Is mesh pore size in polypropylene meshes associated with the outcome in Lichtenstein inguinal hernia repair: a registry-based analysis of 22,141 patients
H. C. Albrecht, M. Trawa, F. Köckerling, D. Adolf, M. Hukauf, H. Riediger, S. Gretschel

TL;DR
This study analyzed 22,141 patients to determine if mesh pore size affects outcomes in inguinal hernia repair, finding no significant differences in most outcomes.
Contribution
The study provides clinical evidence on the association between mesh pore size and hernia repair outcomes using a large registry-based dataset.
Findings
No association was found between mesh pore size and intraoperative or postoperative complications.
Small-pore meshes showed a tendency for lower complication-related reoperation risk.
Small-pore meshes were linked to reduced pain at rest and on exertion after one year.
Abstract
Experimental data show that large-pored meshes reduce foreign body reaction, inflammation and scar bridging and thus improve mesh integration. However, clinical data on the effect of mesh porosity on the outcome of hernioplasty are limited. This study investigated the relation of pore size in polypropylene meshes to the outcome of Lichtenstein inguinal hernioplasty using data from the Herniamed registry. This analysis of data from the Herniamed registry evaluated perioperative and 1-year follow-up outcomes in patients undergoing elective, primary, unilateral Lichtenstein inguinal hernia repair using polypropylene meshes. Patients operated with a non-polypropylene mesh or a polypropylene mesh with absorbable components were excluded. Polypropylene meshes with a pore size of 1.0 × 1.0 mm or less were defined as small-pored meshes, while a pore size of more than 1.0 × 1.0 mm was…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
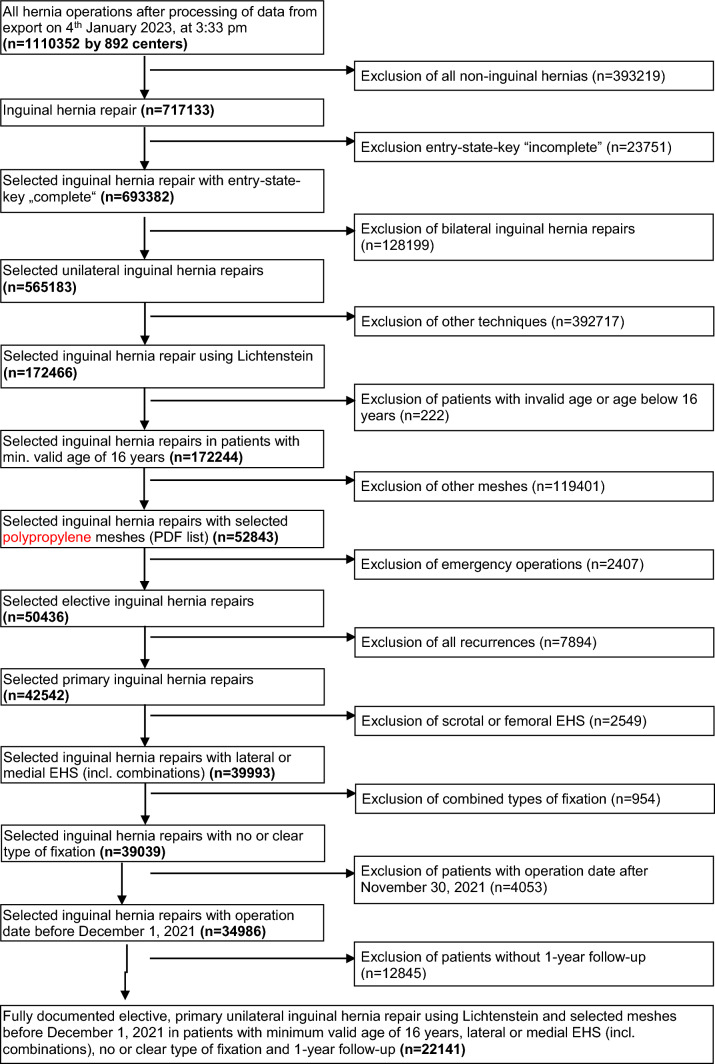 Figure 1
Figure 1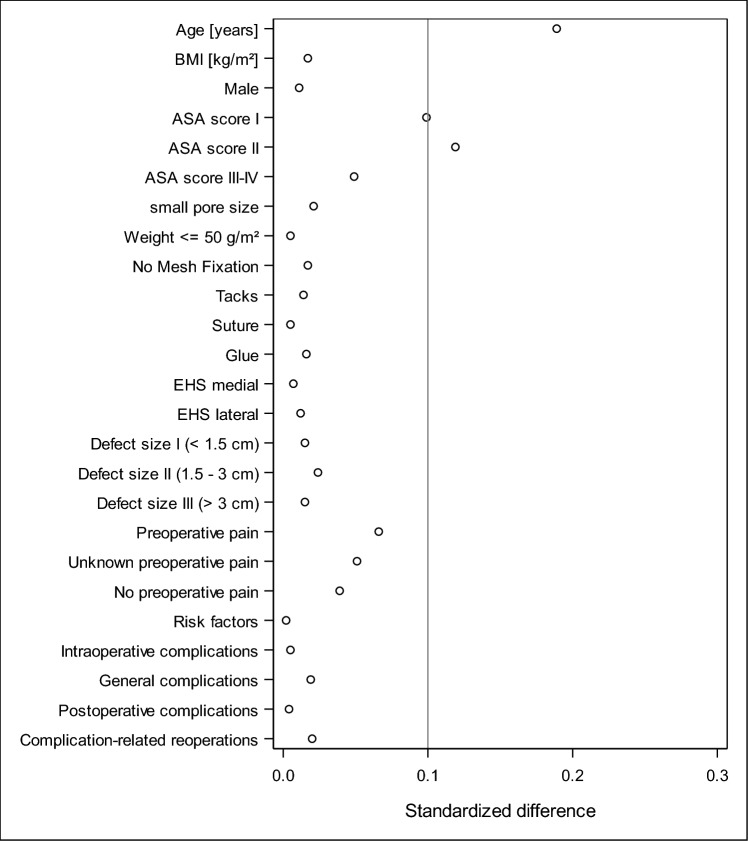 Figure 2
Figure 2- —Medizinische Hochschule Brandenburg CAMPUS GmbH (5634)
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsHernia repair and management · Pelvic and Acetabular Injuries · Abdominal Surgery and Complications
Introduction
Inguinal hernioplasty is one of the most frequently performed surgical procedures in which synthetic mesh implants are nowadays used for standard repair, as recurrence rates are significantly lower compared to non-mesh repair [1]. However, several complications have been associated with mesh repairs, most commonly chronic postoperative inguinal pain (CPIP), which can occur in up to 50% of patients [2, 3]. Due to its frequency, this complication has a significant impact on patients’ quality of life [2]. Furthermore, mesh implants have been assumed to affect the spermatic cord structures and, in rare cases, cause dysejaculation, sexual pain, and orchialgia [4–6].
However, potential complications after mesh repair are influenced by several factors, among which surgical technique and mesh material parameters are considered relevant [7, 8].
Synthetic mesh implants differ in terms of raw material, mechanical and structural parameters [5]. In the latter, mesh weight and porosity are in focus with regard to biocompatibility and outcomes after inguinal hernioplasty.
The postulated advantage of light weight meshes (<50 g/m^2^) with regard to CPIP [3, 9–12] due to lower foreign body reactions, inflammation and fibrosis could not be consistently confirmed in all studies [13–15]. However, since the mesh weight depends significantly on specific density of the polymer, it is not considered the only relevant predictor for tissue reaction [7, 8, 13]. Several studies have shown that porosity is instead an even more important factor for the biocompatibility of synthetic meshes. Large pores (>1 mm) improve tissue ingrowth by reducing inflammatory infiltration, connective tissue and scar bridging [8, 16, 17]. The extent to what these findings transfer to the results of inguinal hernioplasty, both in studies and in everyday clinical practice, is still controversial [2, 9, 14].
The aim of this study was to investigate the association of pore size in polypropylene meshes with the outcome of Lichtenstein inguinal hernioplasty using data from the Herniamed registry.
Patients and methods
Herniamed is an internet-based hernia registry in which hospitals and independent surgeons in Germany, Austria and Switzerland can voluntarily enter data on their routine hernia operations [18, 19]. A contract is concluded with each participating hospital and each participating surgeon, in which the latter two parties undertake to enter all data on hernia repairs completely and correctly in the Herniamed register. For routine procedures, surgeons choose one of the meshes available on the market.
However, in order for a patient to be included in the Herniamed registry, the patient must sign a special declaration of consent in which the patient agrees to the data documentation and follow-up by the treating hospital or surgeon. If this special declaration of consent is not available, the patient may not be included in the Herniamed registry. As part of the information patients receive about participating in the Herniamed registry, they are also encouraged to inform the treating hospital or surgeon of any problems or complications that occur after hernia surgery.
If problems or complications arise after the operation, the patient can contact the treating hospital or surgeon at any time and request a clinical examination [18, 19]. All intra- and postoperative complications as well as complication-related reoperations are recorded up to 30 days after the operation. After 1, 5 and 10 years, all patients and their general practitioner receive a questionnaire from the hospital or the treating surgeon in which they are asked about pain at rest, pain on exertion, chronic pain requiring treatment, protrusions in the groin area or recurrence. Patients are also asked again whether any postoperative complications have occurred. If the patient or the general practitioner reports a relevant finding, the patient may be requested to attend for further diagnostic examination [18, 19]. Haapaniemi et al. [20] showed that participation in the registry and follow-up by questionnaire and selective physical examination provide a solid basis for quality control.
Data from the Herniamed database collected prospectively between January 5, 2009 and December 1, 2021 were used for the analysis. Inclusion criteria were an age of 16 years or older and an elective, primary, unilateral Lichtenstein inguinal hernia repair performed with one of the selected polypropylene meshes (Table 1) by November 30, 2021. Non-polypropylene meshes and polypropylene meshes with absorbable components were excluded.Table 1. Polypropylene meshes used for Lichtenstein repairMeshSmall pore (≤ 1.0 × 1.0 mm)n%Large pore (> 1.0 × 1.0 mm)n%Optilene LP 36 g/m^2^; 1.0 × 1.0 mm414060.41DynaMesh-LICHTENSTEIN 68 g/m^2^; 2.6 × 2.6 mm365123.88Prolene 76 g/m^2^; 1.0 × 1.0 mm116216.96Optilene mesh 60 g/m^2^ 1.5 × 1.5 mm251816.47TiMesh Light 35 g/m^2^; 1.0 × 1.0 mm105015.32Dynamesh Endolap 78 g/m^2^; 2.6 × 2.6 mm192212.57Premilene 82 g/m^2^; 0.8 × 0.8 mm3254.74Bard Soft mesh 42 g/m^2^; 6.29 × 6.29 mm191812.55TiMesh strong 65 g/m^2^; 1.0 × 1.0 mm901.31Parietene Standard 88 g/m^2^; 2.0 × 2.6 mm167710.97TiMesh extra light 16 g/m^2^; 1.0 × 1.0 mm570.83Dynamesh PP standard 70 g/m^2^; 1.6 × 1.6 mm8315.443D Max Mesh 104.5 g/m^2^; 0.55 × 0.55 mm290.42Optilene Mesh elastic 48 g/m^2^; 3.6 × 2.8 mm8135.32Dynamesh PP light 37 g/m^2^; 2.4 × 2.4 mm7594.96Parietene makroporös 46/m^2^; 2.8 × 2.5 mm6254.09TiO2Mesh 47 g/m^2^; 2.8 × 2.8 mm2921.91Tilene blue 24 g/m^2^; 3.0 × 3.0 mm2431.593D Max Light Mesh 42 g/m^2^; 6.29 × 6.29 mm360.24Parietene light 36/m^2^; 1.6 × 1.5 mm30.02Total6853100.0015,288100.00
The polypropylene meshes with a pore size of 1.0 × 1.0 mm or less were defined as small-pore meshes. Accordingly, meshes with a pore size of more than 1.0 × 1.0 mm were considered large pored.
Exclusion criteria were incomplete documentation (e.g., missing age, weight, and duration of surgery), follow-up examinations outside the specified time period and data from the deactivated centers which could not be followed up before deactivation. In addition, femoral and scrotal hernias and operations with combined mesh fixation methods (e.g., staple and adhesive) were excluded. In addition, patients operated with non-polypropylene meshes or polypropylene meshes with absorbable components were excluded.
After plausibility and inclusion criteria were checked, the data were first examined univariately for differences between the pore size groups with regard to all patient and surgical characteristics and outcome parameters. Finally, binary logistic regression models were created for all outcome parameters with all potential influencing factors. The binary variables general, intra- or postoperative complications or a risk factor were deemed present each as soon as at least one corresponding single item was present.
In the univariate analysis, the small- and large-pore groups were compared with each other. All categorical patient data were presented as absolute and relative frequencies for these categories in contingency tables and tested via Chi-square test. For continuous parameters, mean and standard deviation were presented and the robust t-test (Satterthwaite) was used for normally distributed data.
The association of patient and surgical characteristics with the outcome parameters (general, intra- and postoperative complications, complication-related reoperations, recurrences as well as pain at rest, pain on exertion and pain requiring treatment after 1 year) was investigated using the binary logistic regression model.
All analyses were performed using SAS 9.4 software (SAS Institute Inc., Cary, NC, USA) and are deliberately considered at the full significance level of 5%, i.e., no correction is made for multiple testing.
Results
Between January 2009 and January 2023, 1,110,352 patient records were prospectively enrolled in the Herniamed registry. The data of 22,141 patients were included in the present study with regard to inclusion criteria, plausibility and completeness of follow-up (Fig. 1).Fig. 1. Flowchart of patient inclusion
Of the latter, 6853 patients (31%) were operated on with a small-pore mesh and 15,288 patients (69%) with a large-pore mesh in Lichtenstein repair.
Non-adjusted analyses
With regard to patient and surgical characteristics, there were significant differences between the small- and large-pore polypropylene meshes for most parameters (Table 2). For example, the patients in whom a large-pored mesh was used were older and had a higher proportion of heavyweight meshes. In addition, these patients had a higher proportion of ASA III/IV, risk factors, preoperative pain, larger defects and use of sutures.Table 2. Non-adjusted analysis of patient and surgical characteristicsPore sizepSmallLargen%n%Age [years] N/[mean ± SD]6853/67.7 ± 13.715,288/68.6 ± 13.4 < 0.001BMI [kg/m^2^] N/[mean ± SD]6830/25.7 ± 3.515,237/25.9 ± 3.7 < 0.001Mesh weigh≤ 50 g/m^2^524776.6468930.7 < 0.00 > 50 g/m^2^160623.410,59969.3SexMale607188.613,94391.2 < 0.001Female78211.413458.8ASAI106115.5208813.7 < 0.001II389656.9802952.5III/IV189627.7517133.8Preoperative painNo212631.0450729.5 < 0.001Yes382255.8957262.6Unknown90513.212097.9Defect size (inguinal)I (< 1.5 cm)82612.114579.5 < 0.001II (1.5–3 cm)412960.3820053.6III (> 3 cm)189827.7563136.8EHS classification (inguinal)Medial198228.9445329.10.473Lateral331848.4727747.6Combined155322.7355823.3FixationNo mesh fixation1071.62341.5 < 0.001Tacks110.2330.2Suture646894.414,92997.7Glue2673.9920.6Risk factors—totalYes264238.6632541.4 < 0.001No421161.4896358.6COPDYes6339.211957.8 < 0.001No622090.814,09392.2DiabetesYes6399.314009.20.691No621490.713,88890.8Aortic aneurysmYes540.81691.10.029No679999.215,11998.9ImmunosuppressionYes741.11721.10.767No677998.915,11698.9CorticoidsYes811.22231.50.102No677298.815,06598.5SmokingYes6118.913228.60.513No624291.113,96691.4CoagulopathyYes1732.55153.4 <0 .001No668097.514,77396.6Antithrombotic medicationYes97814.3266917.5 < 0.001No587585.712,61982.5Anticoagulant medicationYes3585.28945.80.063No649594.814,39494.2
The relation of the pore sizes of the meshes to the intraoperative, general and postoperative complications, complication-related reoperations, recurrences as well as pain at rest, exertion and pain requiring treatment in the 1-year follow-up is shown in Table 3.Table 3. Non-adjusted analysis of perioperative complications and 1-year follow-up dataPore sizepSmallLargen%n%Intraoperative complications—totalYes480.71060.70.953No680599.315,18299.3General complications—totalYes1101.62101.40.182No674398.415,07898.6Postoperative complications—totalYes2714.05783.80.534No658296.014,71096.2Complication-related reoperationsYes771.12251.50.039No677698.915,06398.5Recurrence on 1-year follow-upYes650.91390.90.777No678899.115,14999.1Pain on exertion on 1-year follow-upYes6519.5161410.60.016No620290.513,67489.4Pain at rest on 1-year follow-upYes3455.08745.70.040No650895.014,41494.3Pain requiring treatment on 1-year follow-upYes1882.74723.10.164No666597.314,81696.9
In the unadjusted analysis, there was a significant disadvantage for patients in whom large-pored meshes were used in terms of complication-related reoperations as well as rest pain and pain on exertion in the 1-year follow-up.
Multivariable analyses
The risk of intraoperative complications was associated with defect size (p=0.003), mesh fixation (p = 0.003) and ASA classification (p = 0.058) (Table 4). The results showed a lower complication rate for suture vs. glue fixation.Table 4. Multivariable analysis for intraoperative complicationsVariablep-valueCategoriesOdds ratioLCLUCLp-value (pair-wise)Defect size0.003III (> 3 cm) vs II (1.5–3 cm)1.8401.2942.616 < 0.001II (1.5–3 cm) vs I (< 1.5 cm)0.7270.4201.2590.255III (> 3 cm) vs I (< 1.5 cm)1.3380.7602.3550.313Fixation0.003Suture vs glue0.2590.1270.530 < 0.001No mesh fixation vs glue0.3550.0941.3450.127No mesh fixation vs suture1.3690.4334.3280.593Tacks vs glue*–––0.977No mesh fixation vs tacks*–––0.979Suture vs tacks*–––0.979ASA0.058III/IV vs II1.5151.0382.2090.031II vs I0.7020.4241.1630.169III/IV vs I1.0640.5981.8910.833BMI [5-point OR]0.1391.1680.9511.435Preoperative pain0.391Unknown vs no0.6450.3261.2750.207Yes vs no0.8540.6061.2030.366Yes vs unknown1.3240.6852.5600.403Sex0.625Female vs male0.8610.4731.568EHS classification0.650Medial vs lateral0.8320.5641.2290.356Medial vs combined0.8770.5631.3670.562Lateral vs combined1.0540.7051.5750.799Age [10-year OR]0.6801.0300.8951.186Risk factors0.843Yes vs no0.9650.6801.371Mesh weight0.887≤ 50 g/m^2^ vs > 50 g/m^2^1.0260.7191.466Pore size0.993Small vs large0.9980.6771.473LCL lower confidence limit, UCL upper confidence limit* No valid information available as categories are not sufficiently populated
The risk of general complications was significantly increased with high ASA classification (p<0.001), older age (p = 0.004) and the presence of risk factors (p = 0.038) (Table 5).Table 5. Multivariable analysis for general complicationsVariablep-valueCategoriesOdds ratioLCLUCLp-value (pair-wise)ASA < 0.001III/IV vs II1.9431.5012.515 < 0.001III/IV vs I1.5420.9832.4200.060II vs I0.7940.5221.2070.279Age [10-year OR]0.0041.1721.0521.307Risk factors0.038Yes vs no1.2921.0151.645Mesh weight0.138≤ 50 g/m^2^ vs > 50 g/m^2^1.2040.9421.539Defect size0.154III (> 3 cm) vs II (1.5–3 cm)1.2470.9801.5860.073III (> 3 cm) vs I (< 1.5 cm)1.3470.8552.1220.199II (1.5–3 cm) vs I (< 1.5 cm)1.0800.6981.6730.729Pore size0.241Small vs large1.1690.9001.518EHS classification0.666Lateral vs combined0.8850.6711.1680.387Medial vs combined0.8980.6641.2140.484Medial vs lateral1.0150.7741.3300.915BMI [5-point OR]0.7411.0270.8781.200Preoperative pain0.821YES vs no1.0850.8401.4000.532Unknown vs no1.0450.6821.6010.841Yes vs unknown1.0380.6991.5430.852Fixation0.973No mesh fixation vs tacks0.6130.0675.6430.666No mesh fixation vs suture0.8280.3062.2380.710No mesh fixation vs glue0.8130.2252.9360.752Suture vs tacks0.7410.1015.4220.768Tacks vs glue1.3250.15411.3730.797Suture vs glue0.9820.4282.2500.965Sex0.989Female vs male1.0030.6821.475LCL lower confidence limit, UCL upper confidence limit
A similar relation was found for postoperative complications. Furthermore, preoperative pain compared to unknown pain status (p = 0.003), large hernia defect (p = 0.013), lightweight mesh (p = 0.013), female gender (p = 0.010) and high BMI (p = 0.027) were identified as being related to a higher risk for postoperative complications (Table 6). However, a medial EHS classification was associated with a lower complication rate compared to a lateral classification.Table 6. Multivariable analysis for postoperative complicationsVariablep-valueCategoriesOdds ratioLCLUCLp-value (pair-wise)ASA < 0.001III/IV vs II1.4191.2111.663 < 0.001III/IV vs I1.6391.2232.196 < 0.001II vs I1.1550.8841.5080.291Age [10-year OR] < 0.0011.1221.0511.198Risk factors < 0.001Yes vs no1.2881.1101.496Preoperative pain0.003Yes vs unknown1.6961.2552.292 < 0.001Unknown vs no0.6130.4480.8410.002Yes vs no1.0400.8911.2150.615Sex0.010Female vs male1.3291.0691.652Defect size0.013III (> 3 cm) vs II (1.5–3 cm)1.2471.0711.4510.004III (> 3 cm) vs I (< 1.5 cm)1.2740.9721.6710.080II (1.5–3 cm) vs I (< 1.5 cm)1.0220.7891.3220.870Mesh weight0.013≤ 50 g/m^2^ vs > 50 g/m^2^1.2131.0411.413BMI [5-point OR]0.0271.1111.0121.220EHS classification0.091Medial vs lateral0.8330.7030.9860.033Lateral vs combined1.1170.9351.3340.224Medial vs combined0.9300.7631.1330.471Fixation0.375No mesh fixation vs glue0.4540.1861.1090.083No mesh fixation vs suture0.5360.2521.1380.105No mesh fixation vs tacks0.5160.1032.5780.420Suture vs glue0.8470.5191.3830.507Tacks vs glue0.8810.1963.9600.868Suture vs tacks0.9620.2314.0020.958Pore size0.552Small vs large1.0510.8911.240LCL lower confidence limit, UCL upper confidence limit
No significant relation could be demonstrated between pore size and either intraoperative, general or postoperative complications.
The risk of complication-related reoperation was significantly associated with ASA classification (p = 0.002), age (p = 0.013), the presence of risk factors (p = 0.036) and tended to be associated with EHS classification (p = 0.062), preoperative pain (p = 0.066), pore size (p = 0.086) and mesh weight (p = 0.087). Accordingly, a higher ASA, a higher age, the presence of at least one risk factor, preoperative pain and low weight mesh were associated with a higher risk of reoperation. On the other hand, medial EHS classifications and smaller pore size (OR = 0.778 [0.585; 1.036]) were associated with a lower complication-related reoperation rate (Table 7).Table 7. Multivariable analysis for complication-related reoperationsVariablep-valueCategoriesOdds ratioLCLUCLp-value (pair-wise)ASA0.002III/IV vs II1.5971.2292.075 < 0.001III/IV vs I1.6591.0172.7070.043II vs I1.0390.6601.6350.868Age [10-year OR]0.0131.1511.0301.286Risk factors0.036Yes vs no1.3031.0171.669EHS classification0.062Medial vs combined0.6860.4950.9500.023Medial vs lateral0.7560.5641.0140.062Lateral vs combined0.9070.6861.1980.492Preoperative pain0.066Yes vs no1.2770.9761.6710.075Yes vs unknown1.5320.9522.4660.079Unknown vs no0.8330.5011.3870.483Pore size0.086Small vs large0.7780.5851.036Mesh weight0.087≤ 50 g/m^2^ vs > 50 g/m^2^1.2430.9691.595Sex0.274Female vs male1.2310.8491.785BMI [5-point OR]0.2791.0900.9331.274Fixation0.311Tacks vs glue6.8330.92750.3470.059Suture vs tacks0.3530.0841.4780.154Suture vs glue2.4140.5939.8260.219No mesh fixation vs tacks < 0.001 < 0.001 > 999.9990.962No mesh fixation vs suture < 0.001 < 0.001 > 999.9990.965No mesh fixation vs glue < 0.001 < 0.001 > 999.9990.967Defect size0.510III (> 3 cm) vs II (1.5–3 cm)1.1400.8881.4640.303III (> 3 cm) vs I (< 1.5 cm)1.2260.7691.9540.392II (1.5–3 cm) vs I (< 1.5 cm)1.0750.6881.6790.751LCL lower confidence limit, UCL upper confidence limit
No association between pore size and recurrence was found at 1-year follow-up.
However, it was shown that medial EHS classifications (p < 0.001), female gender (p < 0.001), higher BMI (p = 0.004) and higher ASA (p = 0.038) were associated with a higher risk of recurrence. On the other hand, older age (p = 0.041) was associated with a lower risk of recurrence (Table 8).Table 8. Multivariable analysis for recurrence at 1-year follow-upVariablep-valueCategoriesOdds ratioLCLUCLp-value (pair-wise)EHS classification < 0.001Medial vs lateral2.2971.6693.163 < 0.001Medial vs combined1.5541.0792.2390.018Lateral vs combined0.6760.4581.0000.050Sex < 0.001Female vs male1.9151.3082.803BMI [5-point OR]0.0041.2791.0831.509ASA0.038III/IV vs I1.9451.1273.3560.017III/IV vs II1.3961.0061.9370.046II vs I1.3940.8672.2390.170Age [10-year OR]0.0410.8880.7920.995Preoperative pain0.147Yes vs no0.7410.5491.0000.050Unknown vs no0.8360.5061.3800.483Yes vs unknown0.8870.5471.4370.625Defect size0.203III (> 3 cm) vs I (< 1.5 cm)0.6770.4141.1080.120III (> 3 cm) vs II (1.5–3 cm)0.7830.5691.0780.133II (1.5–3 cm) vs I (< 1.5 cm)0.8640.5541.3490.521Mesh weight0.217≤ 50 g/m^2^ vs > 50 g/m^2^0.8200.5981.124Fixation0.467No mesh fixation vs tacks0.1360.0082.2300.162No mesh fixation vs glue0.2240.0261.9390.174No mesh fixation vs suture0.3120.0442.2400.247Suture vs tacks0.4340.0593.2050.413Suture vs glue0.7160.2881.7800.472Tacks vs glue1.6480.18514.6850.654Risk factors0.577Yes vs no0.9170.6781.242Pore size0.580Small vs large1.0990.7861.537LCL lower confidence limit, UCL upper confidence limit
The 1-year follow-up showed that older age (p < 0.001), larger defects (p < 0.001) and small-pore meshes (OR = 0.851 [0.737; 0.985]; p = 0.029) were associated with a lower risk of pain at rest (OR = 0.851 [0.737; 0.983]). In contrast, preoperative pain, postoperative complications, medial EHS classifications, greater BMI, female gender (each p < 0.001), and higher ASA classification (p = 0.001) were associated with an increased risk of pain at rest (Table 9).Table 9. Multivariable analysis for pain at rest at 1-year follow-upVariablep-valueCategoriesOdds ratioLCLUCLp-value (pair-wise)Age [10-year OR] < 0.0010.7910.7560.828Preoperative pain < 0.001Yes vs no1.6311.4111.886 < 0.001Unknown vs no1.6161.2962.015 < 0.001Yes vs unknown1.0100.8311.2270.923Sex < 0.001Female vs male1.6881.4242.000Defect size < 0.001III (> 3 cm) vs II (1.5–3 cm)0.6760.5870.778 < 0.001III (> 3 cm) vs I (< 1.5 cm)0.5900.4810.725 < 0.001II (1.5–3 cm) vs I (< 1.5 cm)0.8740.7311.0440.137Postoperative complications < 0.001Yes vs no1.6511.2742.140EHS classification < 0.001Medial vs lateral1.2931.1321.478 < 0.001Medial vs combined1.2711.0771.4990.005Lateral vs combined0.9820.8371.1520.826BMI [5-point OR] < 0.0011.1441.0621.233ASA0.001II vs I1.4161.1741.708 < 0.001III/IV vs I1.4171.1301.7780.003III/IV vs II1.0010.8661.1570.990Pore size0.029Small vs large0.8510.7370.983Mesh weight0.271≤ 50 g/m^2^ vs > 50 g/m^2^0.9290.8151.059Risk factors0.379Yes vs no1.0590.9321.203Fixation0.894No mesh fixation vs glue0.7730.3971.5030.448Suture vs glue0.8770.5571.3810.571No mesh fixation vs suture0.8810.5371.4450.616Tacks vs glue0.7770.1743.4720.742Suture vs tacks1.1280.2704.7080.869No mesh fixation vs tacks0.9940.2204.4980.994LCL lower confidence limit, UCL upper confidence limit
In regard to pore size, this result (OR = 0.851) would correspond to pain at rest at follow-up in 51 out of 1000 operations with small-pore size meshes compared to 59 out of 1000 operations with large-pore size meshes (prevalence 5.51%).
A similar relation was confirmed in the 1-year follow-up analysis for pain on exertion.
Again, older age, larger defects and small-pored meshes (OR = 0.815 [0.731; 0.909]) were associated with a lower risk of pain on exertion (p < 0.001 each). Preoperative pain, higher BMI, postoperative complications, female gender and medial EHS classifications were associated with a higher risk of pain on exertion (p < 0.001 each) (Table 10).Table 10. Multivariable analysis for pain at exertion at 1-year follow-upVariablep-valueCategoriesOdds ratioLCLUCLp-value (pair-wise)Age [10-year OR] < 0.0010.7230.6990.748Sex < 0.001Female vs male1.6751.4661.915Preoperative pain < 0.001Yes vs no1.5271.3731.699 < 0.001Unknown vs no1.4211.2001.682 < 0.001Yes vs unknown1.0750.9231.2520.353Defect size < 0.001III (> 3 cm) vs II (1.5–3 cm)0.6990.6280.778 < 0.001III (> 3 cm) vs I (< 1.5 cm)0.5960.5110.696 < 0.001II (1.5–3 cm) vs I (< 1.5 cm)0.8530.7450.9760.021BMI [5-point OR] < 0.0011.1651.1001.234Postoperative complications < 0.001Yes vs no1.7011.3872.087EHS classification < 0.001Medial vs lateral1.2661.1441.402 < 0.001Medial vs combined1.2931.1391.468 < 0.001Lateral vs combined1.0210.9041.1540.737Pore size < 0.001Small vs large0.8150.7310.909ASA0.088II vs I1.1461.0051.3060.042III/IV vs II0.9400.8391.0540.292III/IV vs I1.0770.9131.2710.378Fixation0.470No mesh fixation vs suture0.7350.4911.0990.133No mesh fixation vs glue0.6720.3961.1410.141No mesh fixation vs tacks0.7340.2412.2320.586Suture vs glue0.9140.6441.2990.618Tacks vs glue0.9150.3062.7350.874Suture vs tacks0.9990.3532.8240.999Risk factors0.693Yes vs no0.9800.8881.082Mesh weight0.729≤ 50 g/m^2^ vs > 50 g/m^2^1.0180.9221.123LCL lower confidence limit, UCL upper confidence limit
In terms of pore size, this result (OR = 0.815) would correspond to pain on exertion at follow-up in 93 out of 1000 operations with small-pore meshes compared to 112 out of 1000 operations with large-pore meshes (prevalence 10.24%).
The analysis of the pain requiring treatment at the 1-year follow-up shows that the pore size of the mesh has no significant relation to this outcome variables. Age, gender, defect size, preoperative pain, EHS classification, ASA status, BMI and postoperative complications (each p < 0.001) were significantly associated with pain requiring treatment at 1-year follow-up. Again, older age and larger defects were associated with a lower risk of pain requiring treatment. On the other side, preoperative pain, medial EHS classification, higher ASA classification, higher BMI, female gender and postoperative complications were associated with an increased risk of pain requiring treatment at 1-year follow-up (Table 11).Table 11. Multivariable analysis for pain requiring treatment at 1-year follow-upVariablep-valueCategoriesOdds ratioLCLUCLp-value (pair-wise)Age [10-year OR] < 0.0010.7620.7180.809Sex < 0.001Female vs male2.2091.7952.718Defect size < 0.001III (> 3 cm) vs I (< 1.5 cm)0.4780.3650.626 < 0.001III (> 3 cm) vs II (1.5–3 cm)0.6050.4980.736 < 0.001II (1.5–3 cm) vs I (< 1.5 cm)0.7890.6290.9910.042Preoperative pain < 0.001Yes vs no1.7621.4412.155 < 0.001Unknown vs no1.6601.2252.2500.001Yes vs unknown1.0620.8151.3830.657EHS classification < 0.001Medial vs lateral1.5981.3391.907 < 0.001Medial vs combined1.4061.1281.7520.002Lateral vs combined0.8800.7071.0950.252ASA < 0.001III/IV vs I2.2171.6233.029 < 0.001II vs I1.7281.3272.251 < 0.001III/IV vs II1.2831.0611.5520.010BMI [5-point OR] < 0.0011.2201.1111.340Postoperative complications < 0.001Yes vs no1.7571.2572.455Pore size0.120Small vs large0.8570.7061.041Fixation0.142Suture vs glue0.5840.3520.9710.038No mesh fixation vs suture1.3700.7932.3690.259No mesh fixation vs glue0.8010.3831.6730.555Tacks vs glue*–––0.952No mesh fixation vs tacks*–––0.953Suture vs tacks*–––0.955Mesh weight0.215≤ 50 g/m^2^ vs > 50 g/m^2^0.8940.7491.067Risk factors0.347Yes vs no0.9210.7751.094LCL lower confidence limit, UCL upper confidence limit* No valid information available as categories are not sufficiently populated
Standardized differences of patients with and without follow-up information
Figure 2 shows the results of the standardized differences for patients with (n = 22,141) and without (n = 12,845) follow-up information. Standardized differences above a value of 10% were found only for age and ASA categories. The patients in the analysis population were on average 2.8 years older and had more frequently ASA II classification.Fig. 2. Scatter plot—standardized differences between patient with and without follow-up
Discussion
In order to reduce mesh-related side effects such as foreign body sensation, chronic pain or mesh shrinkage following hernioplasty, research has focused on improving the biocompatibility of meshes. Experimental data show that large-pored meshes reduce foreign body reaction, inflammation and scar bridging and thus improve mesh integration [16, 17, 21, 22]. However, clinical data on the effect of mesh porosity on the outcome of hernioplasty are still limited [2, 3, 14, 25]. This Herniamed registry study evaluates the largest patient cohort (22,141 patients) to date with regard to the relation of mesh porosity in polypropylene meshes to the outcome of Lichtenstein inguinal hernioplasty. However, patient and surgical characteristics differed significantly between the small- and large-pore mesh groups, which is related to the design of the registry study reflecting everyday care rather than selective bias. In general, a higher proportion of patients (69%) were treated with large-pored polypropylene meshes in this study. Furthermore, the patients who had large-pore polypropylene mesh repair were older, had more comorbidities and risk factors, and had larger hernia defects. In addition, a higher proportion of heavyweight meshes (69.3%) was used in large-pore mesh repair. The reason for the apparent preference for large-pored meshes in the treatment of elderly patients and rather difficult hernia situations in everyday care remains speculation. It might reflect the positive characteristics attributed to large-pored meshes from experimental studies.
Chronic postoperative pain as one of the primary outcome measures of inguinal hernia surgery was a main focus of attempts to improve the biocompatibility of meshes.
In this context, large-pored meshes are intended to enable tissue ingrowth, provide better mesh integration, maintain the elasticity of the implant and reduce scar formation [23, 24].
In our study, patients in the large-pore mesh group had a higher risk of both pain at rest and pain on exertion at 1-year follow-up. In contrast, in a randomized clinical trial of 321 patients, O'Dwyer et al. reported less chronic pain but an increase in hernia recurrence in the group treated with large-pore lightweight mesh for inguinal hernia repair at 12-month follow-up [3]. Similarly, in a randomized study of 590 patients who underwent Lichtenstein repair, Bringman et al. described an improvement in pain and discomfort in the group treated with a large-pore lightweight mesh, without affecting the recurrence rate at 3-year follow-up [25]. In both studies, large-pore lightweight meshes were used, while in our study, the majority of patients in the large-pore group received heavyweight meshes. Despite the reported benefits in terms of postoperative pain in the early postoperative course for lightweight meshes, these results are controversial in the literature with regard to the long-term effect [9–12, 15, 26–30].
Krauß et al. reported in a questionnaire study of the Danish Hernia Registry with 1782 patients that large-pore light weight mesh repair does not reduce chronic pain, but increases the recurrence rate compared to small-pore, heavy mesh repair [14]. Consistent with the results of our study, Nikkolo et al. saw more patients with pain in the large-pore mesh group at 3-year follow-up in a randomized trial of 128 patients [2].
Regarding the clinical relevance of our results, it should be noted that even very small differences can be significant due to the relatively large number of cases.
The described differences in postoperative pain between the groups with large-pore and small-pore mesh repair were not found in the analysis of pain requiring treatment at 1-year follow-up in our study.
It is known that the development of chronic postoperative pain after inguinal hernia repair is multifactorial [7]. In our study, in addition to large-pored meshes, younger age, smaller defects, preoperative pain, postoperative complications, medial EHS classifications, higher BMI, and female gender were associated with a higher risk of pain at rest and on exertion. In this context, young age, female gender, preoperative pain and postoperative complications have been identified in previous studies as risk factors for chronic postoperative pain after inguinal hernia repair [31].
Considering the multifactorial genesis and the size of the study population, a cautious conclusion regarding clinical relevance could be that the use of large-pore polypropylene mesh did not improve chronic postoperative pain in our study.
The analysis of the recurrence rate as a primary outcome measure showed no association to the mesh pore size at 1-year follow-up in our study. In contrast, both O'Dwyer et al. and Krauß et al. reported increased recurrence rates after anterior inguinal hernia repair with large-pore lightweight meshes in the above-mentioned studies [3, 14]. Experimental studies have shown that lightweight meshes with a large-pore size may lack structural stability and, therefore, have a tendency for mesh shrinkage [16]. In line with these findings, some studies and meta-analyses reported increased recurrence rates in lightweight mesh inguinal hernia repair with both anterior and laparoendoscopic techniques [30, 32, 33]. However, these results are not consistent in the literature, as further meta-analyses did not confirm increased recurrence rates for open inguinal hernia repair with light weight mesh [10, 11, 34].
In our study, the factors associated with a higher risk of recurrence were medial EHS classifications, female gender, higher BMI and higher ASA score, which is consistent with risk factors reported in the literature [35, 36].
When evaluating intraoperative, general or postoperative complications after Lichtenstein repair, no differences were found between the large-pore and small-pore mesh groups in this study. However, a lower risk of complication-related reoperations was associated with small-pore mesh repair. In the literature to date, there is no data on the influence of mesh porosity on intraoperative or postoperative complications.
Register studies have several limitations, including the present study. The patients enrolled in the registry are heterogeneous, as is the daily practice of hernia surgery. The analysis of register data for certain outcome parameters can, therefore, hardly be performed on heterogeneous groups. In addition, participation in the Herniamed registry is voluntary. Not all hospitals and surgeons in the participating countries include patients in the registry, which could imply a certain bias. Furthermore, a relevant proportion of patients with missing follow-up data could not be included in the analysis of this study. However, standardized differences of more than 10% between the study population and the excluded patients with incomplete follow-up data were only found for age and ASA categories. Therefore, there should only be a limited selection bias in terms of completeness of follow-up. Nevertheless, the follow-up results should be interpreted with caution.
In summary, this Herniamed registry study, investigating the association of mesh porosity in polypropylene meshes to the outcome of Lichtenstein inguinal hernioplasty, found no significant relation between mesh pore size and recurrence rate, intraoperative, general or postoperative complications as well as pain requiring treatment at 1-year follow-up.
Taking into account the potential influence of other patient and surgical characteristics, a significant effect of mesh pore size on complication-related reoperations (tendency), on pain at rest and on pain on exertion was demonstrated at 1-year follow-up.
In general, it should be noted that due to the relatively large number of cases, even very small differences can be significant, but their clinical significance in this context should be interpreted with caution.
In a cautious conclusion regarding clinical relevance, the present study could not demonstrate an advantage of large-pore meshes for the outcome of Lichtenstein inguinal hernioplasty.