Case Reports: Presumable tuberculous mastitis-like
Michel de Araujo Tavares, Marcelo Cordeiro dos Santos, Vinicius da Silva Monteiro, Djane Baia-da-Silva, Marcus Vinícius Guimarães de Lacerda, René Aloisio da Costa Vieira

TL;DR
This paper presents 15 cases of women with confirmed or presumed tuberculous mastitis, highlighting the challenges in diagnosis and treatment.
Contribution
The study emphasizes the importance of considering presumptive tuberculous mastitis based on clinical and radiological suspicion.
Findings
4% of cases were confirmed tuberculous mastitis, and 8% were presumed tuberculous mastitis.
There were no significant differences between confirmed and presumed cases except for follow-up and treatment duration.
P-TM should be considered when clinical and radiological signs suggest it.
Abstract
Tuberculous mastitis (TM) is a rare cause of breast disease. The test sensitivity for TM is low and sometimes characterized by idiopathic granulomatous mastitis. Both have different treatments; however, many patients are treated with presumptive TM (P-TM). We present fifteen women with confirmed TM or P-TM. We found 4% (5/124) of TM and 8% (10/124) of P-TM, grouped according to their diagnosis, with no differences between them, except for follow-up and treatment time. P-TM is an entity that must be considered based on clinical and radiological suspicion and is associated with presumptive pathological data.
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
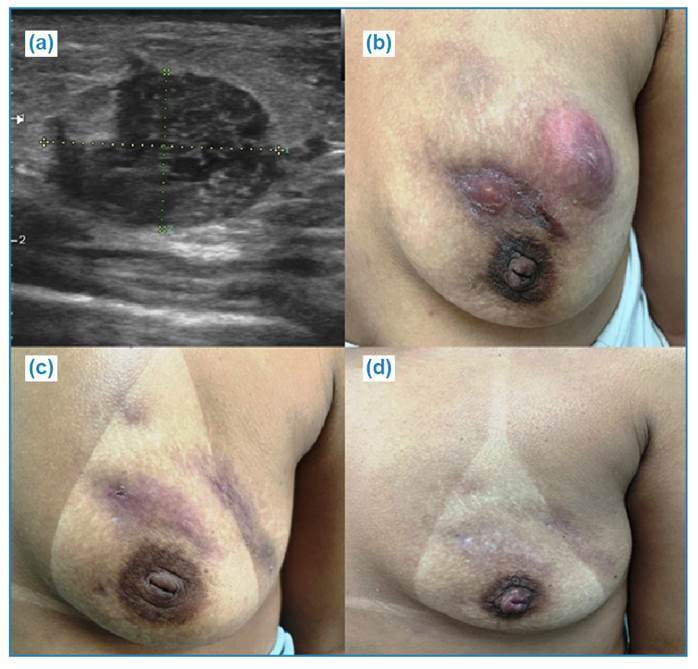 Figure 1
Figure 1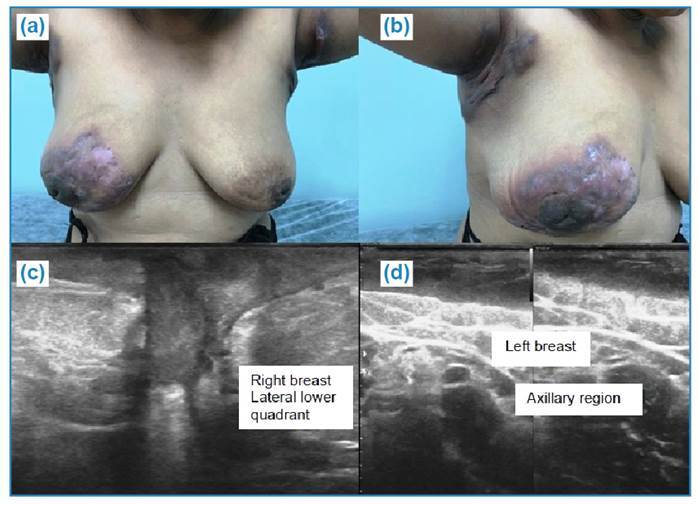 Figure 2
Figure 2Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsBreast Lesions and Carcinomas · Mycobacterium research and diagnosis · Infectious Diseases and Tuberculosis
INTRODUCTION
One third of the world's population has had contact with Mycobacterium tuberculosis, which causes tuberculosis (TB). TB is more common in developing countries, with 22 countries accounting for 80% of the affected individuals; Brazil ranks 16th in incidence. Tuberculous mastitis (TM) is a rare, but an important cause of breast infections that are difficult to diagnose1. The incidence of TM ranges from 0.1% in developed countries to approximately 4% in highly TB endemic countries2. In the Amazon, where TB is endemic, there has been only one TM report3. Patients with mastitis are usually treated with antibiotic therapy, and among those without resolution, TM should be differential. The sensitivity of tests for the diagnosis of TM is low (approximately 12% for M. tuberculosis culture, the gold standard technique), and the histological diagnosis is idiopathic granulomatous mastitis (IGM)4 ^,^ 5. Both have different treatments; however, many patients are treated with presumptive TM (P-TM). We present the clinical aspects and outcomes of 15 women with confirmed TM or P-TM-treated who showed a clinical response at Fundação de Medicina Tropical Doutor Heitor Vieira Dourado, a reference service for infectious diseases in the Brazilian Amazon, located in Manaus, Amazonas, between 2013 and 2021. We defined antituberculosis therapeutic response as a diagnostic criterion.
Clinical, laboratory, and radiological data were obtained from the electronic medical records (iDoctor system). For the etiological diagnosis of TM, we consider the results of multiple procedures: fine needle aspiration; core needle biopsy (CNB); and laboratory tests, such as the purified protein derivative (PPD) skin test, Ziehl-Neelsen (ZN) staining, culturing, polymerase chain reaction, Xpert MTB RIF rapid molecular test (RMT), bacilloscopy (acid fast bacilli -AFB BAAR), histopathological evaluation, culture for identification of mycobacterium and aerobic bacteria, direct examination, and culture of fungi. For P-TM, the following were considered: (1) clinical mastitis, which is difficult to resolve with usual therapies; (2) PPD skin test positivity; (3) histology suggestive of IGM or nonspecific chronic mastitis; and (4) absence of recurrence during a minimum follow-up period of six months after treatment.
CASE REPORT
One hundred and twenty-four patients with IGM were identified throughout the study period: 5 and 10 were diagnosed with TM and P-TM, respectively. The clinical, laboratory, and radiological characteristics of the evaluated women are shown in Table 1. The average age among those diagnosed with TM was 35.4 (range: 22-50), while the average age among those with P-TM was 35.1 (range: 24-62). None of the patients were diagnosed with HIV; however, patients 1, 2, and 3 previously had TB. Most patients complained of pain, heat, breast erythema, breast lumps, and fistulous disease. Fever, chills, and axillary adenopathy were the most common systemic complaints. All patients had positive PPD (induration equal to or greater than 5 mm). Among the five patients with TM, only one had a bacteriologically confirmed positive culture. Altered mammography findings were nonspecific, and the ultrasound findings were highlighted. The ultrasonographic findings were more expressive. Six patients had abscesses and six had fistulas. The most common findings were fistulas, abscesses, circumscribed nodules, hypoechoic nodules, and skin thickening (Figures 1 and 2). Magnetic resonance imaging and chest computed tomography were performed for only one patient and no specific findings were observed. We grouped the individuals according to their diagnosis of TM and P-TM and found no differences between the groups, except for the follow-up and treatment time, which were shorter in the TM group, as expected (Supplementary Table 1), given the need for minimal follow-up and no recurrence.
TABLE 1:Clinical, laboratory, and radiological aspects per case.IDMastitis classificationAgeLocal symptomsSystemic symptomsRadiological aspects HistologyCriteriaPPD (induration in mm)Time of treatment (months)Time of follow-up time (months)Ultrasound1TM22Pain, erythema, papillary discharge, nodule/mass, and fistulaFever and chills, axillary lymph nodesAbscess and fistula NPAFB positive in respiratory sample NP6.28.08Sclerosant2TM41Pain, erythema, papillary discharge, and nodule/massFever and chills Circumscribed hypoechoic noduleICM (ZN+)AFB positive in respiratory sample NP8.81.66Nodular3TM24Pain, erythema, papillary discharge, nodule/mass, and fistulaAxillary adenopathy Abscess and fistula GCMcPPD, lung TB and GCM136.04.39Nodular4TM50Pain, erythema, papillary discharge, and abscessFever and chillsHypoechoic noduleGCMc (ZN+)PPD, Biopsy 86.00.01Nodular5TM40Pain, erythema, papillary discharge, nodule/mass, and abscessAxillary adenopathyCircumscribed hypoechoic noduleICMPositive culture NP9.03,89NP6P-TM39Erythema, papillary discharge, and nodule/mass Fever and chills, axillary adenopathyAbscess, irregular hypoechoic nodule, architectural distortionGCMPPD and GCM258.024.17Nodular7P-TM62Pain, erythema, nodule/mass, and abscessAxillary adenopathyFistula and skin thickeningICMPPD219.39.91Diffuse8P-TM26Pain, erythema, nodule/mass, and abscessFever and chillsCircumscribed hypoechoic nodule and axillary adenopathy.GCMPPD and GCM126.06.66Nodular9P-TM41Pain, erythema, nodule/mass, and fistulaFever and chillsFistulaGCMcPPD, GCM, IGRA 256.014.1Sclerosant10P-TM29Pain, erythema, nodule/mass, and fistula-AbscessGCMPPD and GCM149.015.11Nodular11P-TM34Pain, erythema nodule/mass, and fistulaFever and chills, axillary adenopathyConfluent nodulesICMPPD199.118.47Nodular12P-TM33Pain, erythema, and papillary discharge Abscess and axillary adenopathyICMPPD 188.36.01Diffuse13P-TM24Pain, erythema, papillary discharge, abscess and fistulaFever and chillsAbscess and axillary adenopathyICMPPD179.06.03Sclerosant14P-TM29Pain, erythema, papillary discharge, abscess and fistula-FistulaICMPPD and CT1510.18.78Diffuse15P-TM34Pain, erythema, and fistula-Fistula GCMPPD and GCM57.126.06Nodular AFB: acid-fast bacilli; IGRA: interferon gamma release assay; TM: tuberculous mastitis; P-TM: presumable-tuberculous mastitis; GCMc: caseous granulomatous chronic mastitis; GCM: granulomatous chronic mastitis; ICM: non-specific chronic mastitis; CT: computed tomography; NP: not performed; PPD: purified protein derivative; ZN: Ziehl-Neelsen stain; TB: Tuberculosis. Lung TB was diagnosed by lung biopsy.
FIGURE 1:Patient with a presumed diagnosis of breast tuberculosis. a) Breast ultrasound showing a solid hypoechoic nodule with circumscribed margins in the left breast. b) Left breast showing abscesses, scars, and fistulas in the sixth week of treatment for breast tuberculosis. c) Left breast showing abscesses, scars, and fistulas on the third month of treatment for breast tuberculosis. d) Left breast showing clinical improvement 10 months after starting treatment.
FIGURE 2:Patients in the third month of treatment for bilateral mammary and lymph node tuberculosis. a) and b) Images of the breast and axillary regions with scars, fistulas, erythema, and skin thickening. c) Breast ultrasonography demonstrating a fistulous path with a collection of thick fluid intermingled in the inferolateral quadrant of the right breast. d) Breast ultrasound showing skin thickening in the left axillary region.
DISCUSSION
TB is common in underdeveloped and developing countries, such as Africa, India, and Pakistan4. In Brazil, TB is endemic to the Amazon, with an estimate is 74.1 per 100,000 inhabitants. In Manaus, the rate is 93.2 per 100,000 inhabitants and is associated with income inequalities that influence health and TB transmission6. Although TB is a common disease in the Amazon region, we found 4% TM and 8% P-TM cases in women treated with idiopathic granulomatous mastitis at a reference hospital for infectious diseases in the Brazilian Amazon. The low frequency of TM can be explained by the diagnostic difficulty, which is generally defined as IGM. The importance of the diagnostic definition is that the treatment differs, since IGM is usually treated with surgery or immunosuppressive drugs, such as corticosteroids and methotrexate, which are harmful if the patient has TM. In addition, it is harmful to the patient undergoing a surgical procedure when there is a treatable etiology of a disease that may be recurrent; therefore, the etiology must be extensively evaluated. However, IGM is treated with immunosuppressants and has a high recurrence rate7. One treatment option for IGM is surgery, including mastectomy. The problem is performing surgery when there is a treatable etiology; therefore, the etiology must be evaluated extensively.
In the present study, the diagnostic method varied according to the medical criteria. However, we adjusted the definitions and re-evaluated the classification of cases. According to medical records, 23 women had TM or P-TM; however, based on a detailed analysis of the kinetics, diagnostic methods used, clinical characteristics, and response to therapy, we found only 15 cases. Diagnostic evaluation is essential, and many of these patients are treated with antibiotic therapy and have persistent or recurrent breast findings4. Patients should be evaluated histologically in the absence of resolution. In the presence of granulomatous lesions, IGM, TM should be considered as differential diagnosis8. The gold standard for the diagnosis of the disease is the detection of the etiologic agent, M. tuberculosis using Ziehl-Neelsen staining or culture. However, AFB smear positivity and ZN staining are not frequently performed. In most cases, breast TB can only be accurately diagnosed using the histological identification of a typical necrotizing granulomatous lesion9. On biopsy, the predominance of neutrophils in the background and relative absence of caseous necrosis favor the diagnosis of granulomatous mastitis. Generally, CNB is sufficient for evaluation, therefore, an open biopsy is rarely necessary10. In TB-endemic areas, the PPD skin test may be positive and related to previous exposure to M. tuberculosis in those vaccinated with the Bacillus Calmette-Guerin vaccine or previous exposure to nontuberculous mycobacteria. It is difficult to distinguish between an old and recent infection; therefore, the PPD skin test lacks diagnostic value11. In our study, almost all patients treated for TM showed elevated skin test results.
The Brazilian study included 20 cases, of which 19 women had IGM with caseous necrosis and the ZN test was positive in only one patient. All the patients had high PPD levels. The patients were treated for six months, with a mean follow-up of 12 months (8-14 months), and no recurrence was observed12. Despite having 15 patients (five with TM and 10 with P-TM), our study constitutes one of the largest Brazilian studies influenced by the endemic area and treatment in specific treatment centers. PPD values and follow-up times were similar.
This study had some limitations, particularly those associated with the study design. However, it represents the second largest sample in Brazil and originates from an endemic region. The lack of positivity criteria for all patients was overcome by the response to therapy and the six-month follow-up of patients with P-TM. This study aimed to establish the criteria based on the presence of a therapeutic response.
In conclusion, standardizing diagnostic tests can increase the positivity rate for TM. P-TM must be considered based on clinical and radiological suspicion, associating presumptive pathological data with examinations that indirectly suggest exposure to TB. Among the treated patients, the anti-TB therapeutic response must be considered, and one of the criteria for the final diagnosis is the response to long-term therapy.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Ramaema DP Buccimazza I Hift RJ Prevalence of breast Tuberculosis: retrospective analysis of 65 patients attending a tertiary hospital in Durban, South Africa S Afr Med J 2015105108668692642859510.7196/SAM Jnew.7704 · doi ↗ · pubmed ↗
- 2Sabageh D Amao EA Ayo-Aderibigbe AA Sabageh AO Tuberculous mastitis simulating carcinoma of the breast in a young Nigerian woman: a case report Pan Afr Med J 20152112512510.11604/pamj.2015.21.125.633626327962 PMC 4546730 · doi ↗ · pubmed ↗
- 3Bianco SR Gurgel RL Tavares MA Radiological aspects of primary Tuberculosis in the breast: a case report and review of the literature Rev Soc Bras Med Trop 200542220320510.1590/s 0037-8682200900020002219448943 · doi ↗ · pubmed ↗
- 4Grover H Grover SB Goyal P Hegde R Gupta S Malhotra S Clinical and imaging features of Idiopathic Granulomatous Mastitis - The diagnostic challenges and a brief review Clin Imaging 2021691261323271754010.1016/j.clinimag.2020.06.022 · doi ↗ · pubmed ↗
- 5Gupta PP Gupta KB Yadav RK Agarvval D Tuberculous mastitis: A review of seven consecutive cases Ind J Tub 20035014750
- 6Teixeira R Rodrigues MGA Ferreira MD Borges MC Safe I Melo GC Tuberculosis and malaria walk side by side in the brazilian Amazon: an ecological approach Trop Med Int Health 2019248100310103123367110.1111/tmi.13282 · doi ↗ · pubmed ↗
- 7Mohammed S Statz A Lacross JS Lassinger BK Contreras A Gutierrez C Granulomatous Mastitis: a 10 year experience from a large inner city county hospital J Surg Res 201318412993032389040110.1016/j.jss.2013.06.047 · doi ↗ · pubmed ↗
- 8Maione C Palumbo VD Maffongelli A Damiano G Buscemi S Spinelli G alet Diagnostic techniques and multidisciplinary approach in Idiopathic Granulomatous Mastitis: a revision of the literature Acta Biomed 2019901111510.23750/abm.v 90i 1.6607 PMC 650216730889150 · doi ↗ · pubmed ↗