Paediatric Splenic Abscess Due to Salmonella
Kemal Buğra Memiş, Zeynep Betul Deve, Sonay Aydın

Abstract
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
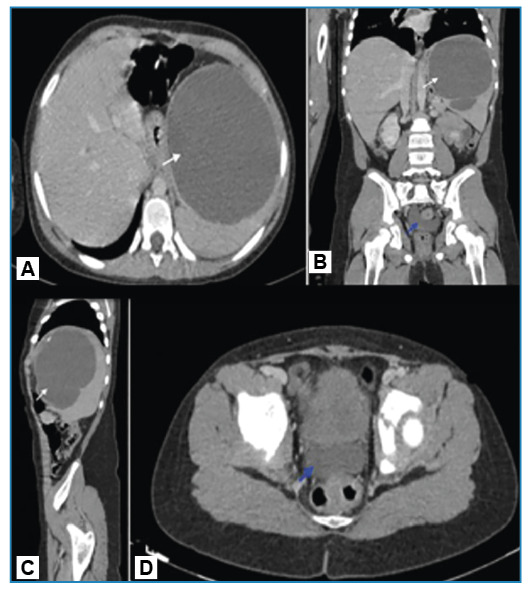 Figure 1
Figure 1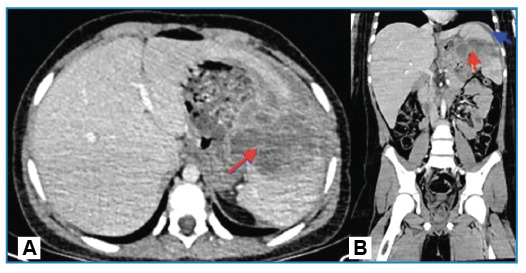 Figure 2
Figure 2Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsSalmonella and Campylobacter epidemiology · Abdominal Trauma and Injuries · Abdominal vascular conditions and treatments
A 12-year-old boy presented to the emergency department with upper left quadrant abdominal pain, fever, and vomiting for three days. He had a fever of 38.5 °C. Test results revealed an elevated white blood cell count and C-reactive protein level.
Computed tomography (CT) revealed a thick-walled cystic lesion measuring approximately 11 cm across the spleen. The patient experienced septation and wall calcification on the upper side. A 2-cm depth of pelvic free fluid was also found (Figure 1). Percutaneous drainage and an 8-day antibiotic regimen were administered, and Salmonella type B was cultured from the abscess. The symptoms improved, leading to discharge. Follow-up CT revealed a 7 × 5-cm septate collection area extending into the splenogastric recess, compressing the stomach’s greater curvature and causing inflammatory wall thickening with perisplenic free fluid, suggestive of a hematoma (Figure 2). Following discharge, the hematoma, which was monitored using ultrasonography in our radiology department, was completely absorbed.
FIGURE 1:Axial- (A), coronal- (B) and sagittal**-**plane (C) abdominal CT showing a thick-walled hypodense cystic lesion approximately 11 cm in diameter in the spleen, with septations and wall calcification in the superior aspect (white arrows); axial- (D) and coronal-plane (B) abdominal CT showing free fluid of approximately 2 cm depth in the pelvic area (blue arrow).
FIGURE 2:Axial- (A) and coronal-plane (B) CT images of a hematoma occurring in the perisplenic region one month after the drainage. 7x5-cm septated and wall-enhancing collection area, extending into the splenogastric recess (red arrows); free fluid measuring 15 mm in depth in the perisplenic space (blue arrow).
Splenic abscesses are rare in children and are associated with high mortality rates. The reported incidence in autopsy series ranges from 0.14%-0.7%1. Symptoms such as fever and abdominal pain are nonspecific. Increased imaging allows for early diagnosis, which is crucial. Aerobic microorganisms, including staphylococci, streptococci, salmonella, and Escherichia coli, are common2. Percutaneous drainage, preferred over surgery, yields 51-72% success rates under specific conditions, replacing traditional antibiotic therapy and splenectomy3 ^,^ 4. This case highlights the importance of considering splenic abscesses in the differential diagnosis of children presenting with nonspecific symptoms such as fever and abdominal pain.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Faruque AV Qazi SH Arshad M Anwar N Isolated splenic abscess in children, role of splenic preservation Pediatr Surg Int 20132987877902381193510.1007/s 00383-013-3336-2 · doi ↗ · pubmed ↗
- 2Liu YH Liu CP Lee CM Splenic abscesses at a tertiary medical center in Northern Taiwan J Microbiol Immunol Infect 20144721041082321840610.1016/j.jmii.2012.08.027 · doi ↗ · pubmed ↗
- 3Qu J Zong Z Giant splenic cyst complicated by infection due to Salmonella enterica serovar Livingstone in a previously healthy adolescent male: a case report BMC Infect Dis 20222215575573571714310.1186/s 12879-022-07529-6PMC 9206239 · doi ↗ · pubmed ↗
- 4Thanos L Dailiana T Papaioannou G Nikita A Koutrouvelis H Kelekis DA Percutaneous CT-guided drainage of splenic abscess AJR Am J Roentgenol 200217936296321218503210.2214/ajr.179.3.1790629 · doi ↗ · pubmed ↗