Piloting a Patient-Driven Online Survey to Better Understand Cancer in Adolescents and Young Adults (AYA) in the United States
Lynda Beaupin, Scott Borinstein, Nicholas D Yeager, Denise Rokitka, Jennifer Schweitzer, Odochi Uwazurike, John Senall, Earnest Amankwah, Peter H Shaw

TL;DR
A patient-driven online survey was piloted to understand cancer experiences among adolescents and young adults in the U.S.
Contribution
The study introduces a feasible and effective online survey method for gathering insights from AYA cancer patients and survivors.
Findings
A 28-item online survey was successfully completed by 76% of registered AYA cancer patients and survivors.
The survey covered demographics, treatment, clinical trials, and socioeconomic impacts.
The approach proved feasible for engaging this unique patient population.
Abstract
Adolescents and young adults (AYAs) with cancer are a unique patient population in oncology. An opt-in, secure online survey was conducted among a general population of AYA patients and survivors to better understand the current landscape of AYA cancer. A 28-item online survey was designed for cancer patients and survivors diagnosed between the ages of 18 and 39 years. It comprised questions about demographics, treatment site, clinical trial involvement, support services available, and impact on employment, schooling, and finances. A total of 590 patients registered and 447 (76%) completed the survey. This online exercise was found to be feasible and can serve as an effective method to survey the AYA cancer population.
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
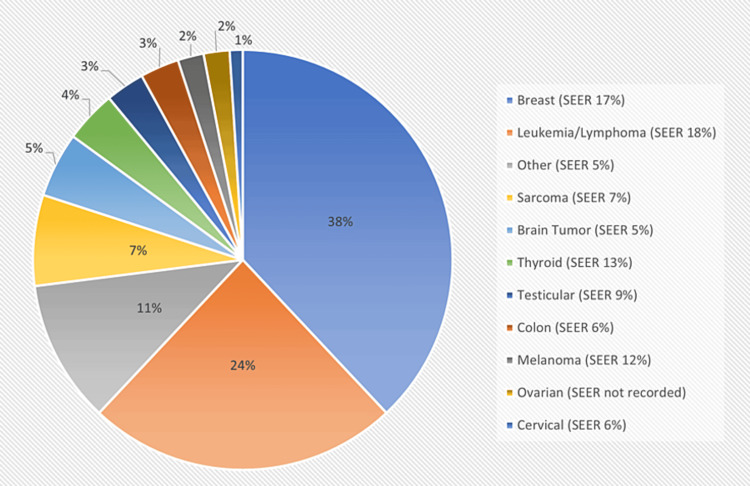 Figure 1
Figure 1| Question | ||
| Age in years, median (range) | 33 (18-60) | |
| Sex | N | % |
| Female | 380 | 85% |
| Male | 67 | 15% |
| Race (can select more than one) | ||
| White | 420 | 94% |
| Black/African American | 13 | 3% |
| Hispanic and Latino | 18 | 4% |
| Asian | 17 | 4% |
| Native American/Alaska Native | 5 | 1% |
| Personal/family situation at the time of the survey | ||
| Married/living with partner | 281 | 63% |
| Single and never married | 172 | 38% |
| Divorced or separated | 24 | 5% |
| Raising children at the time of the survey | ||
| Yes | 210 | 47% |
| No | 237 | 53% |
| Education completed | ||
| Some or completed high school | 25 | 6% |
| Some college/vocational school | 62 | 14% |
| College degree/postgraduate degree | 360 | 80% |
| Health insurance at diagnosis | ||
| Yes | 421 | 94% |
| No | 24 | 5% |
| I don’t know | 2 | 0.40% |
| Lapses in health insurance during treatment | ||
| Yes | 51 | 11% |
| No | 390 | 87% |
| I don’t know | 6 | 1% |
| Question | N | % |
| How long were you experiencing symptoms before seeking care? | ||
| Weeks | 134 | 32% |
| Months | 131 | 31% |
| Days | 73 | 17% |
| No symptoms – found on a routine visit | 64 | 15% |
| One year or longer | 45 | 11% |
| Treatment setting | ||
| Cancer center | 277 | 62% |
| Community hospital or community clinic | 58 | 13% |
| Pediatric cancer center or children's hospital | 49 | 11% |
| Independent adult cancer oncology practice | 49 | 11% |
| Other | 14 | 3% |
| How did you choose your primary oncology provider? (Can select more than one) | ||
| My doctor referred me | 287 | 64% |
| I did my own research | 176 | 39% |
| Shortest distance from home | 100 | 22% |
| Based on my insurance | 81 | 18% |
| Currently receiving cancer treatment | ||
| Yes | 183 | 41% |
| No | 264 | 59% |
| Aware of available clinical trials | ||
| Yes | 126 | 28% |
| No | 98 | 22% |
| I don’t know | 223 | 50% |
| Did your doctor recommend a clinical trial? | ||
| Yes | 114 | 25% |
| No | 316 | 71% |
| I don’t know | 17 | 4% |
| Quality of care you received | ||
| Excellent | 210 | 47% |
| Very good | 158 | 35% |
| Good | 53 | 12% |
| Fair | 23 | 5% |
| Poor | 3 | 0.70% |
| Information on long-term side effects | ||
| I have enough information | 246 | 55% |
| I need some more information | 124 | 28% |
| I need much more information | 37 | 8% |
| Does not apply | 40 | 9% |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsChildhood Cancer Survivors' Quality of Life · Adolescent and Pediatric Healthcare · Global Cancer Incidence and Screening
Introduction
Adolescents and young adult (AYA) cancer patients aged 15-39 years had demonstrated inferior survival rates for many malignancies compared to older and younger patients from the 1970s through 2000 [1], albeit some progress in survival rates over the last 10 years [2]. The reasons for this are multifactorial, including a low index of suspicion for cancer in the AYA population, delay in diagnosis, lack of insurance, referral patterns of these patients, lower rates of clinical trial enrollment, poor treatment compliance, and poor understanding of the biology of AYA malignancies [3]. Although pediatric cancer accounts for <1% of all new cases annually in the United States, AYA patients make up 4.6% of all new cases, which equates to more than 88,000 new cancer patients per year, and account for 1.5% of all cancer deaths, or approximately 9,000 per year [4]. Our understanding of cancer in this unique population was mostly derived from retrospective epidemiological studies, and there is a lack of research based on self-reported data. While most pediatric patients are treated at academic medical centers where clinical trial enrollment is high, most young adults >18 years are treated at community hospitals [5,6], where they are significantly less likely to be enrolled in therapeutic or non-therapeutic clinical trials, leading to a knowledge gap related to this vulnerable patient population [7].
In 2005, the National Cancer Institute (NCI), with support from the Lance Armstrong Foundation (LIVESTRONG), convened a Progress Review Group on AYA cancer [8]. Its recommendations led to the first national cohort study of AYA cancer patients in the United States: the Adolescent and Young Adult Health Outcomes and Patient Experience (AYA HOPE). Study participants diagnosed between the ages of 15 and 39 years were identified from seven NCI Surveillance, Epidemiology, and End Results (SEER) cancer registries, and 524 participants who were diagnosed between July 1, 2007, and October 31, 2008, with common AYA cancers were enrolled [9]. Researchers in Germany performed the AYA-Leipzig study, a longitudinal study that looked into different aspects of the lives of AYA cancer survivors and elucidated various needs of these patients regarding psychological distress and quality of life. Most of their study subjects were recruited through rehabilitation clinics and acute care hospitals [10-13]. Also, recently two multicenter studies examined the financial and employment-related impact among AYA cancer survivors, one involving only women [14] and the other both men and women [15].
Although AYA HOPE has provided comprehensive information on AYAs, a simplified approach to assess the current landscape of AYA survivors may be an effective method to engage with and learn more about this unique population. The Consortium of Adolescent and Young Adult Cancer Centers (CAYACC) was established to improve our understanding of AYA cancer in the United States. An online, web-based platform was created to collect self-reported health and psychosocial information from AYAs both in academic and community settings. The goal of this study was to assess the feasibility of an opt-in, secure online survey to collect data from a broader landscape of AYA patients and survivors.
Materials and methods
In this cross-sectional study, an internet-based online survey was designed for cancer patients and survivors diagnosed between the ages of 18 and 39 years to collect information about their cancer diagnosis, treatment setting, clinical trial access and enrollment, insurance status, social support, and fertility preservation utilization. The inclusion criteria were as follows: individuals diagnosed with cancer between the ages of 18 and 39 years. Respondents could be older than 39 years at the time of survey completion if they had been diagnosed and treated within the established age range. The survey was open from April 2018 to February 2019. Patients were recruited through social media and outreach to AYA cancer programs and support organizations. Patients self-enrolled and completed a 28-question confidential study. No identifying data were collected. Only completed survey data were included for analysis. Survey participation implied informed consent. The survey was approved by the Roswell Park Comprehensive Cancer Center (RPCCC)’s Institutional Review Board. Data were compiled through a website and securely stored on a REDCap database through the RPCCC [16].
Dichotomous items involved questions about insurance at the time of diagnosis, lapses in insurance during treatment, treatment status, awareness of clinical trials, and physician’s recommendation for participation in a clinical trial. Data on the duration of symptoms, treatment setting, selection of a provider, quality of care, and information on side effects were ascertained using the questions indicated in the survey. Survey responses were summarized as counts and percentages and age at diagnosis was summarized as median and range. We did not test any hypothesis in this study and hence no p-values are presented (see the Appendices for the full questionnaire).
Results
Demographics
A total of 590 patients registered and 447 (76%) completed the survey, as summarized in Table 1. The median age of respondents was 33 years at the time of survey entry (range: 18-60 years) with an IQR of 11. Most patients were female (n = 380, 85%) and self-described as Caucasian (n = 420, 94%). Most patients (n = 281, 63%) were married or living with a partner and nearly half (n = 210, 47%) were parents. Most (n = 360, 80%) had a college degree.
Diagnosis and access to care
The distribution of cancer diagnoses among the participants is shown in Figure 1, with the distribution from the SEER data included for comparison. The most common diagnoses were breast cancer, which comprised more than one-third (N = 170, 38%) of all survey responses, and leukemia and lymphoma (N = 107, 24%).
Distribution of cancer diagnoses compared to SEER dataSEER: Surveillance, Epidemiology, and End Results
Table 2 summarizes the characteristics of the patient cancer experience. Most patients experienced symptoms for weeks to months before seeking medical care (n = 265, 63%). Only a small proportion (n = 45, 11%) stated that their symptoms lasted more than one year before physician evaluation, and over one quarter (n = 137, 32%) had either no symptoms or symptoms for days before medical care. Most received or were receiving care at a cancer center or children’s hospital (n = 326, 73%) rather than at a community hospital or private practice. Nearly all patients were satisfied with the cancer treatment they received, most rating it as “very good” or “excellent” (n = 368, 82%). When asked if clinical trials were available at diagnosis, 50% were not sure (n = 223), 28% stated yes (n = 126), and 22% no (n = 98). When asked about overall clinical trial participation, 64% of patients (n = 286) stated that they had participated, 31% had not (n = 139), and 5% did not know (n = 22). Many participants were actively receiving therapy at the time of completion of the survey (n = 183, 41%).
Education and employment
Most patients (n = 402, 90%) were engaged in full-time employment or school. Nearly all patients needed to make significant work/educational changes due to their cancer diagnosis, such as needing to take extended time off (n = 191, 43%), switching to part-time (n = 48, 10%), or stopping work/school completely (n = 114, 26%). Only 23% (n = 103) of the patients reported that cancer had no impact on either work or school. Of note, 45% of the patients (n = 201) in school reported no impact on their education plans, while 21% (n = 94) had a somewhat negative impact, 7% a very negative impact (n = 31), 6% a somewhat positive impact (n = 27), and 6% a very positive impact (n = 27). Regarding the effect of cancer on work plans, 42% reported a somewhat negative impact (n = 188), 24% no impact (n = 107), 19% a very negative impact (n = 85), 8% a very positive impact (n = 36), and 5% a somewhat positive impact (n = 22).
Financial impact and social support
Most (79%) participants stated that cancer had a negative impact financially (n = 353). A small segment (15%) stated that the cancer diagnosis had no impact (n = 67) and only a few (4%) thought that it had a positive financial impact (n = 18). One quarter (27%) received professional advice to help figure out payment of healthcare costs (n = 121). Psychosocial support was provided mostly by family (77% mother, 54% father, 36% sister, 22% brother) in addition to friends (60%) and a significant other (12%). Very few (2%) reported no support (n = 9). Many patients relied on psychosocial support groups, with 39% participating in person (n = 174) and 62% in an online or social media support group (n = 277).
Knowledge of long-term side effects and fertility risks
Regarding knowledge about the long-term side effects of therapy, nearly half (n = 197, 44%) felt that they were adequately educated. Approximately one-third (n = 156, 35%) needed some additional information and 18% (n = 80) needed much more information. When asked specifically about the fertility risks of their therapy, 46% (n = 206) thought they had been adequately informed, 22% (n = 98) needed some more information and 10% (n = 45) needed much more information. When asked if someone at their treatment center discussed the potential impact of therapy on fertility, 73% (n = 326) said yes, 22% (n = 98) no, and 4% (n = 18) were unsure. When asked if they had been offered fertility preservation services (sperm banking oocyte/embryo cryopreservation), 64% (n = 287) stated they did not use any of these services, 14% (n = 63) banked sperm, 14% (n = 63) froze oocytes, and 7% (n = 31) froze embryos. The cost was a major barrier for nearly half (n = 215, 48%) of these patients, and two-thirds (n = 291, 65%) stated that at the time of diagnosis, fertility preservation was not a priority to them, despite it hurting future family planning for 62% (n = 277).
Insurance coverage
Nearly all patients (n = 420, 94%) had insurance at diagnosis; however, 12% (n = 54) reported that they had lapses in insurance coverage during or after treatment; 17% (n = 76) of patients stated that their decision about where to receive cancer care was dictated by insurance coverage. Most patients (n = 340, 76%) had private health insurance through an employer or school. A small segment (n = 49, 11%) were covered through their parents’ insurance plan. A few respondents (n = 54, 12%) were enrolled in Medicaid, while 5% (n = 22) were insured through a federal or state exchange through the Affordable Care Act (ACA). When asked the question “Were there any tests or treatments your oncologist recommended for cancer not covered by insurance?”, 35% (n = 156) responded “yes.” In instances where the tests and treatments were not covered, most patients (n = 344, 77%) stated that they still received them.
Discussion
AYA cancer patients face unique challenges that hinder their ability to receive optimal health care. The models of cancer care for these patients vary between medical centers and regions, and each medical team has its own unique environment and inherent strengths and challenges in terms of delivering care to its patients. Clinicians who focus on improving AYA cancer outcomes have learned that collaboration and data sharing are paramount in these efforts. It is through cooperative meetings that the idea for CAYACC and this patient-reported survey emerged.
By engaging in this effort, we were able to collect meaningful data describing the AYA cancer care climate effectively and economically from around the country in under one year, with 590 unique patients starting and 447 completing the full survey (76%). The CAYACC registry was created as a user-friendly platform and registered a substantial group of patients in a short period, demonstrating that such a tool is feasible and can be useful in studying this population.
Our study has certain limitations. We acknowledge that updated AYA SEER data from 2014-2018 exists [4] and is now available; however, the data is less granular and shows similar disease numbers compared to earlier SEER data, prompting us to choose to compare our results to the 2000-2009 data [17]. While we were able to enroll many AYA patients and survivors of cancer, most of our respondents were female, white, well-insured, and well-educated, likely because a greater percentage of respondents had breast cancer when compared to the SEER data (38% vs 17%). Unfortunately, this demographic distribution limits our ability to adequately assess the cancer experience of patients from lower socioeconomic strata or persons of color. Most of the respondents were treated at a cancer center or pediatric hospital vs. a community hospital. Patients were almost uniformly very happy with the care they received. The quality of care in our survey was subjective, and hence it is unclear whether the high overall satisfaction with the care these patients received (82% reporting “very good” or “excellent”) has any correlation with the setting in which they were treated.
Another shortcoming of our research is that 94% of surveyed patients had insurance at the time of diagnosis, which is most likely skewed to a more advantaged socioeconomic demographic, compared to the majority of AYA cancer patients, who have traditionally been the least insured age group in the United States [18]. The insurance coverage landscape has changed for this population after the passage of ACA in 2010, which allows young adults to remain as dependents until 26 years of age [19]. It is unclear, however, how much of an impact the ACA has had on the insurance coverage of our patients based on the questions in our survey. The AYAs we surveyed continue to report several ongoing challenges, especially financial issues and a lack of clinical trial-related knowledge despite national efforts to improve education and access. Challenges in medical and social areas carry over into survivorship, as our survey reveals.
Conclusions
Overall, we have demonstrated the feasibility of a patient-driven survey to accelerate the tracking of AYA cancer populations and develop robust databases. There has not been a follow-up to the AYA HOPE study or any other substantial AYA online American survey study to date. Our study, despite its limitations, demonstrates that an online patient-driven registry is feasible, not geographically limited, and treatment center-agnostic while being inexpensive to execute. It has established a method to engage with AYAs, which can be utilized to study this unique population further with more focused, in-depth questionnaires. The scope and reach of future surveys could be further expanded through more aggressive marketing and by increasing the number of cooperating centers to obtain a more representative AYA population in the United States.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Highlights and challenges Cancer Epidemiology in Older Adolescents and Young Adults 15 to 29 Years of Age, Including SEER Incidence and Survival, 1975-2000 Bleyer W Barr R 911Bethesda, MD National Cancer Institute 22006 https://seer.cancer.gov/archive/publications/aya/aya_mono_complete.pdf
- 2Survival outcomes for cancer types with the highest death rates for adolescents and young adults, 1975-2016 Cancer Lewis DR Siembida EJ Seibel NL Smith AW Mariotto AB 4277428612720213430855710.1002/cncr.33793 · doi ↗ · pubmed ↗
- 3Closing the gap: research and care imperatives for adolescents and young adults with cancer; Report of the Adolescent and Young Adult Oncology Progress Review Group 7 2024 2006 https://www.cancer.gov/types/aya/research/ayao-august-2006.pdf
- 4Cancer stat facts: cancer among adolescents and young adults (AY As) (ages 15-39). Surveillance, Epidemiology, and End Results Program 7 2024 2024 https://seer.cancer.gov/statfacts/html/aya.html
- 5Patterns of care among adolescents with malignancy in Ohio J Pediatr Hematol Oncol Yeager ND Hoshaw-Woodard S Ruymann FB Termuhlen A 1722282006 https://pubmed.ncbi.nlm.nih.gov/16394887/16394887 · pubmed ↗
- 6Access to pediatric cancer care by age, race, and diagnosis, and outcomes of cancer treatment in pediatric and adolescent patients in the state of Georgia J Clin Oncol Howell DL Ward KC Austin HD Young JL Woods WG 461046152520071792555610.1200/JCO.2006.07.6992 · doi ↗ · pubmed ↗
- 7Childhood cancer patients' access to cooperative group cancer programs: a population-based study Cancer Liu L Krailo M Reaman GH Bernstein L 133913459720031259924310.1002/cncr.11192 · doi ↗ · pubmed ↗
- 8Highlights and challenges. In: Bleyer A,O’Leary M, Barr R, Ries LAG, eds. Cancer Epidemiology in Older Adolescents and Young Adults 15 to 29 Years of Age, including SEER Incidence and Survival, 1975-2000, NIH Pub No 06-5767. Bethesda MD: National Cancer Institute Bleyer W Barr R 9112006 https://seer.cancer.gov/archive/publications/aya/aya_mono_complete.pdf