An Infant With COVID-19 Presenting With a Bulging Fontanel: A Case Report and Literature Review
Hiroyuki Kuroda, Yoshiki Kusama, Ayu Ogura, Takashi Matsunaga, Yukari Atsumi, Katsunori Kamimura

TL;DR
An infant with mild COVID-19 presented with a bulging fontanel, initially raising suspicion of bacterial meningitis, but tests ruled out serious infection.
Contribution
Highlights the low specificity of bulging fontanel in infants with COVID-19 to avoid unnecessary antibiotic use.
Findings
The infant showed no signs of bacterial meningitis despite a bulging fontanel.
Fever resolved quickly, and the infant was discharged in good condition.
Cerebrospinal fluid tests were normal, confirming no bacterial infection.
Abstract
A bulging fontanel is a sign of elevated intracranial pressure, which can be caused by diseases with intracranial fluid retention or swelling of the cerebral parenchyma. We experienced a case of an infant with a typical course of mild coronavirus disease 2019 (COVID-19) but with a bulging fontanel as a finding at presentation. The patient, a three-month-old boy with no underlying conditions, presented to the emergency clinic with fever, vomiting, and loss of appetite. Due to the absence of crying and the bulging fontanel, he was referred to our hospital with suspected bacterial meningitis. The diameter of the anterior fontanel was 2.5 cm, as measured by the Popich and Smith method. He showed no signs of consciousness impairment and appeared to be as active as usual. Computed tomography revealed a bulging fontanel. Cerebrospinal fluid examination showed no elevated cell counts, and…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
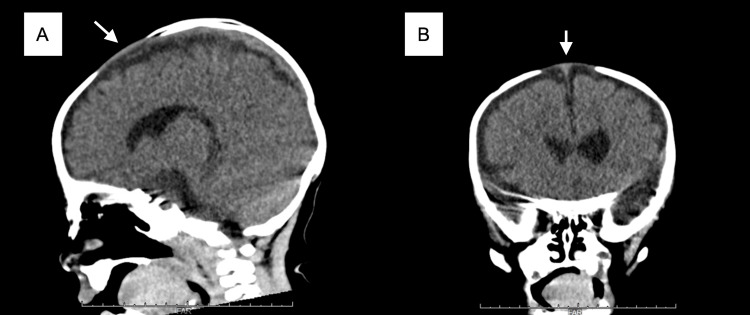 Figure 1
Figure 1| Test | Unit | Case | Reference |
| Leukocyte count | 109/μL | 5.8 | 3.3-8.6 |
| Percentage of neutrophils | % | 39.3 | 43-65 |
| Percentage of lymphocyte | % | 38.0 | 20-50 |
| Red blood cell count | 1012/μL | 4.35 | 4.35-5.55 |
| Hemoglobin | g/dL | 11.4 | 13.7-16.8 |
| Thrombocyte count | 109/μL | 216 | 158-348 |
| Total billirubin | mg/dL | 0.6 | 0.4-1.5 |
| AST | IU/L | 74 | 13-30 |
| ALT | IU/L | 65 | 10-42 |
| Urea nitrogen | mg/dL | 6.6 | 8.0-20 |
| Creatinine | mg/dL | 0.26 | 0.65-1.07 |
| Creatine kinase | IU/L | 130 | 59-248 |
| Glucose | mg/dL | 109 | 73-109 |
| C-reactive protein | mg/dL | 0.24 | 0.00-0.14 |
| Procalcitonin | ng/mL | 0.13 | < 0.5 |
| Sodium | mmol/L | 138 | 138-145 |
| Potassium | mmol/L | 4.7 | 3.6-4.8 |
| Chloride | mmol/L | 107 | 101-108 |
| Total cell count (CSF) | /μL | 1 | 0-5 |
| Total protein (CSF) | mg/dL | 13.7 | 8-43 |
| Glucose (CSF) | mg/dL | 57 | ND |
| Reported year | Authors | Age | Sex | Lumbar tap | Brain imaging | Treatment | Hospital stay |
| 2021 | Schiff et al. [ | 4 month | Girl | Done | CT | Ceftriaxone | Not hospitalized |
| 2022 | Al Amri et al. [ | 6 month | Girl | Done | Ultrasonography | Ceftriaxone | Not hospitalized |
| 2023 | Sethuraman et al. [ | 9 month | Boy | Done | CT and MRI | Ceftriaxone, clarithromycin, and acyclovir | 5 days |
| This case | 3 month | Boy | Done | CT | Cefotaxime and vancomycin | 3 days |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsTraumatic Brain Injury and Neurovascular Disturbances · Bacterial Infections and Vaccines · Cerebrospinal fluid and hydrocephalus
Introduction
A bulging fontanel is a sign of elevated intracranial pressure, which is caused by diseases with intracranial fluid retention or swelling of the cerebral parenchyma [1]. There is no clear definition of a bulging fontanel, but it can be identified by palpating the bulge and touching the bone in the vestibular area. Meningitis is a well-known infectious disease that can cause bulging fontanel, but this symptom can also be caused by other infections, such as roseola infantum [2]. We experienced the case of an infant who presented with a typical course of mild COVID-19 but had a bulging fontanel at presentation. Although it is difficult to prove a bulging fontanel on physical examination due to the lack of an objective assessment and modification of the symptom by crying [3], in the present case, it was demonstrated on computed tomography (CT). Since there are few case reports of COVID-19 with bulging fontanel, we report this case along with a literature review of previous cases.
Case presentation
Case
A three-month-old boy with no notable medical history presented to the emergency clinic with poor feeding, a single episode of vomiting, and a fever. He was referred to our hospital with suspected meningitis due to the absence of crying and a bulging fontanel. COVID-19 was diagnosed based on a positive qualitative SARS-CoV-2 antigen test at the clinic. He had been born via cesarean section at 37 weeks and four days gestation without apparent asphyxia, with a birth weight of 2,564 g. No maternal infections were noted prenatally, and the mother’s group B Streptococcus (GBS) screening test was negative. The mother had not consumed cured ham or cheese during pregnancy. The boy had received the Hib vaccine twice, the pneumococcal vaccine twice, the hepatitis B vaccine twice, and the tetanus, diphtheria, and pertussis vaccines twice. His mother had been diagnosed with COVID-19 17 days before his hospital visit.
History before admission
At the emergency department, the patient’s vital signs were as follows: body temperature, 39.0℃; heart rate, 178 beats/min; respiratory rate, 40 breaths/min; and oxygen saturation, 97% on room air. The capillary refilling time was less than two seconds. In the dorsal position, a physician was unable to follow the entire circumferential bone edge of the anterior fontanel that was suspected to be bulging. The diameter of the anterior fontanel was 2.5 cm, as measured by the Popich and Smith methods, which determine the size by averaging the width and length of the fontanel. He showed no signs of consciousness impairment and appeared to be as active as usual. The patient’s skin color and muscle tone were normal. Sucking and grasping reflexes in both the palms and soles were intact. There were no findings of sunset eye signs or other neurological abnormalities, such as paralysis. There were no abnormalities of breath or heart sounds. The patient’s respiratory pattern was stable, and there was no suggestion of circulatory failure. A projection of the large fontanel from the skull was discovered on computed tomography, which was conducted to rule out cerebral bleeding and mass lesions. There were no space-occupying or hemorrhagic lesions, hydrocephalus, or bone fractures (Figure 1).
Computed tomography findingsSagittal (A) and coronal (B) reconstruction showed a bulging fontanel. The images show the projection of the large fontanel from the skull (arrows).
Considering the possibility of meningitis, cefotaxime (100 mg/kg) was administered after taking a blood culture. Laboratory analysis revealed the following (Table 1): white blood cell count, 5.8 × 10^9^/L; C-reactive protein, 0.24 mg/dL; procalcitonin, 0.13 ng/mL; and serum glucose, 10^9^ mg/dL. There were no organ damage or electrolyte abnormalities, except mild elevation of aspartate aminotransferase (74 IU/L) and alanine aminotransferase (65 IU/L). This mild liver damage was considered attributable to COVID-19. Lumbar puncture revealed a white blood cell count of 1.0/mm^3^, a protein level of 13.7 g/dL, and a glucose level of 57 mg/dL. These laboratory data did not indicate meningitis.
Differential diagnosis
Cerebral hemorrhage, brain tumor, brain abscess, hydrocephalus, meningitis, head trauma, and viral infection were included as differential diseases since a bulging fontanel occurs due to elevated intracranial pressure.
Clinical course
Due to the patient's young age of three months and the presence of fever and vomiting, it was deemed necessary to rule out bacterial meningitis. We decided to treat the child with a regimen for bacterial meningitis until blood and cerebrospinal fluid cultures were confirmed to be negative for bacteria. On admission, the patient was treated with cefotaxime and vancomycin. Forty-eight hours after admission, blood and cerebrospinal fluid cultures were negative, and antibiotic medication was discontinued. On the day after admission, the patient’s fever subsided, and his general status improved. He was discharged on the third day of hospitalization. Three days after discharge, the patient was reassessed in the outpatient department and was found to be well. Follow-up laboratory analysis and imaging were not performed to avoid unnecessary invasive procedures and radiation exposure.
Discussion
We reported the case of a three-month-old infant with COVID-19 who presented with a bulging fontanel but no evidence of meningitis and who had a mild natural course. Although bulging fontanel is a well-known finding suspicious for meningitis, Shacham et al. reported in 2008 that only one case of bacterial meningitis occurred among 153 infants presenting with fever and bulging fontanel and they raised questions about the need for routine CSF testing in infants with these symptoms [3]. In a more recent study, Takagi et al. reviewed 304 febrile patients of 2-18 months of age with bulging fontanel and reported that 40% had upper respiratory tract infection, 25% had aseptic meningitis, 9.8% had some type of viral infection, and only 0.3% had bacterial meningitis [4]. Freedman et al. pointed out that vaccination may be a cause of bulging fontanel [5], and Amarilyo et al. reported that the sensitivity and specificity of bulging fontanel for bacterial meningitis were 50% and 60%, respectively, with a positive predictive value of only 38% during a period when pneumococcal and Hib vaccines were widely available [6]. Therefore, bulging fontanel should not be considered the sole determining factor in the diagnosis of meningitis, but should be combined with other physical and laboratory findings.
At the beginning of the COVID-19 pandemic, cases in infants were rare, but the emergence of the Omicron strain made it more prevalent in infants [7]. Nevertheless, to our knowledge, only three cases of COVID-19 patients with bulging fontanel have been reported in the literature [8-10] (Table 2).
All three cases were treated with antibacterial or anti-herpesvirus medication, although imaging and CSF examinations were performed with no evidence of meningitis. These patients fully recovered with a typical mild course, consistent with COVID-19. Evaluating and treating fever in an infant who appears well is a challenging issue. The American Academy of Pediatrics guidelines state that, in infants older than 29 days of age with an unknown source of infection, there is no need for CSF testing if there is no elevated inflammatory response on a blood test [11]. Despite this recommendation, if there are signs that suggest meningitis, such as a bulging fontanel, it would be difficult to choose not to perform a CSF test, as it is the only way to confirm the presence of meningitis [12]. However, in the absence of elevated cell counts on CSF testing, the appropriateness of empiric antimicrobial administration should be debated. Antimicrobial treatment during infancy leads to the acquisition of drug-resistant bacteria. Future allergic diseases such as bronchial asthma, atopic dermatitis, and obesity have also been noted [13,14]. If the likelihood of meningitis is clearly low based on a physical examination and laboratory findings, it may be possible to observe the patient without administering antimicrobial medication. However, no studies have examined the need for antibiotic medication in infants with a bulging fontanel who are otherwise well. In fact, antibiotics have been used in all previous cases of infants with COVID-19 with a bulging fontanel. Further research is necessary to discuss the appropriateness of observing infants without medication in such cases.
Conclusions
While a bulging fontanel is a finding that requires attention and may suggest bacterial meningitis, it can also be observed in infants with common viral infections, including COVID-19. When an infant diagnosed with COVID-19 presents with a bulging fontanel, it is important to be aware of its low specificity, and excessive antibiotic treatment should be reconsidered.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1The abnormal fontanel Am Fam Physician Kiesler J Ricer R 25472552152003 https://www.aafp.org/pubs/afp/issues/2003/0615/p 2547.html 12825844 · pubmed ↗
- 2The not-so-soft spot: pathophysiology of the bulging fontanelle in association with roseola Pediatr Emerg Care Cristoforo T Le NK Rye-Buckingham S Hudson WB Carroll LF 0836202010.1097/PEC.000000000000144729489601 · doi ↗ · pubmed ↗
- 3Bulging fontanelle in febrile infants: is lumbar puncture mandatory?Arch Dis Child Shacham S Kozer E Bahat H Mordish Y Goldman M 6906929420091953152810.1136/adc.2009.158956 · doi ↗ · pubmed ↗
- 4Bulging fontanelle in febrile infants as a predictor of bacterial meningitis Eur J Pediatr Takagi D Oren-Ziv A Shles A Schujovitzky D Yechiam H Rosenbloom E 1243124818020213316923810.1007/s 00431-020-03865-4 · doi ↗ · pubmed ↗
- 5Transient bulging fontanelle after vaccination: case report and review of the vaccine adverse event reporting system J Pediatr Freedman SB Reed J Burwen DR Wise RP Weiss A Ball R 64064414720051629135610.1016/j.jpeds.2005.06.009 · doi ↗ · pubmed ↗
- 6Diagnostic accuracy of clinical symptoms and signs in children with meningitis Pediatr Emerg Care Amarilyo G Alper A Ben-Tov A Grisaru-Soen G 1961992720112134667610.1097/PEC.0b 013e 31820 d 6543 · doi ↗ · pubmed ↗
- 7Severe COVID-19 outcomes in pediatrics: an observational cohort analysis comparing Alpha, Delta, and Omicron variants Lancet Reg Health Am Bahl A Mielke N Johnson S Desai A Qu L 1004051820233647452110.1016/j.lana.2022.100405 PMC 9714340 · doi ↗ · pubmed ↗
- 8Bulging anterior fontanelle caused by severe acute respiratory syndrome coronavirus-2Pediatr Infect Dis J Sethuraman C Holland J Priego G Khan F Johnson R Keane M 0542202310.1097/INF.0000000000003750 PMC 972574036476525 · doi ↗ · pubmed ↗