Investigating Urinary Pathogens and Their Antibiotic Resistance: A Cross-Sectional Urine Culture Study
Muzamil Khan, Fazeel Hussain, Muhammad Naseem, Ruchira Clementina, Nida Gul, Aysha Habib, Laiba Ali Khan, Ayaz Ali, Waqas Rahim, Izhar Khan

TL;DR
This study examines urinary tract infection pathogens and their antibiotic resistance in Pakistan, finding higher rates in females and significant resistance to common drugs.
Contribution
The study provides current data on uropathogen prevalence and resistance patterns in a Pakistani population.
Findings
Females had a higher UTI prevalence (70%) compared to males (30%).
E. coli and Citrobacter were the most common pathogens in females.
High resistance was observed to drugs like ampicillin and polymyxin B.
Abstract
Introduction: Urinary tract infections (UTIs) are among the most prevalent infectious diseases. Females are more affected than males. The primary culprit is Escherichia coli. Multiple research investigations have documented widespread antimicrobial resistance in uropathogens, sparking global concerns, especially regarding the rise of multidrug resistance (MDR). Methodology: This cross-sectional study was conducted from December 2023 to March 2024. A non-probability purposive sampling technique was employed to select participants, and informed consent was obtained from them. Data were extracted from the culture and sensitivity reports of these patients. The collected data were meticulously entered into IBM SPSS Statistics for Windows, Version 21 (IBM Corp., Armonk, NY). The findings were then presented using a blend of percentages and numerical figures, offering a clear and concise…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
 Figure 1
Figure 1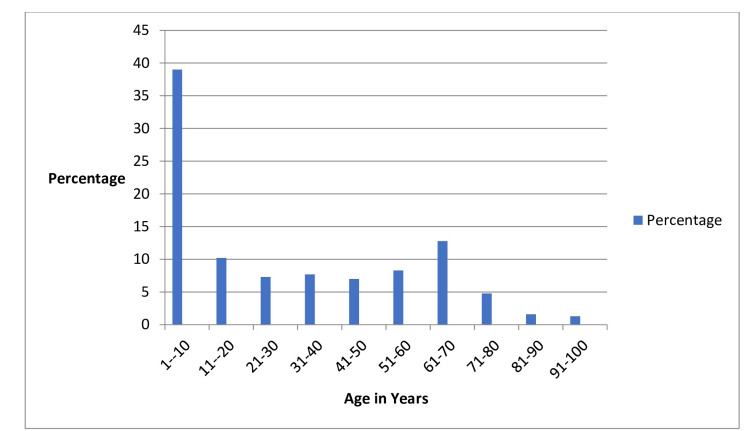 Figure 2
Figure 2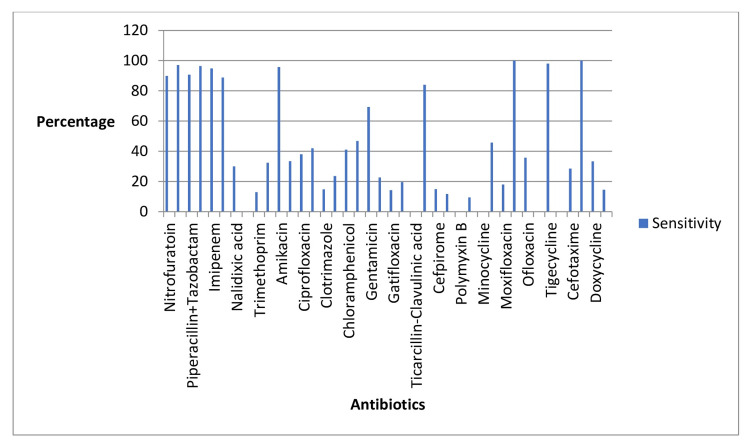 Figure 3
Figure 3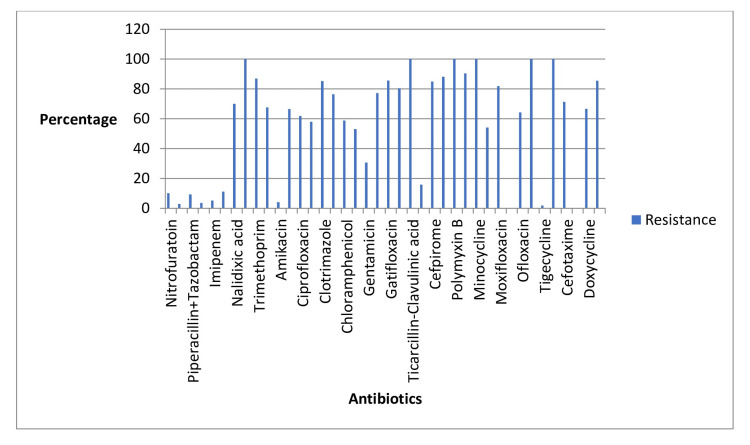 Figure 4
Figure 4| Male, | Female, |
|
| 94 (30) | 219 (70) | <0.001 |
| Age of participant (Years) | Male, | Female, | Total, |
| 1-10 | 28 (8.9) | 94 (30) | 122 (30.5) |
| 11-20 | 12 (3.8) | 20 (6.3) | 32 (8.0) |
| 21-30 | 4 (1.3) | 19 (6.1) | 23 (5.8) |
| 31-40 | 6 (1.9) | 18 (5.7) | 24 (6.0) |
| 41-50 | 5 (1.6) | 17 (5.4) | 22 (5.5) |
| 51-60 | 9 (2.8) | 17 (5.4) | 26 (6.5) |
| 61-70 | 15 (4.8) | 25 (7.9) | 40 (10.0) |
| 71-80 | 10 (3.1) | 5 (1.6) | 15 (3.8) |
| 81-90 | 5 (1.6) | 0 (0) | 5 (1.3) |
| 91-100 | 0 (0) | 4 (1.2) | 4 (1.0) |
| Bacteria name | Frequency ( | Percentage (%) | Male, | Female, | Total male patients, | Total female patients, |
| E. coli | 154 | 49.2 | 41 (13.1) | 113 (36.1) | 41 (43.6) | 113 (51.6) |
| Citrobacter | 82 | 26.2 | 18 (5.7) | 64 (20.4) | 18 (19.1) | 64 (29.2) |
| Enterobacter | 8 | 2.6 | 8 (2.5) | 0 (0) | 8 (8.5) | 0 (0) |
| Pseudomonas | 10 | 3.2 | 2 (0.6) | 8 (2.5) | 2 (2.1) | 8 (3.7) |
| Morganella morganii | 39 | 12.5 | 19 (6.1) | 20 (6.3) | 19 (20.2) | 20 (9.1) |
| Staphylococcus | 3 | 1.0 | 3 (0.9) | 0 (0) | 3 (3.2) | 0 (0) |
| Proteus | 2 | 0.6 | 1 (0.3) | 1 (0.3) | 1 (1.1) | 1 (0.5) |
| Serratia species | 11 | 3.5 | 2 (0.6) | 9 (2.8) | 2 (2.1) | 9 (4.1) |
| Providencia species | 4 | 1.3 | 0 (0) | 4 (1.2) | 0 (0) | 4 (1.8) |
| Antibiotic | Number tested | Sensitivity (S, %) | Resistance (R, %) |
| Nitrofurantoin | 237 | 89.87 | 10.12 |
| Fosfomycin | 208 | 97.11 | 2.88 |
| Piperacillin + Tazobactam | 312 | 90.70 | 9.29 |
| Meropenem | 310 | 96.45 | 3.54 |
| Imipenem | 310 | 94.83 | 5.16 |
| Cefoperazone/Sulbactam | 295 | 88.81 | 11.18 |
| Nalidixicacid | 40 | 30 | 70 |
| Ampicillin | 143 | 0 | 100 |
| Trimethoprim | 23 | 13.01 | 86.95 |
| Ceftriaxone | 179 | 32.40 | 67.59 |
| Amikacin | 289 | 95.84 | 4.15 |
| Aztreonam | 296 | 33.44 | 66.55 |
| Ciprofloxacin | 305 | 38.03 | 61.96 |
| Co-amoxiclav | 276 | 42.02 | 57.97 |
| Clotrimazole | 196 | 14.79 | 85.20 |
| Cefuroxime | 72 | 23.61 | 76.38 |
| Chloramphenicol | 180 | 41.11 | 58.88 |
| Ceftazidime | 301 | 46.84 | 53.15 |
| Gentamicin | 297 | 69.36 | 30.63 |
| Levofloxacin | 119 | 22.68 | 77.31 |
| Gatifloxacin | 21 | 14.28 | 85.71 |
| Cefixime | 92 | 19.56 | 80.43 |
| Ticarcillin-Clavulanic acid | 15 | 0 | 100 |
| Ertapenem | 113 | 84.07 | 15.92 |
| Cefpirome | 80 | 15 | 85 |
| Colistin | 17 | 11.76 | 88.23 |
| PolymyxinB | 15 | 0 | 100 |
| Tobramycin | 63 | 9.52 | 90.47 |
| Minocycline | 15 | 0 | 100 |
| Cefepime | 286 | 45.80 | 54.19 |
| Ofloxacin | 42 | 35.71 | 64.28 |
| Norfloxacin | 9 | 0 | 100 |
| Tigecycline | 261 | 98.08 | 1.91 |
| Cefobid | 30 | 0 | 100 |
| Cefotaxime | 203 | 28.57 | 71.42 |
| Sulfonamides | 3 | 100 | 0 |
| Doxycycline | 6 | 33.33 | 66.66 |
| Maxipime | 62 | 14.51 | 85.48 |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsUrinary Tract Infections Management · Enterobacteriaceae and Cronobacter Research · Pediatric Urology and Nephrology Studies
Introduction
One of the most common infectious disorders is urinary tract infection (UTI). With an estimated yearly global incidence of at least 250 million cases, UTIs are a common illness that doctors encounter in developing nations [1,2]. At any age, UTIs tend to affect both genders equally. However, due to their anatomical makeup or the high bacterial load in the urothelial mucosa, women are more likely than men to get UTIs. In addition to these factors, pregnancy, urinary tract blockage, and sexual activity all play a role in the development of UTIs in females. One in two women experiences a UTI at some point in their lives. According to reports, 30% of children worldwide suffer from UTIs. In Iran, it has been documented that approximately 1% of boys and 3% of girls experience their initial occurrence of UTI before reaching the age of 11 years [3].
Several types of gram-positive and gram-negative bacteria contribute to UTIs, but the primary culprit is Escherichia coli, a gram-negative, facultative anaerobic bacterium known for its uropathogenic properties [4]. Besides E. coli, UTIs commonly involve other microbes like Klebsiella spp., Acinetobacter baumannii, and Pseudomonas aeruginosa. Moreover, gram-positive bacteria, such as Methicillin-resistant Staphylococcus aureus (MRSA) and Staphylococcus saprophyticus, are also implicated in UTI occurrences [5].
The approach to treating UTI cases typically involves initiating empirical therapy, guided by knowledge derived from the antimicrobial resistance profile of the urinary pathogens [6]. Multiple research investigations have documented widespread antimicrobial resistance in uropathogens, sparking global concerns, especially regarding the rise of multidrug resistance (MDR) and extended-spectrum beta-lactamases (ESBLs) [7,8].
The growing challenge of antibiotic resistance among urinary tract bacteria presents a dynamic regional shift. Thus, it becomes imperative to discern which antibiotics have encountered resistance. This knowledge equips healthcare professionals with vital guidance for prescribing medications, ensuring informed decisions, and providing effective patient care. This study is motivated by the pressing need to navigate this evolving antibiotic resistance terrain, aiming to elevate healthcare standards and optimize treatment strategies.
Materials and methods
This cross-sectional study was conducted within the departments of General Medicine, Nephrology, and Urology at Khyber Teaching Hospital (KTH) in Peshawar, spanning from December 2023 to March 2024. Formal permission for data collection was obtained from the Medical Director of KTH and the Director of Medical Education at Khyber Medical College (Ref: 280/DME/KMC), ensuring adherence to ethical guidelines. All patients admitted to these departments with UTIs during the specified period were eligible for inclusion. A non-probability purposive sampling technique was employed to select participants, and informed consent was obtained from them. Patients with catheterization were excluded from the study to maintain the integrity and validity of the findings, as their urine samples could potentially be contaminated with bacteria from the catheter itself.
Procedure for bacterial isolation and identification
An early morning midstream urine sample was taken from UTI patients who have not used antibiotics for the past 48-72 hours and do not have catheters passed. Total samples were taken from 400 patients. The isolation of uropathogens was conducted using a surface streak method on both blood and MacConkey agar (Oxoid Ltd., Basingstoke, Hampshire, UK) with calibrated loops for a semiquantitative approach. These were incubated aerobically at 37 °C for 24 hours. Cultures that showed no growth after 24 hours were incubated for an additional 48 hours. A specimen was deemed positive for a UTI if a single organism was cultured at a concentration of ≥10^5^ CFU/mL. Bacterial identification was carried out using a series of biochemical tests, including indole, citrate utilization, oxidase activity, hydrogen sulfide production, lysine decarboxylase activity, lactose fermentation, urease activity, gas production, catalase activity, coagulase activity, mannitol fermentation, and susceptibility to novobiocin [9].
Susceptibility testing
Antibiotic susceptibility was carried out on Müller-Hinton agar and blood agar. The antimicrobial susceptibility of the isolated bacterial uropathogens was assessed using the disk diffusion method, following the guidelines provided by the Clinical Laboratory Standards Institute (CLSI) [10]. Antibiotic discs used were nitrofurantoin, fosfomycin, piperacillin + tazobactam, meropenem, imipenem, cefoperazone/sulbactam, nalidixic acid, ampicillin, trimethoprim, ceftriaxone, amikacin, aztreonam, ciprofloxacin, co-amoxiclav, clotrimazole, cefuroxime, chloramphenicol, ceftazidime, gentamicin, levofloxacin, gatifloxacin, cefixime, ticarcillin-clavulanic acid, ertapenem, cefpirome, colistin, polymyxin B, tobramycin, minocycline, cefepime, ofloxacin, norfloxacin, tigecycline, Cefobid (cefoperazone), cefotaxime, sulfonamides, doxycycline, and maxipime. A total of 313 patients showed growth of UTI-causing bacteria.
Data analysis
The collected data were meticulously entered into IBM SPSS Statistics for Windows, Version 21 (IBM Corp., Armonk, NY), a powerful statistical analysis tool, to explore the resistance and sensitivity profiles of the organisms under study. The chi-square test was applied to find out the relationship between UTI and gender. A P-value less than 0.05 was considered significant, while a P-value greater than 0.05 was considered insignificant. The findings were then presented using a blend of percentages and numerical figures, offering a clear and concise representation of the data. This approach not only enhances the accessibility of the results but also facilitates a deeper understanding of the intricate patterns observed in antimicrobial resistance.
Results
In our study, 400 patients participated, and 313 of them showed bacterial growth indicative of a UTI. Out of these 313 patients, 94 (30%) were male, while 219 (70%) were female. To determine the association between UTI occurrence and gender, we applied the chi-square test. The results showed a significant difference, with a P-value of less than 0.001. This statistical outcome indicates that the prevalence of UTIs is significantly higher among females compared to males (Figure 1).
Gender-wise prevalence.
In our study, the participants' ages ranged from 1 to 97 years. Among the 313 patients who exhibited bacterial growth indicative of a UTI, a notable observation was that the majority fell within the age group of 1-10 years, suggesting that younger patients, particularly those in early childhood, were more commonly affected by UTIs in our study. Further analysis revealed that within this age range, both males and females showed bacterial growth, although the overall prevalence remained higher among females. This age-specific trend underscores the importance of monitoring and addressing UTIs in pediatric population. Age-specific prevalence is illustrated in Figure 2 and Table 1.
Age-wise prevalence.
*Table 1: Gender-wise prevalence.The chi-square test was applied.P < 0.05 was considered significant, and P > 0.05 was considered nonsignificant.
Among the 313 patients who showed bacterial growth indicative of a UTI, approximately 154 (49.2%) were found to have E. coli, making it the most prevalent bacterium. This was followed by Citrobacter in 82 patients (26.2%), Morganella morganii in 39 patients (12.5%), Serratia species in 11 patients (3.5%), Pseudomonas in 10 patients (3.2%), Enterobacter in 8 patients (2.6%), Providencia in 4 patients (1.3%), Staphylococcus in 3 patients (1%), and Proteus in 2 patients (0.6%).
Further analysis revealed that the occurrence of E. coli and Citrobacter was notably higher in female patients, aligning with the overall trend of higher UTI prevalence among females in the study. Conversely, bacteria such as Enterobacter and Staphylococcus were found more frequently in male patients. This gender-specific distribution of bacterial growth highlights the need for targeted approaches in the diagnosis and treatment of UTIs, taking into consideration the differing bacterial profiles between male and female patients. Details are given in Table 2.
The results of the antibiogram analysis provided important insights into the drug sensitivities and resistances observed among the UTI-causing bacteria. Several antibiotics demonstrated notable effectiveness against these pathogens. Specifically, nitrofurantoin, fosfomycin, piperacillin/tazobactam, meropenem, imipenem, cefoperazone/sulbactam, amikacin, ertapenem, amoxicillin, tigecycline, and sulfonamides were identified as having high sensitivities. This indicates that these drugs were generally effective in inhibiting the growth of the UTI bacteria identified in our patient cohort.
On the other hand, certain antibiotics exhibited higher resistance rates among the bacteria. Notably, norfloxacin, Cefobid (cefoperazone), minocycline, polymyxin B, ticarcillin-clavulanic acid, and ampicillin showed lower efficacy, with the bacteria demonstrating substantial resistance to these medications. This resistance pattern suggests that these antibiotics may be less suitable for treating UTIs in the studied population.
The findings underscore the importance of conducting antibiogram analyses to inform the selection of appropriate antimicrobial therapy. By identifying which antibiotics are more likely to be effective and which are prone to resistance, healthcare providers can make more informed decisions, leading to better patient outcomes and more effective management of UTIs. Details are given in Tables 3-4 and Figures 3-4.
UTI antibiogram sensitivity profile.UTI, urinary tract infection
Antibiotics and their resistance profiles.
Discussion
The rise of antibiotic resistance is becoming a significant global issue. UTIs, which impact many people each year, are caused by bacteria exhibiting a range of resistance to different antibiotics [11]. Hence, identifying the resistance and sensitivity profiles of antibiotics in patients with UTIs is crucial. This knowledge enables healthcare providers to select the most effective treatment, ensuring better patient outcomes and helping to combat the growing issue of antibiotic resistance.
The prevalence of UTIs was higher in females than in males in our study, consistent with the findings of other research [12]. The higher prevalence of UTIs among females can be attributed to several factors that predispose women to these infections [13].
Our study reveals that E. coli is the most common organism responsible for UTIs, a finding that aligns with research conducted in both Iran [14] and Scotland [15]. While various studies indicate that E. coli is typically followed by Klebsiella in prevalence, our research identified Citrobacter as the second most common organism causing UTIs [16]. These variations depend on multiple factors, including geographic region, ethnicity, types of pollution, and other environmental influences [17]. Understanding these variations is crucial for developing targeted treatment strategies and preventive measures. The identification of Citrobacter as a significant UTI pathogen in our study suggests that regional microbial profiles should be closely monitored to ensure effective clinical management. Furthermore, the impact of environmental factors on pathogen prevalence underscores the need for comprehensive public health approaches that address not only medical treatment but also environmental and societal conditions. Future research should aim to explore these factors in greater depth to enhance our understanding of UTI etiology and improve patient outcomes across different regions.
In our study, E. coli and Citrobacter are more prevalent in females than in males, while Staphylococcus and Enterobacter are higher in male patients. A study from China also shows that E. coli is common in females [18].
In our study, the highest resistance was developed to ampicillin, which is consistent with the findings of other research [19, 20]. This widespread resistance can be attributed to the extensive and prolonged use of ampicillin in clinical settings, leading to selective pressure and the proliferation of resistant bacterial strains.
Our study shows higher sensitivity to amoxicillin, while other studies show resistance to it [19]. This discrepancy may be due to regional differences in antibiotic prescribing practices or variations in local bacterial populations. Additionally, variations in resistance patterns can arise from differences in study design, sample size, and the specific patient populations being studied. Understanding these variations highlights the importance of local antimicrobial susceptibility testing to guide effective antibiotic therapy.
Our study identified a notable resistance to polymyxin B, contrasting with other research that reports sensitivity to this antibiotic in multi-drug-resistant pathogens [21-23]. This unexpected finding raises serious concerns about evolving resistance patterns and suggests that local variations in antibiotic usage and resistance mechanisms may be at play. The emergence of resistance to polymyxin B, a critical last-resort antibiotic, underscores the urgent need for enhanced surveillance and innovative approaches to combat antimicrobial resistance. Our findings highlight the importance of continuous monitoring and adapting treatment strategies to effectively address the dynamic landscape of bacterial resistance.
Limitations
The primary limitation of our study is that it was conducted at a single center, Khyber Teaching Hospital. Additionally, the study duration was relatively short, spanning only four months.
Conclusions
Our study of 313 patients highlights a significant prevalence of UTIs among females compared to males. E. coli and Citrobacter were predominant in females, while Enterobacter and Staphylococcus were more prevalent in males. Antibiotic sensitivity analysis revealed promising results for nitrofurantoin, fosfomycin, and others, while resistance was notable against norfloxacin, polymyxin B, and others. These findings emphasize the need for targeted antibiotic therapy based on local resistance patterns to effectively manage UTIs.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Urinary tract infection in adults: research priorities and strategies Int J Antimicrob Agents Ronald AR Nicolle LE Stamm E 3433481720011129541910.1016/s 0924-8579(01)00303-x · doi ↗ · pubmed ↗
- 2Urinary tract infections in South Croatia: aetiology and antimicrobial resistance Int J Antimicrob Agents 2. BarisićZ Babić-Erceg A BorzićE 6164220032210.1016/s 0924-8579(03)00233-414527773 · doi ↗ · pubmed ↗
- 3Community-acquired urinary tract infections in children: pathogens, antibiotic susceptibility and seasonal changes Eur Rev Med Pharmacol Sci YolbaşI Tekin R Kelekci S 971976172013 https://pubmed.ncbi.nlm.nih.gov/23640446/23640446 · pubmed ↗
- 4Population structure of gut Escherichia coli and its role in development of extra-intestinal infections Iran J Microbiol Katouli M 597222010 https://pubmed.ncbi.nlm.nih.gov/22347551/22347551 PMC 3279776 · pubmed ↗
- 5Antimicrobial susceptibility of microorganisms causing urinary tract infections in Saudi Arabia J Infect Dev Ctries Balkhi B Mansy W Al Ghadeer S Alnuaim A Alshehri A Somily A 2202271220183185163010.3855/jidc.9517 · doi ↗ · pubmed ↗
- 6Laboratory diagnosis of urinary tract infections in adult patients Clin Infect Dis Wilson ML Gaido L 115011583820041509522210.1086/383029 · doi ↗ · pubmed ↗
- 7Antibiotic susceptibility patterns of urinary pathogens in female outpatients N Am J Med Sci Shaifali I Gupta U Mahmood SE Ahmed J 163169420122253655810.4103/1947-2714.94940 PMC 3334255 · doi ↗ · pubmed ↗
- 8Urinary tract infections: epidemiology, mechanisms of infection and treatment options Nat Rev Microbiol Flores-Mireles AL Walker JN Caparon M Hultgren SJ 2692841320152585377810.1038/nrmicro 3432 PMC 4457377 · doi ↗ · pubmed ↗