Prediction of mortality in patients with secondary pulmonary embolism based on primary admission indication: A short communication
Martin J Ryll, Toby N Weingarten, Juraj Sprung

TL;DR
This study compares different scores to predict mortality in ICU patients who develop secondary pulmonary embolism, finding that APACHE-IV performs best overall.
Contribution
The study evaluates the performance of PE-specific scores and APACHE-IV in predicting mortality for ICU patients with secondary PE.
Findings
APACHE-IV outperformed PESI and ICU-sPESI in predicting in-hospital mortality for ICU patients with secondary PE.
sPESI showed poor predictive performance across all ICU admission categories.
Mortality prediction was consistently weak for patients admitted due to infections, regardless of the score used.
Abstract
Secondary pulmonary embolism (PE) may significantly complicate the clinical course of intensive care unit (ICU) patients, creating the need for reliable stratification of severity and mortality risk in these patients. We evaluated the prediction of mortality in patients admitted to the ICU who subsequently developed a PE (i.e., secondary PE) using three PE-specific scores, the Pulmonary Embolism Severity Index (PESI), simplified PESI (sPESI), and modified sPESI (ICU-sPESI) and compared them to the gold standard for the assessment of ICU all-cause mortality, the Acute Physiology and Chronic Health Evaluation-IV (APACHE-IV). All critical care admission indications were grouped into four major categories: post-operative, cardiovascular, infectious (sepsis), and other. The APACHE-IV displayed better discriminative ability to predict in-hospital mortality than the PESI and ICU-sPESI, but…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
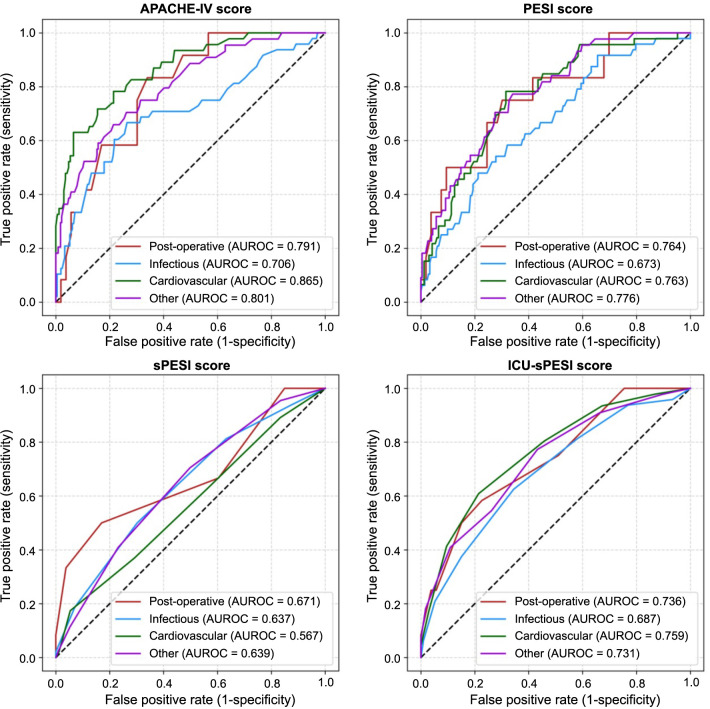 Figure 1
Figure 1|
|
|
|---|---|
| Post-operative ( | 18.5% [9.0%–27.9%] |
| Gastrointestinal | |
| Neurosurgical | |
| Cardiovascular | |
| Thoracic | |
| General/endocrine/otorhinolaryngological | |
| Infectious ( | 18.5% [13.7%–23.2%] |
| Sepsis, pulmonary/pneumonia | |
| Sepsis, renal/urinary tract infections | |
| Sepsis, gastrointestinal | |
| Sepsis, cutaneous/soft tissue | |
| Sepsis, other/unknown | |
| Endocarditis | |
| Encephalitis/meningitis | |
| Cholangitis | |
| Cardiovascular ( | 21.5% [16.0%–27.0%] |
| Cardiac arrest/MI | |
| Dysrhythmia (supraventricular, ventricular, etc.) | |
| Congestive heart failure | |
| Unstable angina | |
| Aortic dissection | |
| Other ( | 16.1% [11.8%–20.5%] |
| Emphysema/bronchitis | |
| Respiratory arrest | |
| ARDS/pleural effusions | |
| Cerebrovascular accident/stroke | |
| Gastrointestinal bleeding | |
| Acute renal failure | |
| Intracranial hemorrhage | |
| Cancer/neoplasm |
|
|
|
|
|
|
|---|---|---|---|---|
|
| ||||
| APACHE-IV | 54.0 [36.0–77.0] | 48.0 [32.0–66.0] | 78.0 [57.8–91.2] | 0.002 |
| PESI | 132.0 [99.0–178.0] | 124.0 [83.0–161.0] | 184.0 [152.5–216.2] | 0.005 |
| sPESI | 2.0 [1.0–2.0] | 2.0 [1.0–2.0] | 2.5 [1.0–4.0] | 0.056 |
| ICU-sPESI | 3.0 [2.0–4.0] | 3.0 [2.0–3.0] | 4.5 [2.8–5.5] | 0.010 |
|
| ||||
| APACHE-IV | 60.5 [46.0–80.0] | 58.0 [45.0–75.0] | 81.5 [55.8–98.5] | <0.001 |
| PESI | 143.5 [106.0–179.0] | 140.5 [100.8–170.0] | 170.0 [133.8–203.8] | <0.001 |
| sPESI | 2.0 [1.0–3.0] | 2.0 [1.0–3.0] | 2.5 [2.0–3.0] | 0.002 |
| ICU-sPESI | 3.0 [2.0–4.0] | 3.0 [2.0–4.0] | 4.0 [3.0–5.0] | <0.001 |
|
| ||||
| APACHE-IV | 56.5 [42.0–82.0] | 50.0 [38.8–65.0] | 112.0 [71.5–146.0] | <0.001 |
| PESI | 130.0 [93.0–162.8] | 118.5 [89.8–152.0] | 162.5 [144.2–197.2] | <0.001 |
| sPESI | 2.0 [1.0–3.0] | 2.0 [1.0–3.0] | 2.0 [1.0–3.0] | 0.151 |
| ICU-sPESI | 3.0 [1.0–4.0] | 2.0 [1.0–3.0] | 4.0 [3.0-5.0] | <0.001 |
|
| ||||
| APACHE-IV | 51.0 [40.0–70.0] | 49.0 [39.0–67.0] | 81.5 [59.5–110.5] | <0.001 |
| PESI | 137.0 [92.0–172.0] | 125.0 [85.0–163.0] | 178.0 [147.8–211.5] | <0.001 |
| sPESI | 2.0 [1.0–3.0] | 1.0 [1.0–2.0] | 2.0 [1.0–3.0] | 0.002 |
| ICU-sPESI | 2.0 [1.0–4.0] | 2.0 [1.0–4.0] | 4.0 [3.0–5.0] | <0.001 |
|
|
|
|
|
|
|
|
|---|---|---|---|---|---|---|
| Post-operative | 0.767 | 0.297 | 0.602 | 0.288 | 0.700 | 0.293 |
| Infectious | 0.506 | 0.259 | 0.724 | 0.449 | 0.710 | 0.195 |
| Cardiovascular |
|
|
|
| 0.927 |
|
| Other | 0.596 |
| 0.159 |
| 0.215 |
|
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsSepsis Diagnosis and Treatment · Venous Thromboembolism Diagnosis and Management · Acute Ischemic Stroke Management
Introduction
The ability to quantify the risk of in-hospital mortality for patients with critical illness may result in cost savings and improvement of resource allocation [1]. The clinical presentation of patients with pulmonary embolism (PE) varies, from asymptomatic to complete cardiovascular collapse [2], and a large proportion of patients with PE require admission to the intensive care unit (ICU). Several PE-specific scores have been developed for predicting mortality in patients who present to the hospital with PE (i.e., primary PE), namely, the Pulmonary Embolism Severity Index (PESI) [3], simplified PESI (sPESI) [4], and ICU-modified sPESI (ICU-sPESI), specifically designed to improve prediction of mortality in critically ill patients [5, 6]. Details of the individual score components were provided in our earlier communication [5]. In the recent Biomolecules and Biomedicine report [6], we evaluated the predictive performance of these PE-specific tests for critically ill patients who were admitted to the ICU for an indication other than PE, but subsequently developed PE (i.e., secondary PE), and demonstrated that these tests had reduced accuracy compared to their predictions for primary PE [5, 6]. Since secondary PE in our previously reported cohort [6] occurred for a wide range of primary ICU admission diagnoses, we hereby explore whether the predictive performance differs depending on admission indications. The performance of PE-specific mortality risk scores was compared to the Acute Physiology and Chronic Health Evaluation-IV (APACHE-IV) score, which represents a gold standard for the prediction of all-cause mortality in ICU patients [7, 8].
Materials and methods
For the full details on data source, cohort selection, data extraction, and processing, we refer the reader to our comprehensive description in our prior publication [6]. Briefly, using the eICU Collaborative Research Database (eICU-CRD) for 2014 and 2015 [9, 10], we identified 812 patients admitted to ICU with various indications (admissions unrelated to PE) and who were subsequently diagnosed with a secondary PE within 48 h after admission. These patients were classified into four broad categories according to the admission indications: a) post-operative, b) cardiovascular (non-surgical), c) infectious (e.g., most frequently sepsis), and d) any other indications (Table 1). The predictive accuracy of the APACHE-IV and three PE-specific risk-scores (PESI, sPESI, and ICU-sPESI) were compared using the area under the receiver operating characteristic curve (AUROC) [11]. AUROCs were descriptively interpreted as follows: AUROC ≥0.9 was considered excellent, ≥0.8 to <0.9 good, ≥0.7 to <0.8 fair, ≥0.6 to <0.7 poor, and <0.6 non-discriminatory [12, 13]. Statistical analyses were performed with Python v.3.9 (Python Software Foundation, Wilmington, Delaware, USA).
Results
Table 1 provides an overview of the four categories of admission indications and their overall in-hospital mortality rates, as well as examples of individual admission diagnoses. Overall, mortality was similar in all categories, with intersecting confidence intervals, highest for cardiovascular (21.5%, 95% CI [16.0%–27.0%]), and lowest for other admissions (16.1%, 95% CI [11.8%–20.5%]). Median [IQR] APACHE-IV, PESI, sPESI, and ICU-sPESI scores for the admission categories are shown in Table 2. Compared to survivors, non-survivors had higher risk scores regardless of admission category. AUROC analyses according to admission indication are detailed in Figure 1 and Table 3. In particular, the sPESI performed poorly for postoperative, infectious, and “other” admissions and had a non-discriminatory performance for cardiovascular admissions. In addition, cardiovascular admissions displayed the largest difference between the APACHE-IV and the PE-specific risk scores, with better performance noted for APACHE-IV compared to PE-specific scores (APACHE-IV vs PESI, P ═ 0.018; APACHE-IV vs sPESI, P < 0.001, APACHE-IV vs ICU-sPESI, P ═ 0.033). Despite the similar overall mortality, all scores, including the APACHE-IV, performed worse for infectious admissions (fair for APACHE-IV, AUROC ═ 0.706, and poor for PESI, sPESI and ICU-sPESI, AUROCs 0.673, 0.637, 0.687, respectively). Notably, by adding only three binary variables to the sPESI for calculating the ICU-sPESI, this modified score performed similarly well in comparison to the more complex PESI score across all admission indications.
Receiver operating characteristic curves for the different subgroups of primary ICU admission diagnoses. APACHE-IV: Acute Physiology and Chronic Health Evaluation-IV; AUROC: Area under the receiver operating curve; ICU: Intensive care unit; PESI: Pulmonary Embolism Severity Index score; sPESI: Simplified PESI; ICU-sPESI: ICU-modified sPESI.
Discussion
We examined four mortality prediction scores and demonstrated their different discriminative ability to predict in-hospital mortality of secondary PE depending on the primary admission indication. In patients with secondary PE, APACHE-IV was a better prognosticating instrument than the three PE-specific prediction scores regardless of the nature of ICU admission. The discriminatory ability of the PESI and ICU-sPESI was still within the acceptable range for postoperative, cardiovascular, and other admissions, but was less accurate for infectious admissions. Better performance of APACHE-IV compared to the PE-specific scores is likely related to the APACHE-IV covering a wide range of differentially weighted clinical variables integrated into complex algorithms [8]. In contrast, the simpler PE-specific scales were designed to include signature features associated with primary PE and these relatively focused inclusion criteria are likely responsible for the observed reduction of predictive precision after secondary PE. It is important to note that when the ICU admission was related to infection, all four scores underperformed. This may be expected because sepsis represents a systemic, multi-etiological disorder with a wide variability of clinical presentations and unpredictable responses to treatment. Furthermore, mortality prediction scores are typically built by collecting clinical variables early and in a relatively short timeframe (e.g., APACHE-IV variables are collected within the first 24 hours of admission). In contrast, sepsis can change its clinical course rapidly, progressing from mild to severe over a short period of time, thus being improperly represented. All this renders the prediction of mortality from sepsis more difficult, even for a score as comprehensive as the APACHE-IV. Consistent with this finding, several previous studies demonstrated that the ability of general scoring systems to predict outcomes in septic patients is frequently unreliable compared to diseases that affect specific organ systems [14–16].
Conclusion
In our study, APACHE-IV had the best ability to predict all-cause in-hospital mortality in critically ill patients with a secondary PE. However, PESI and ICU-sPESI still offered a fair predictive ability for postoperative, cardiovascular, and other admission indication categories. In contrast, sPESI displayed a poor performance throughout. Notably, discriminatory performance for patients with an infectious admission indication was low regardless of which score was used. More studies are needed to improve the accuracy of outcome prediction scores; however, as stated decades ago by Becker and Zimmerman [17], “even with the highest degree of precision, such predictions are only useful in support of, and not as a substitute for, good clinical judgment.”
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Berge KH Maiers DR Schreiner DP Jewell SM Bechtle PS Schroeder DR Resource utilization and outcome in gravely ill intensive care unit patients with predicted in-hospital mortality rates of 95% or higher by APACHE III scores: the relationship with physician and family expectations Mayo Clin Proc 200580216673 https://doi.org/10.4065/80.2.1661570477010.4065/80.2.166 · doi ↗ · pubmed ↗
- 2Corrigan D Prucnal C Kabrhel C Pulmonary embolism: the diagnosis, risk-stratification, treatment and disposition of emergency department patients Clin Exp Emerg Med 20163311725 https://doi.org/10.15441/ceem.16.1462775262910.15441/ceem.16.146PMC 5065342 · doi ↗ · pubmed ↗
- 3Aujesky D Obrosky DS Stone RA Auble TE Perrier A Cornuz J Derivation and validation of a prognostic model for pulmonary embolism Am J Respir Crit Care Med 2005172810416 https://doi.org/10.1164/rccm.200506-862OC 1602080010.1164/rccm.200506-862OCPMC 2718410 · doi ↗ · pubmed ↗
- 4Jimenez D Aujesky D Moores L Gomez V Lobo JL Uresandi F Simplification of the pulmonary embolism severity index for prognostication in patients with acute symptomatic pulmonary embolism Arch Intern Med 20101701513839 https://doi.org/10.1001/archinternmed.2010.1992069696610.1001/archinternmed.2010.199 · doi ↗ · pubmed ↗
- 5Ryll MJ Zodl A Weingarten TN Rabinstein AA Warner DO Schroeder DR Predicting hospital survival in patients admitted to ICU with pulmonary embolism J Intensive Care Med 20243945564 https://doi.org/10.1177/088506662312128753796455110.1177/08850666231212875 PMC 10935623 · doi ↗ · pubmed ↗
- 6Ryll M, Weingarten T, Darrell R.Schroeder D, Sprung J. Validity of mortality risk prediction scores in critically Ill patients with secondary pulmonary embolism. Biomol Biomed Online ahead of print. 10.17305/bb.2024.10202 PMC 1129323338421722 · doi ↗ · pubmed ↗
- 7Ko M Shim M Lee SM Kim Y Yoon S Performance of APACHE IV in medical intensive care unit patients: comparisons with APACHE II, SAPS 3, and MPM(0) III Acute Crit Care 201833421621 https://doi.org/10.4266/acc.2018.001783172388810.4266/acc.2018.00178 PMC 6849024 · doi ↗ · pubmed ↗
- 8Zimmerman JE Kramer AA Mc Nair DS Malila FM Acute Physiology and Chronic Health Evaluation (APACHE) IV: hospital mortality assessment for today’s critically ill patients Crit Care Med 20063451297310 https://doi.org/10.1097/01.CCM.0000215112.84523.F 01654095110.1097/01.CCM.0000215112.84523.F 0 · doi ↗ · pubmed ↗