatology residents ( | 3 years | To evaluate the impact of cadaver training sessions on improving surgical knowledge with pre‐ and post‐intervention quizzes. | Procedural dermatology | Decision making; assess novel CR | Simulation | Patient care |
| Hernandez (2013); United States | Fourth year medical students ( | 6 months | To examine the student's ability to detect melanomas using standardized patients and moulage. | Medical dermatology | Decision making; assess existing CR | Simulation | Patient care |
| Jain (2013); United States | Third year medical students ( | 2 years | To evaluate a melanoma simulation model to teach visual assessment and counselling skills using standardized patients and moulage. | Medical dermatology | Assess novel CR | Simulation | Medical knowledge; patient care |
| Jenkins (2008); United States | Second year medical students ( | 4 days | To assess the effectiveness of an online tutorial in teaching morphology and terminology in comparison to traditional lectures. | Medical dermatology | Decision making | NWBA | Medical knowledge |
| Kaliyadan (2014); Saudi Arabia | Fifth year medical students ( | 3 weeks | To validate the use of a computer based OSCE | Medical dermatology | Decision making; assess novel CR | WBA | Medical knowledge; professionalism |
| Li (2013); China | Fourth year medical students ( | Not specified | To compare the impact of real patients, digital problem‐based learning, paper problem based‐learning, and traditional lecture‐based learning by administering a written exam and OSCE | Medical dermatology | Decision making | NWBA | Medical knowledge; patient care |
| Liu (2019); United States | Dermatology residents ( | Not specified | To assess the impact of a video‐based, flipped classroom curriculum and surgical simulation skin models on procedural skills. | Procedural dermatology | Decision making; course/curriculum (>1 session) | Simulation | Patient care |
| Marsch (2014); United States | Dermatology and pathology residents ( | 2 weeks | To determine the effectiveness of annotated digital pathology slides as a teaching tool by administering pre‐ and post‐tutorial MCQ | Dermatopathology | Decision making | NWBA | Patient care |
| Ochsendorf (2004); Germany | Medical students in sixth clinical term ( | 2 consecutive clinical terms | To compare a problem‐oriented practical course to a bedside teaching course and standard practical course with pre‐ and post‐course MCQ | Medical dermatology | Course/curriculum (>1 session); decision making | NWBA | Medical knowledge |
| Ochsendorf (2006); Germany | Medical students in sixth clinical term ( | 2 consecutive clinical terms | To determine whether a large group case‐based teaching approach combined with small group bedside teaching improves learning outcomes with pre‐ and post‐course MCQ | Medical dermatology | Course/curriculum (>1 session); decision making | NWBA | Medical knowledge |
| Pontius (2020); United States | Dermatology residents ( | 1 academic year | To determine if there is a difference in knowledge acquisition between traditional and flipped classrooms with a MCQ | Medical dermatology | Course/curriculum (>1 session); decision making | NWBA | Medical knowledge |
| Punj (2014); Australia | Sixth year medical students ( | Not specified | To investigate the value of tactile descriptive information of a lesion on the diagnostic accuracy of a pigmented skin lesion using MCQ | Medical dermatology | Decision making | NWBA | Medical knowledge; patient care |
| Reichel (2004); United States | Chief dermatology residents, residency programme directors, directors of dermatologic surgery ( | 4 months | To assess how the surgical skills of dermatology residents are taught and evaluated within the United States through a survey. | Procedural dermatology | Descriptive | N/A | Patient care |
| Rimoin (2015); United States | Pre‐clerkship medical students ( | 1 year | To investigate whether online perceptual and adaptive learning modules could efficiently train in skin lesion morphologies through MCQ | Medical dermatology | Decision making | NWBA | Medical knowledge |
| Robinson (1996); United States | Second‐ and fourth‐year medical students ( | 2 years | To determine the likelihood of skin cancer detection with a standardized patient and a written exam. | Medical dermatology | Decision making; assess existing CR | NWBA | Medical knowledge; patient care |
| Sabzwari (2017); Pakistan | Third‐year medical students ( | 1 day | To assess the validity and feasibility of moulage‐based simulation on standardized patients in summative assessment. | Medical dermatology | Decision making; assess existing CR | Simulation | Medical knowledge; patient care |
| Saceda‐Corraloa (2017); Spain | ‘Sixth grade’ medical students ( | 1 day | To determine the feasibility of implementation of a dermatology OSCE | Medical dermatology | Decision making; assess existing CR | Simulation | Medical knowledge; patient care; IPCS |
| Smith (2009); United States | Third year medical students ( | 1 year | To design a physical exam course and evaluate the course by developing an OSCE | Medical dermatology | Course/curriculum (>1 session); decision making | Simulation | Medical knowledge; patient care |
| Ternov (2020); Denmark | Medical students ( | 3 months | To develop and gather validity evidence for a MCQ | Medical dermatology | Decision making; assess existing CR | NWBA | Medical knowledge; patient care |
| Ulman (2015); United States | Fourth year medical students ( | 1 day | To assess whether a medical school curriculum is adequately preparing medical students to diagnose and treat common dermatologic conditions through administering a MCQ | Medical dermatology | Course/curriculum (>1 session); decision making; assess existing CR | NWBA | Medical knowledge; patient care |
| Wahlgren (2006); Sweden | Medical students in the 7th term ( | 3 consecutive 17‐day courses | To develop an interactive educational dermatology computer programme for medical students and evaluate it with a final written examination. | Medical dermatology | Decision making | NWBA | Medical knowledge; patient care |
| Waller (2019); Canada | Third year medical students ( | 1 week | To develop and evaluate the results of a dermatology stations programme including standardized patients, simulated procedures, and MCQ | Medical dermatology | Decision making | NWBA | Medical knowledge |
| Wanat (2013); United tates | Second year medical students ( | 3 years | To determine the effectiveness of a programme for teaching the total body skin exam using a standardized patient with moulage. | Medical dermatology | Decision making; assess existing CR | Simulation | Patient care |
| Wang (2015); United States | Dermatology residents ( | Not specified | To pilot the use of a melanoma simulation model to improve standardization of clinical findings in a dermatology OSCE | Medical dermatology | Decision making; assess novel CR | Simulation | Medical knowledge; patient care |
| Location |
|
|---|---|
| United States | 26 |
| Europe | 8 |
| India | 2 |
| China, Israel, Pakistan, Saudi Arabia, Australia, Canada | 1 (each) |
- —This article received no specific grant from any funding agency in the public, commercial, or not‐for‐profit sectors
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsClinical Reasoning and Diagnostic Skills · Innovations in Medical Education · Empathy and Medical Education
What is already known?
- The acquisition of clinical reasoning (CR) skills is a central objective in any medical training programme. However, little is known about how dermatology training programs are teaching and assessing CR. There are no standard guidelines on how to measure and improve CR acquisition amongst dermatology trainees.
What does this study add?
- This scoping review found that rigorous studies that examine CR in the teaching and assessment of trainees are lacking in the dermatology literature and offered proposals on how to enhance the speciality's ability to develop and assess CR skills.
INTRODUCTION
1
Critical to the achievement of medical competence is a poorly understood mental skill known as clinical reasoning (CR). Although definitions vary, CR is often described as ‘a skill, process, or outcome wherein clinicians observe, collect, and interpret data to diagnose and treat patients’.1 One of the central objectives of any residency programme is to develop accurate CR skills. Little is known about how dermatology residency programs (DRP) teach and assess CR.
Until recently, a multiple‐choice examination was utilized to evaluate dermatology graduates. This knowledge‐based exam heavily relied on memorization rather than scenarios requiring the application of medical knowledge to make accurate diagnostic and safe therapeutic decisions. In response, the American Board of Dermatology created the ‘applied’ exam where diagnostic and therapeutic decision‐making, both of which involve CR, is emphasized.2, 3 There is scant literature that can guide DRPs regarding the proper rate of CR development as well as standardized methods to measure CR acquisition of trainees throughout their training. Medical educators must continue to improve their understanding of CR development, how to accelerate its acquisition, and how to identify struggling learners early in their training and correct reasoning errors.4 The purpose of this scoping review was to collect information from the medical literature on the approaches utilized to teach and assess CR in dermatology, identify gaps, and prepare a proposal on how to enhance the specialty's ability to develop trainee CR skills.
BACKGROUND
2
Medical educators describe the challenge of CR research as trying to make the ‘invisible’ ‘visible’.5 A common starting point is to simplify CR by dividing it into a series of tasks. For example, Daniel et al.6 proposed seven CR tasks: (1) information gathering; (2) hypothesis generation; (3) problem representation; (4) generation of a differential diagnosis; (5) selection of a leading/working diagnosis; (6) diagnostic justification; and (7) development of management/treatment plan. Novices versus experts move with different levels of efficiency between steps.6 An ‘expert’ clinician appears to heavily rely on ‘intuitive, nonanalytic reasoning’ to rapidly generate an accurate diagnostic hypothesis.7 To achieve this level of expertise, Dreyfus and Dreyfus described a 5‐level staged progressive learning model that hinges on the student being exposed to progressive challenges in CR/skill scenarios.8 This forms the basis of a residency's experiential learning model since it is probable that experience plays an essential role in accurate problem representation.9 Some question whether CR can ever be truly separated from an individual's fund of knowledge/experience. In other words, are ‘experts’ simply in possession of a larger fund of knowledge? If amassing knowledge is the critical link then opportunities for deliberate practice should continue to form the backbone of training programs. Yet it seems clear that even when possessing vast knowledge, it has limits in its ability to explain CR skills. Expert clinicians also appear to have a superior ability to mentally organize increasingly intricate sets of clinical information for rapid retrieval without sacrificing diagnostic accuracy.10, 11, 12, 13 Efforts to understand the CR process have given rise to a number of conceptualizations that reflect different theoretical approaches and asssumptions about it.
A review of CR theories by Yazdani et al.9 divided them into three categories: (1) process‐based theories/models (T/M); (2) knowledge‐structure‐based T/M, and (3) compilation T/M. The first category (process‐based T/M) utilizes the hypothetico‐deductive model,9, 10, 11, 12, 13, 14 where CR is viewed as a largely sequential process with physicians generating a number of hypotheses that generate the basis for further enquiries to test them. The second category (knowledge‐structure T/M) utilizes illness script theory,9 where novices organize increasing amounts of knowledge into ‘illness scripts’.15 Scripts are list‐like mental structures with three components (predispoing conditions, pathophysiological insult, and clinical consequences). Clinicians incorporate additional factors into scripts and continually reorganize them creating greater ease of access when key history or clinical findings trigger memories.11, 13, 16 The third category (compilation T/M) utilizes either dual process or cognitive continuum theories.9 Dual process combines intuition, pattern recognition, as well as experience that are activated in System 1 to rapidly arrive at a diagnosis. Some complex diagnoses require a more analytic approach comparing previously constructed cases in a second process known as System 2, hence dual process.17 As a clinician gains greater experience, they can link new cases with previously constructed illness lists with greater efficiency and seamlessly shift, with minimal cognitive effort, been the two‐systems.18 A weakness of each of these 3 T/M is that they focus on one specific portion of CR and not the entire process. Most fail to account for external factors such as emotions, time available with patients, irrelevant signs/symptoms, and their impact on the processes used to reach a correct diagnosis.18, 19
What is found in the medical literature regarding methods used to teach and assess CR in dermatology? A better understanding of this process could lead to improvements in instruction as well as assessment methods that could accelerate the acquisition of CR among medical students, residents, and even practicing physicians. The scoping review approach was selected because it allows for exploration of current CR publications in dermatology, therefore allowing our team to identify important future CR projects for dermatology.
MATERIALS AND METHODS
3
The five‐stage methodological framework for scoping reviews published by Arksey and O’Malley in 200520 was used for this review. The five steps are as follows: (1) identify the research question; (2) identify relevant studies; (3) select relevant studies; (4) chart the data; and (5) data summary and reporting.
The research team consisted of two medical students, a medical librarian, and the author. For step 2, the librarian performed subject and keyword searches based on the following concepts: dermatological or skin‐related disorders; medical educational groups such as students, residents, and fellows; patient simulation; and CR and examination methods. The following databases were used: Cochrane Library, Embase, PubMed, and Scopus. Inclusion criteria were: (a) peer‐reviewed journal articles, (b) original data, (c) from 1990 to 2020, (d) focused on CR interventions (either instruction/assessment, or discussions could be included), and (e) limited to dermatology. Exclusion criteria were: (a) non‐English language studies without an available translation; (b) book review and editorials; (c) studies not examining dermatology CR; (d) studies of health professionals who were not medical students, residents, or fellows, and; (e) dermatology theoretical CR literature reviews since they were often summaries of CR publications readily available in the medical education literature.
Data collection proceeded with two screeners performing narrative review and documenting the following information: author(s), title, publication year, study objective/aims, intervention, duration, study population, methods, outcome measures, results, analysis, major themes, assessed accrediation council for graduate medical education (ACGME) milestones, location (United States vs. other), work‐based assessment (WBA), non‐WBA, simulation, dermatology subject‐matter focus (dermatopathology, paediatric dermatology, general dermatology, procedural), and limitations.21 A 3rd screener reviewed all data files for accuracy and served as a ‘tie‐breaker’ for discordant findings. Microsoft Excel (Microsoft, Redmond) was used to faciltate descriptive data collection, analyses, and graphical presentations.
RESULTS
4
The initial search of the four databases yielded 780 papers as follows: Cochrane Library n = 30; Embase n = 363; PubMed n = 232; and Scopus n = 155. Of the screened manuscripts, 76 met initial inclusion criteria and upon further review, the selection was narrowed to 42 relevant publications (step 3) (Figure 1). Appendix S1 (see Supporting Information) contains a list of the 42 publications in alphabetical order. An overview of the included publications is provided in Tables 1 and 2. Our interrater concordance was 94%.
Preferred Reporting Items for Systematic Reviews and Meta‐Analyses flow diagram.
Demographics
Charting the data (step 4) began by collecting demographics. Studies from outside the U.S. complicated the review process due to differences in training rotations and duration. Despite this, we found trainees at different educational levels from 17 different countries that participated in dermatology CR studies. Eleven CR interventions utilized residents while 31 involved medical students. Except for a single publication, all interventions utilized a single academic year and/or class meaning no studies evaluated multi‐year CR progression among trainees or tried to determine performance targets by post‐graduate year. No publications examined dermatology faculty CR knowledge/skills in either teaching or assessment domains.
Theoretical framework
Published dermatologic education interventions were categorized into knowledge‐versus process‐versus compilation‐based.22 The process‐oriented CR approach teaches learners how to reason via the use of clinical cases to breakdown student's reasoning by reviewing diagnostic algorithms, specific CR steps, or evaluating and ranking clinical information. Sessions are typically interactive and use a hypothetico‐deductive CR framework. Knowledge‐based CR interventions use a pathophysiological mechanistic approach that supports learning distinctions between similar or lookalike diseases. Compilation is a mixed analytic and non‐analytical approach. Unfortunately, most publications did not describe interventions in sufficient detail to categorize them with high accuracy however knowledge‐based interventions appear to be much more common. Since dermatology utilizes visual processes that rely on a non‐analytical approach, mixed approaches are likely underappreciated.
Thematic content coding
The majority of published manuscripts focused on an area of medical dermatology; four focused on new dermatopathology technology (comparison of glass slides vs. digitized images), four interventions were in procedural dermatology (skill development in cadaveric labs), while only one manuscript concentrated on paediatric dermatology. Published manuscripts described the development of: (a) new course/curriculum (more than one session), n = 11; (b) new educational session (single session), n = 2; (c) decision‐making exercise or assessment, n = 39; (d) evaluation of an existing CR assessment method, n = 12; (e) development of a new CR assessment method, n = 9; or (f) descriptive publication, n = 1. A publication could have more than one theme. Of the relevant articles, 39 out of 42 utilized a decision‐making scenario, however, interventions focused on CR process results did not attempt to understand how data is integrated to reach a diagnosis. Research publications largely focused on improving education in one area of dermatology (i.e. melanoma diagnosis).
Continuum of authenticity
Education interventions included computer‐based modules/flipped classrooms (n = 3), problem‐based learning (n = 3), simulated patients and cadaveric exercises, while interventions that focused on trainee assessment included computer‐based/online/CD‐ROM (n = 15), prosthetic/moulage (n = 9), images (n = 5), objective structured clinical examinations (n = 6), and cadaveric models (n = 3). Some publications used the same method (i.e. simulation) for both education and assessment of trainees resulting in mixed formats. Daniel et al.6 divided CR assessments into WBA, non‐WBA, and assessments in simulated environments (SIM) to categorize them along a ‘continuum of authenticity’. WBA are able to measure multiple components of CR in real clinical settings (high authenticity), followed by SIM, and non‐WBA (typically occurs in classroom).6 Non‐WBA (n = 24) were the most commonly used category in the dermatology literature likely due to their high internal consistency and ease of use across large numbers of learners. Their ability to assess CR is questioned since they are considered ‘part‐task’ due to their inability to capture the ‘whole’ CR process. Even less known is how these classroom‐based skills transfer to the clinical environment. SIM (n = 23) follows closely in the number of published studies and is valuable because SIM can assess multiple CR components. However, high‐fidelity simulations are expensive due to the resources needed to develop and administer them. Most published SIM (often using moulage) reports are small pilot studies making their eventual role in dermatology education unclear. WBA (n = 2) were vastly under‐represented despite their ability to assess multiple components of CR in authentic clinical settings.
Assessment of ACGME core competencies/milestones
The ACGME milestones are patient care, medical knowledge, practice‐based learning and improvement (PBLI), interpersonal and communication skills (IPCS), professionalism, and systems‐based practice (SBP). Four milestones had assessments in the published dermatology literature: (1) medical knowledge, n = 31, (2) patient care, n = 27, (3) IPCS, n = 3, and (4) professionalism, n = 1. 33 interventions had a mixed data collection that included both medical knowledge and patient care outcomes. Research on the potential use of simulation as well as the development of WBAs could help address the lack of published milestone outcome data for PBLI or SBP and increase the rigour of the assessments for all milestones.
DISCUSSION
5
Scoping reviews explore the current literature with the goal of identifying gaps that point to potential future areas of research. Studies that examine practical CR targets for teaching and assessment among dermatology medical students/residents are lacking. Our scoping review also found a lack of published CR process‐oriented research. Published studies lack documentation on the use of CR algorithmic approaches, Bayes theorem (a theorem used in CR where the probability of a diagnosis is based on the disease prevalence and the sensitivity/specificity of the diagnostic test), distinction between pertinent positive and negative/normal findings, etc. when instructing trainees and instead appear to approach differential diagnosis from a knowledge‐structure standpoint by reviewing lists of similar diseases. This likely reflects a lack of clarity regarding the CR processes and/or its amorphous nature making it a challenge to know how to best approach teaching it.
Studies on dermatologic CR deserve a rigorous approach given our specialty's unique mix of medical and procedural patient care along with its reliance on visual recognition patterns. One possible starting point is to consider carrying out in‐depth interviews with recognized expert teachers to explore their thinking algorithms. In other words, dermatology should invest in metacognition exploration to better understand expert CR regarding skin disease. Creation of detailed algorithmic mapping of the integration of clinical data could help make dermatologic CR more concrete or visible to trainees. It is likely that experts approach complex diagnosis by performing mathematical probabilistic calculations when weighing data points. Increasing trainee comfort levels with this approach could improve diagnostic accuracy when pattern recognition is not sufficient to diagnose a patient. Another possible benefit to this approach is in the area of diagnostic error. Process‐oriented research could lead to a better understanding of where diagnostic errors begin to occur in skin disease diagnosis allowing faculty to improve diagnostic education exercises by targeting common errors and developing effective remediation programs.
Quantitative methods to evaluate diagnostic performance remain elusive in medicine and dermatology is no exception. More research is needed to help faculty utilize WBA given dermatology's dependence on outpatient clinics as its principal teaching environment. There are many challenges to assessing residents here including time, high patient volumes, and the nonsystematic nature of clinical practice resulting in over‐ and under‐representation of certain diseases. Association of Professors of Dermatology and American Academy of Dermatology could help develop programs to train faculty on the use of simple and inexpensive WBA CR education/assessment tools such as think alouds, charts recall, etc. and fund studies to develop effective specialty‐specific outpatient direct observation tools.
Faculty would also benefit from a robust framework that details how to best assess trainees and their expected clinical and procedural proficiencies at different points in their training. Dermatology educational research needs to increase study sample sizes so they are multi‐institutional and span then length of a residency programme in order to be able to provide longitudinal data with expected progressive developmental targets in regards to resident performance. Faculty should feel at ease choosing from several CR assessments in order to provide robust feedback to trainees.
Given the small size of many DRP, development of a national educational resource portal or toolkit could assist smaller residency programme faculty. A CR toolkit with critical materials such as expert recordings, discussion boards, and links to up‐to‐date resources could increase faculty comfort levels with some under‐utilized assessment tools such as WBAs. The goal of the toolkit could be to help faculty construct CR objectives as well as correctly choose and employ CR assessments. APD or AAD's web‐based platforms and annual meetings could represent an opportunity for hands on practice in regards to CR education and assessment. Establishing a means for faculty to learn and collaborate may advance CR understanding by providing a mechanism to increase sample size and expand the generalizability of future studies.
There are several limitations to our scoping review including access only to published data since internal training programme tracking mechanisms are not available for review. Our search string could have missed an important CR publication, and reviewing manuscripts required several months to screen meaning recent publications may have not been included in this review. Multi‐specialty interventions that included dermatology could have also been missed in the screening process. Lastly, screeners needed to make decisions/judgements about multiple components of studies that were not always explicitly defined by authors.
CONCLUSIONS
6
The importance of CR in the development and eventual skill set of a practicing physician cannot be understated. This review found that dermatology CR research is largely focused on trainee knowledge‐based exercises. Dermatology would benefit from longitudinal data on knowledge as well as process‐based CR programs, metacognition CR exploration specific to skin disease diagnosis, faculty development programs to increase the use of WBA, and studies that yield practical recommendations about how faculty should choose from a menu of CR tools to construct a multi‐faceted education and assessment programme.
AUTHOR CONTRIBUTIONS
Aliya Rodriguez: Data curation (lead); formal analysis (lead); investigation (lead); writing – original draft (supporting); writing – review & editing (lead). Christopher Farkouh: Data curation (lead); formal analysis (lead); investigation (lead). Rebecca Raszewski: Data curation (lead). Claudia Hernandez: Conceptualization (lead); formal analysis (supporting); investigation (supporting); methodology (lead); supervision (lead); writing – original draft (lead); writing – review & editing (supporting)
CONFLICT OF INTEREST STATEMENT
Claudia Hernandez, MD, MEHP is an editor at JAMA Dermatology. The other authors have no conflicts of interests to disclose.
ETHICS STATEMENT
Not applicable.
Supporting information
Supporting Information S1
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Eva KW , Hatala RM , Le Blanc VR , Brooks LR . Teaching from the clinical reasoning literature: combined reasoning strategies help novice diagnosticians overcome misleading information. Med Educ. 2007;41(12):1152–1158. 10.1111/j.1365-2923.2007.02923.x 18045367 · doi ↗ · pubmed ↗
- 2American Board of Dermatology . ABD certification pathway info center. Availabe from: https://www.abderm.org/residents‐and‐fellows/abd‐certification‐pathway/abd‐certification‐pathway‐info‐center. Accessed 2 October 2023.
- 3Gruppen L . Clinical reasoning: defining it, teaching it, assessing it, studying it. West J Emerg Med. 2017;18(1):4–7. 10.5811/westjem.2016.11.33191 28115999 PMC 5226761 · doi ↗ · pubmed ↗
- 4Cassel CK , Holmboe ES . Professionalism and accountability: the role of specialty board certification. Trans Am Clin Climatol Assoc. 2008;119:295.18596848 PMC 2394686 · pubmed ↗
- 5Delany C , Golding C . Teaching clinical reasoning by making thinking visible: an action research project with allied health clinical educators. BMC Med Educ. 2014;14(1):20. 10.1186/1472-6920-14-20 24479414 PMC 3912345 · doi ↗ · pubmed ↗
- 6Daniel M , Rencic J , Durning S , Holmboe E , Santen SA , Lang V , et al. Clinical reasoning assessment methods: a scoping review and practical guidance. Acad Med. 2019;94(6):902–912. 10.1097/acm.0000000000002618 30720527 · doi ↗ · pubmed ↗
- 7Brush JE , Sherbino J , Norman GR . How expert clincians inutitively recognize a medical diagnosis. Am J Med. 2017;130(6):629–634. 10.1016/j.amjmed.2017.01.045 28238695 · doi ↗ · pubmed ↗
- 8Dreyfus HL , Dreyfus SE . Mind over machine: the power of human intuition. New York: Free Press; 1986.