An Unusual Case of Syphilis With Pulmonary Involvement
Hadia Arzoun, Fawaz Mohammed, Subha Saeed, Tahir Muhammad Abdullah Khan, Karan Singh

TL;DR
A 26-year-old HIV-positive woman presented with syphilis affecting her lungs, a rare occurrence.
Contribution
This case report highlights the unusual pulmonary involvement in a syphilis patient with an HIV history.
Findings
The patient had syphilis confirmed with pulmonary involvement.
Thoracentesis was performed due to shortness of breath.
The case emphasizes the rare lung manifestation of syphilis.
Abstract
Syphilis can affect multiple organs in the secondary or tertiary stages of the disease. Recent reports have suggested an increase in the incidence of the disease. Involvement of the lung has been rarely described in syphilis. In this report, we discuss the case of a 26-year-old female with past medical history significant for HIV who presented to the hospital with complaints of shortness of breath and underwent thoracentesis; she was found to have syphilis with pulmonary involvement.
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
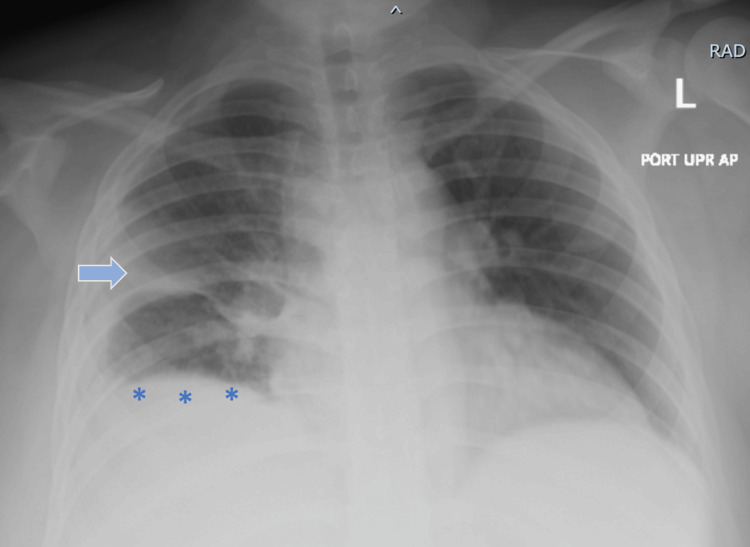 Figure 1
Figure 1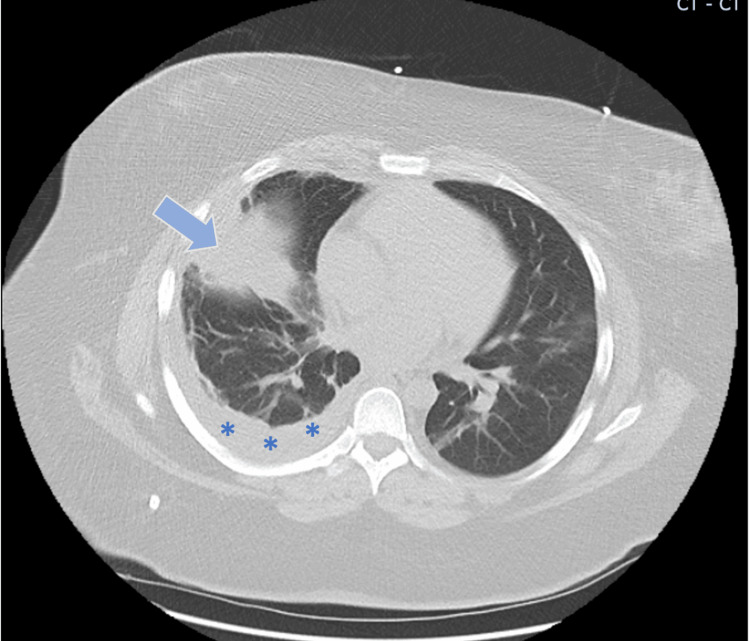 Figure 2
Figure 2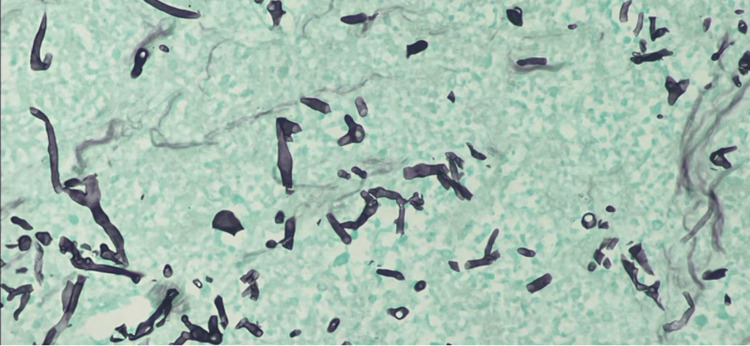 Figure 3
Figure 3| Variables | Patient values | Reference values |
| White blood cell count (k/ul) | 16.7 | 4.8-10.8 |
| Hemoglobin (g/dl) | 9.4 | 12-16 |
| Hematocrit (%) | 31.9 | 34-47 |
| Platelet levels (k/ul) | 556 | 140-440 |
| Variables | Pleural fluid parameters | Reference values |
| Appearance | Dark-amber colored | - |
| Total protein (g/dl) | 4.9 | 1-2 |
| Glucose (mg/dl) | 110 | 90-120 |
| Lactate dehydrogenase (U/L) | 1600 | 40-280 |
| White blood cell count (u/l) | 49 | 0-5 |
| Neutrophils (%) | 1 | 0-100 |
| Lymphocytes (%) | 17 | 0-100 |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsSyphilis Diagnosis and Treatment · Reproductive tract infections research · Body Image and Dysmorphia Studies
Introduction
Syphilis is a sexually transmitted disease, and Treponema pallidum is the organism responsible for it. It is transmitted through sexual contact and manifests with an array of signs and symptoms depending on the stage of the disease. Other routes of infections are infection in utero, blood transfusions, or organ transplantation [1]. The number of infections has dropped drastically since the 1940s thanks to the use of penicillin [1]. The disease course commences with an incubation period ranging from three to six weeks. The disease itself has four stages (primary, secondary, tertiary, latent), with each stage having its distinctive characteristics. Only a handful of cases with pulmonary syphilis have been described in the literature, with the majority of cases reported in the preantibiotic era [2]. Pulmonary involvement was more commonly seen in tertiary and congenital syphilis, although it is more often seen in secondary syphilis after the discovery of antibiotics.
We present a case of a 26-year-old female with past medical history significant for HIV on treatment with bictegravir/emtricitabine/tenofovir alafenamide. She presented to the hospital on account of worsening shortness of breath. Chest imaging showed evidence of a pleural effusion, with pleural fluid cultures subsequently yielding *Treponema pallidum *species.
Case presentation
A 26-year-old female with a recent diagnosis of syphilis who was to commence treatment presented to the hospital with complaints of worsening shortness of breath, fevers, and diarrhea. She denied chest pain, palpitations, nausea, vomiting, or abdominal pain. She also complained of a cough that was non-productive in nature. Her past medical history was significant for HIV and she was on bictegravir/emtricitabine/tenofovir alafenamide. Her recent laboratory values from the outpatient setting showed undetectable HIV RNA with a CD4 count of over 700 (500 to 1500 cells/mm^3^). Blood pressure on presentation was 151/94 mmHg, and she had a heart rate of 109/min. She was found to be hypoxic, requiring supplemental oxygen. The complete blood count at the time of presentation is presented in Table 1.
Chest X-ray showed evidence of a right middle lobe infiltrate and pleural effusion (Figure 1).
Chest X-ray findingsChest X-ray demonstrating right middle lobe infiltrate (blue arrow) and right-sided pleural effusion (asterisks)
For further evaluation, a chest CT was performed, which confirmed the pleural effusion and infiltrate in the right middle lobe (Figure 2). Pulmonology was consulted and a thoracentesis was then performed. Results from pleural fluid studies are presented in Table 2.
Chest CT findingsChest CT with right middle lobe infiltrate (blue arrow) redemonstrated, also confirming the presence of pleural effusion on the right side (asterisks)CT: computed tomography
The pathology report from pleural fluid was positive for Treponema pallidum species on immunohistochemical stain (Figure 3). Infectious disease was consulted and the patient was discharged in stable condition with a planned treatment course of three weeks with intravenous penicillin for syphilis complicated by empyema.
Immunohistochemical stain of pleural fluidImmunohistochemical stain for Treponema pallidum showing multiple spirochetes
Discussion
Our review of the literature has indicated that lung involvement with syphilis is rather rare [1-3]. Other sites less frequently involved include the brain, eye, ear, and gastrointestinal organs [4]. On chest imaging, pulmonary syphilis can present as bilateral infiltrates, single or multiple nodules, or, in rare cases, pleural effusion as seen in our case [5]. A review by Youssef et al. reported co-infection with HIV is seen in about 18% of the patients [6]. These findings coincide with different disease processes often delaying the diagnosis. Therefore, the following criteria proposed by Coleman et al. can be utilized to aid diagnosis: (i) historical and physical findings typical of secondary syphilis; (ii) serologic test results positive for syphilis; (iii) pulmonary abnormalities seen radiographically with or without associated symptoms or signs; (iv) exclusion of other forms of pulmonary disease, when possible, according to findings of serological tests, sputum smears and cultures, and cytological examination of sputum; and (v) response to anti-syphilis therapy [7].
Given that *Treponema pallidum *is difficult to culture, it may be diagnosed with serology [8]. Standard serological testing consists of a non-treponemal test, which is then confirmed with fluorescent treponemal antibody absorptiometry [9]. Clinicians need to be mindful that false-positive treponemal tests are a possibility; these are seen in infections caused by other spirochetes or even malaria [10]. The discrepancy between the nontreponemal and treponemal test may also be observed in patients previously treated for syphilis, in very early or late stages of the disease when the non-treponemal test is essentially non-reactive or in individuals with immunocompromised states who cannot mount an appropriate B-cell response [11-13]. Polymerase chain reaction (PCR) on bronchoalveolar lavage (BAL), pleural fluid, lung biopsy, and immunohistochemistry may also be of benefit to identify the indicated spirochete [6].
Penicillin is the antibiotic of choice for all stages of the disease [14]. One dose of intramuscular benzathine penicillin G 2.4 million units suffices for primary, secondary, and early latent stages of the disease. Three doses of the same are required at weekly intervals in late latent and tertiary syphilis. Doxycycline, a third-generation cephalosporin like ceftriaxone, and ampicillin in combination with probenecid may be used in patients unable to tolerate penicillin [15].
Conclusions
We presented a rare case of syphilis with pulmonary involvement. Clinicians need to be aware of this type of atypical involvement in syphilis. In individuals presenting with airspace disease in the lungs along with pleural involvement, the differential diagnosis is often wide. With epidemiological data suggesting that syphilitic cases are on the rise, a high index of suspicion for pulmonary syphilis should be maintained when investigating the more common causes of such clinical presentations.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Syphilis Principles of Internal Medicine Lukehart AS Fauci AS Braunwald E 4244 Ithaca, NY Cornell University 42011 http://www.accessmedicine.com.elibrary.qatar-weill.cornell.edu/content.aspx
- 2Secondary pulmonary syphilis: report of a likely case and literature review Clin Infect Dis David G Perpoint T Boibieux A 0542200610.1086/49910416392072 · doi ↗ · pubmed ↗
- 3Case report: pulmonary syphilis mimicking pulmonary hematogenous metastases on chest CT and integrated PET/CT Indian J Radiol Imaging Kim HJ Seon HJ Shin HH Choi YD 34372120112143103110.4103/0971-3026.76052 PMC 3056368 · doi ↗ · pubmed ↗
- 4Secondary syphilis: uncommon manifestations of a common disease West J Med Mc Phee SJ 35421401984 https://www.ncbi.nlm.nih.gov/pmc/articles/PMC 1011033/6702190 PMC 1011033 · pubmed ↗
- 5Pulmonary involvement in secondary syphilis Eur J Case Rep Intern Med Benainous R Alunji M Brillet PY Dhote R 24878202110.12890/2021_002487 PMC 833674634377686 · doi ↗ · pubmed ↗
- 6Secondary pulmonary syphilis: case report and review of literature Ann Dermatol Venereol Kassem Youssef H Blind A Chouta Ngaha F Drenou B Nojavan H Michel C 27828714520182946346510.1016/j.annder.2017.11.015 · doi ↗ · pubmed ↗
- 7Secondary syphilis with pulmonary involvement West J Med Coleman DL Mc Phee SJ Ross TF Naughton JL 8758781381983 https://pubmed.ncbi.nlm.nih.gov/6613117/6613117 PMC 1010855 · pubmed ↗
- 8Biological basis for syphilis Clin Microbiol Rev Lafond RE Lukehart SA 29491920061641852110.1128/CMR.19.1.29-49.2006 PMC 1360276 · doi ↗ · pubmed ↗