A case of Rowell syndrome after a herpes simplex infection and prolonged sun exposure
Ariana Palacio, Karla Medrano Cebrian, Michael Majores, Manfred Uerlich, Erhard Bierhoff, Sonja Bonness, Uwe Reinhold

TL;DR
This paper presents a case of Rowell Syndrome in a 43-year-old man following a herpes infection and sun exposure, highlighting its rare combination of skin conditions and successful treatment.
Contribution
The paper contributes a new clinical case of Rowell Syndrome triggered by herpes simplex and sun exposure, with a successful treatment response to topical corticosteroids and calcineurin inhibitors.
Findings
Rowell Syndrome can occur after herpes simplex type 1 infection and sun exposure.
The patient showed good response to topical corticosteroids and calcineurin inhibitors.
The case highlights the importance of recognizing Rowell Syndrome's combination of EEM and SCLE.
Abstract
Rowell Syndrome is a rare entity combining erythema exudativum multiforme (EEM) and lupus erythematosus (LE). Zeitouni et al. redefined Rowell Syndrome's diagnostic criteria. Major criteria include: (1) LE (systemic, discoid or subacute cutaneous), (2) EEM‐like skin lesions and (3) speckled pattern of antinuclear antibodies. Minor criteria comprise: (1) chilblains, (2) positive anti‐SSA/Ro or anti‐SSB/La antibodies and (3) positive rheumatoid factor. The diagnosis is achieved when all major criteria and at least one minor criterion are present. Prognosis and treatment regimens are those of EEM and LE, with reported good response to oral cortisone, azathioprine, cyclosporine, dapsone, antimalarials and methotrexate. We present a case of Rowell Syndrome in a young adult after a herpes simplex type 1 infection and unprotected sun exposure, with good response to both topical corticosteroids…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
 FIGURE 1
FIGURE 1 FIGURE 2
FIGURE 2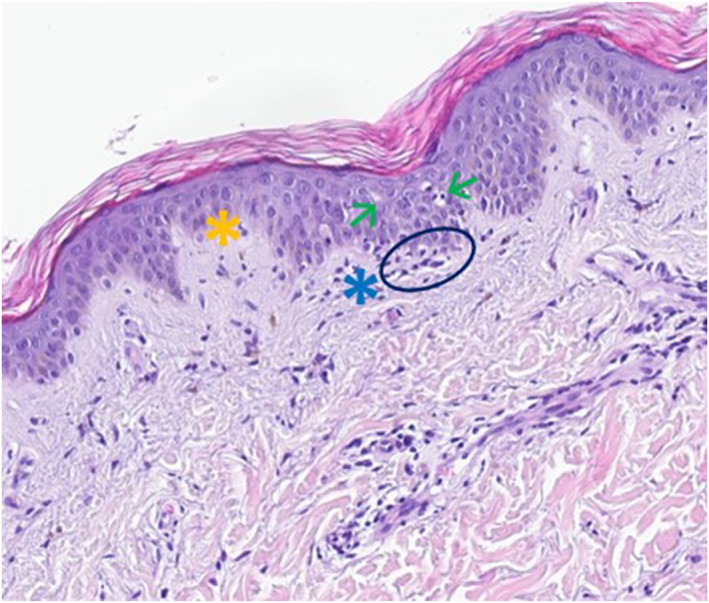 FIGURE 3
FIGURE 3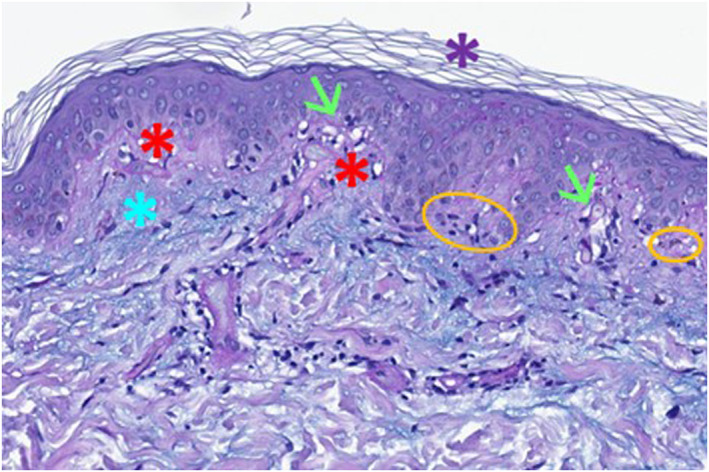 FIGURE 4
FIGURE 4- —This research received no specific grant from any funding agency in the public, commercial, or not‐for‐profit sectors
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsSystemic Lupus Erythematosus Research · Drug-Induced Adverse Reactions · Muscle and Compartmental Disorders
INTRODUCTION
1
We present a case of an otherwise healthy 43‐year‐old man of Balkan descent with a 3‐week history of general malaise and skin rashes on his trunk and upper extremities. The symptoms appeared at the beginning of his holidays in the Dominican Republic after the first day of sun exposure without sunscreen and subsequent sunburn on his neck and shoulders. The patient reported no intake of medication and did not have any known illnesses other than an unclear relapsing alopecia in stress phases with good response to topical minoxidil and betamethasone.
During the physical examination, annular plaques with erythematous to violet elevated borders and central pallor were identified on the dorsal side of both upper extremities and on the upper third of the patient's back. Some of the plaques merged creating a polycyclic pattern, mainly on both forearms, left upper arm and back (see Figure 1). The patient described having experienced the same skin changes the year before in the Dominican Republic, which had a self‐limiting course with completed healing after some weeks. These clinical findings correlated well with a subacute cutaneous lupus erythematosus (SCLE), probably triggered by solar exposure.
Annular plaques with a polycyclic pattern and erythematous to violet elevated borders and central pallor on both upper extremities (above) and on the back (below).
Additionally, 1–4 mm erythematous cocarde‐like papules with central blistering were found on the patient's chest and middle abdominal area, extending symmetrically to both sides (see Figure 2). The patient also reported having had those skin efflorescences on both palms and soles, as well as on the bearded areas of his cheeks during his vacation. A 3 mm × 4 mm scab was located on the lateral side of the lower lip. According to the patient, small vesicles and afterwards an ulcer appeared on the area at the beginning of his trip. This constellation supports the diagnosis of an erythema exudativum multiforme (EEM) induced by a herpes simplex virus infection.
Symmetric erythematous cocarde‐like papules with central blistering on the abdominal area.
Three well‐defined patches with diffuse thinning of the hair were located on the parieto‐occipital area of the scalp. The patient remembered noticing these plaques about 1 month ago. Due to previous medical history and good response to topical corticosteroids, this relapsing stress‐associated hair loss was compatible with alopecia areata.
Blood tests showed leucopenia, elevated liver enzymes, elevated C‐reactive protein (CRP), positive rheumatoid factor, high titres of speckled pattern antinuclear antibodies (ANA) (1:2.560) and positive anti‐SSA/Ro, anti‐SSB/La, anti‐U1‐RNP and antiphospholipid antibodies (lupus anticoagulant, anti‐cardiolipin antibody and anti‐β2‐glycoprotein‐I antibody). Anti‐dsDNA and anti‐Sm were negative. Regarding serologic testing, IgG antibodies against HSV‐1 were detected.
Skin biopsies of two affected areas (abdominal area and right posterior forearm) displayed characteristic histological findings of erythema multiforme (vacuolar degeneration of the epidermis with destruction of the basal membrane, lichenoid inflammation with dense lymphocytic infiltrate and apoptotic keratinocytes; see Figure 3) and subacute cutaneous lupus erythematosus (hyperorthokeratosis, interface‐dermatitis with vacuolisation of the basal layer of the epidermis, dyskeratotic keratinocytes, dense lymphotic infiltrate and mucin deposition within connective tissue; see Figure 4), confirming the diagnosis of a Rowell Syndrome.
Skin biopsy—histology of erythema exudativum multiforme. Vacuolisation of the epidermis (green arrows), destruction of the basal membrane (yellow asterisk), lichenoid inflammation with lymphocytic infiltrate (blue asterisk) and apoptotic keratinocytes (blue circle).
Skin biopsy—histology of subacute cutaneous lupus erythematosus. Hyperorthokeratosis (purple asterisk), interface dermatitis with dense lymphocytic infiltration (red asteriscs), vacuolar degeneration of the basal layer (green arrows), dyskeratotic keratinocytes (orange circles), subcutaneous mucine deposition (blue asterisk).
Our patient was initially treated symptomatically with topical triamcinolone acetonide 0.1% (twice daily for 1 week, once daily for 1 week) followed by topical pimecrolimus (once daily for 2 weeks). A combination of topical minoxidil and betamethasone was applied on the alopecia patches on the scalp. The use of sunscreen was advised. After completing the treatment, all skin lesions were healed without scarring. A slight hypopigmentation was identified on the forearms. Two months later, early signs of hair regrowth were visible on the alopecic plaques without signs of scarring. A new blood test 4 weeks after the first consultation showed a correction of the leucopenia, a reduction of CRP and a reduction of the liver enzymes.
A score of 15 on the 2019 EULAR/ACR classification criteria for systemic lupus erythematosus (SLE) was achieved, increasing the likelihood of a SLE. The patient was referred to his family doctor for an hepatic ultrasound and monitoring of cardiovascular factors. A participation in general screening programs was recommended, including skin cancer screening, colorectal cancer screening and PSA‐test. Further examinations were conducted by the rheumatologists, due to joint pain described by the patient.
Rowell Syndrome1 is a rare entity combining EEM and lupus erythematosus (LE).2, 3, 4, 5, 6, 7, 8 Zeitouni et al. redefined Rowell Syndrome's diagnostic criteria.2 Major criteria include: (1) LE (systemic, discoid or subacute cutaneous), (2) EEM‐like skin lesions and (3) speckled pattern of ANA antibodies. Minor criteria comprise: (1) chilblains, (2) positive anti‐SSA/Ro or anti‐SSB/La antibodies and (3) positive rheumatoid factor. The diagnosis is achieved when all major criteria and at least one minor criterion are present.2, 3, 4, 5, 6, 7, 8 Prognosis and treatment regimens are those of EEM and LE,8 with reported good response to oral cortisone, azathioprine, cyclosporine, dapsone, antimalarials8 and methotrexate.9
CONFLICT OF INTEREST STATEMENT
None to declare.
AUTHOR CONTRIBUTIONS
Ariana Palacio: Conceptualization (lead); data curation (lead); formal analysis (lead); investigation (lead); methodology (lead); project administration (lead); writing – original draft (lead); writing – review & editing (lead). Karla Medrano Cebrian: Validation (supporting). Michael Majores: Formal analysis (supporting). Manfred Uerlich: Formal analysis (supporting). Erhard Bierhoff: Formal analysis (supporting). Sonja Bonness: Validation (supporting). Uwe Reinhold: Validation (supporting).
ETHICS STATEMENT
The patients in this manuscript have given written informed consent to publication of their case details.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Rowell NR , Beck JS , Anderson JR . Lupus erythematosus and erythema multiforme‐like lesions. A syndrome with characteristic immunological abnormalities. Arch Dermatol 1963;88(2):176–180. 10.1001/archderm.1963.01590200064012 14043605 · doi ↗ · pubmed ↗
- 2Zeitouni NC , Funaro D , Cloutier RA , Gagné E , Claveau J . Redefining Rowell's syndrome. Br J Dermatol. 2000;142(2):343–346. 10.1046/j.1365-2133.2000.03306.x 10730772 · doi ↗ · pubmed ↗
- 3Gallo L , Megna M , Festa B , Stellato P , di Pinto R , Fabbrocini G , et al. Rowell syndrome: a diagnostic Challenge. J Clin Aesthet Dermatol. 2020;13(4):40–42.PMC 760539033144910 · pubmed ↗
- 4Duarte AF , Mota A , Pereira M , Baudrier T , Azevedo F . Rowell syndrome ‐ case report and review of the literature. Dermatol Online J. 2008;14(3):15. 10.5070/d 32sv 231h 1 18627716 · doi ↗ · pubmed ↗
- 5Aldousari HFA , Aldaihani D , Al‐Mutairi NBSN . Rowell syndrome. Postepy Dermatol Alergol. 2023;40(4):577–580. 10.5114/ada.2023.130514 37692268 PMC 10485764 · doi ↗ · pubmed ↗
- 6Lee D , Waseh S , Motaparthi K , Hsu S . Rowell syndrome in a middle‐aged woman: a case report. Cureus. 2023;15(5). 10.7759/cureus.39631 PMC 1030550937388608 · doi ↗ · pubmed ↗
- 7Sethy M , Padhan P , Abirami C , Maikap D . Rowell's syndrome: a case report and literature overview. Indian Dermatol Online J. 2021;12(4):608–610. 10.4103/idoj.idoj_554_20 34430473 PMC 8354387 · doi ↗ · pubmed ↗
- 8Lee A , Batra P , Furer V , Cheung W , Wang N , Franks A, Jr . Rowell syndrome (systemic lupus erythematosus + erythema multiforme). Dermatol Online J 2009;15(8):1. 10.5070/d 35pf 8k 3r 2 19891909 · doi ↗ · pubmed ↗