Transthoracic echocardiography-guided PBMV for severe rheumatic mitral stenosis with pregnancy
Hao Xiao, Pan Xiangbin, Hu Haibo

Abstract
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
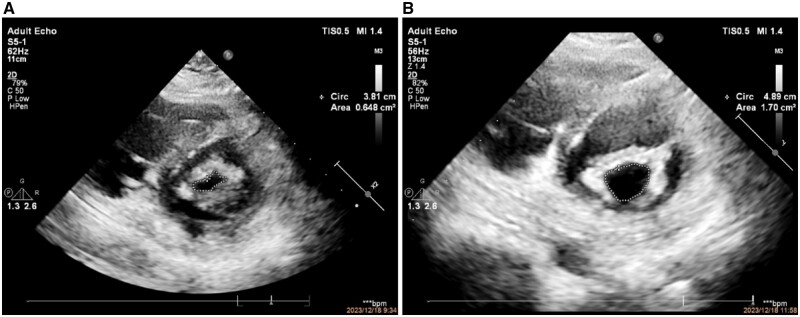 Figure 1
Figure 1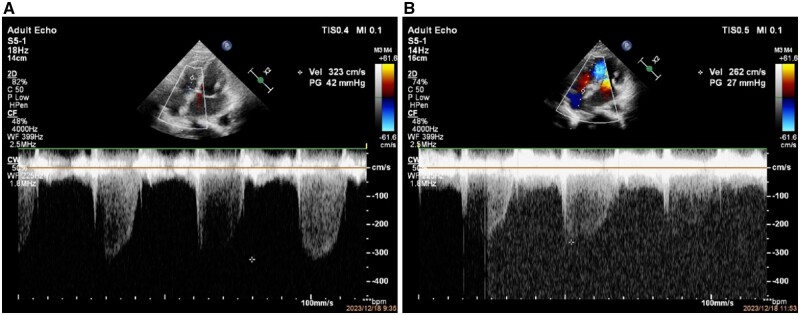 Figure 2
Figure 2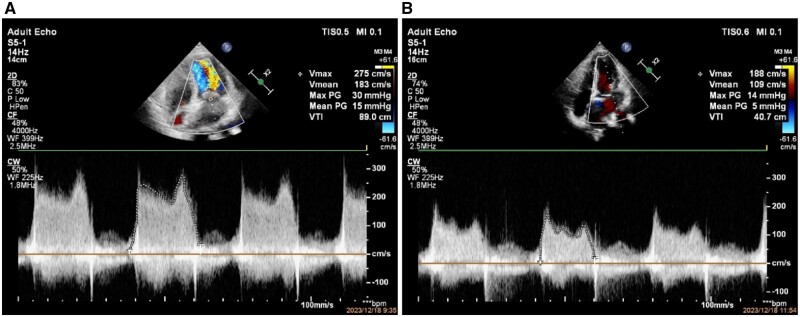 Figure 3
Figure 3Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsCardiac Valve Diseases and Treatments · Cardiovascular Issues in Pregnancy · Cardiac Structural Anomalies and Repair
Background
The currently invasive strategies for mitral valve stenosis include percutaneous balloon mitral valvuloplasty (PBMV) and surgical replacement. Most PBMV procedures are guided by fluoroscopy.1–3 For some patients, such as pregnancy, the use of radiation may have an impact on the fetus. We report a case of PBMV guided by transthoracic-echocardiography.
Case summary
The patient is a 29-year-old female with 15 weeks of pregnancy. She experienced shortness of breath for 1 month after physical activity, accompanied by decreased activity endurance. Pre-procedure examination of the apex of the heart revealed open valve sounds and 4/6 level diastolic murmurs accompanied by tremors, radiating to the left axilla. Pre-procedure transthoracic and transesophageal echocardiography showed thickening of mitral valve leaflets, enhanced echogenicity, and mild calcification, resulting in restricted opening. Wilkins scored 6 points.
Due to pregnancy, we consider a procedure guided by transthoracic echocardiography (TTE) under local anesthesia. We chose a 26-mm Inoue balloon (with a diameter of 25 mm after water-injection) for PBMV procedure. After dilation, transthoracic-ultrasound showed improvement in the opening of the mitral valve, with a valve opening area of 1.7 cm^2^ from 0.64-cm^2^ pre-procedure (Figure 1). Pulmonary artery pressure decreased significantly (Figure 2). Mean left atrial pressure was measured at 10 mmHg after dilation (pre-procedure pressure is 39 mmHg), and there was no severe mitral regurgitation (Figure 3). Post-procedure auscultation revealed 2/6 grade rumbling murmurs in the apex area, without tremors or radiation.
Pre-procedure and post-procedure mitral valve diastolic valve opening area (A, a pre-procedure mitral valve opening area of 0.648 cm2 during diastole; B, post-procedure mitral valve diastolic valve opening area of 1.7 cm2).
Pre-procedure and post-procedure tricuspid regurgitation velocity and estimated pulmonary artery systolic pressure (A, pre-procedure tricuspid regurgitation velocity 3.23 m/s, estimated pulmonary artery systolic pressure 42 mmHg; B, post-procedure tricuspid regurgitation velocity 2.62 m/s, estimated pulmonary artery systolic pressure 27 mmHg).
Pre-procedure and post-procedure mitral valve spectrum measurements (A, pre-procedure average mitral valve velocity of 1.83 m/s and average transvalvular gradients of 15 mmHg; B, post-procedure average mitral valve velocity of 1.09 m/s and average transvalvular gradients of 5 mmHg).
Discussion
X-ray-guided PBMV increases the risk of treatment, including X-ray glandular injury, fetal injury, contrast agent allergy, and contrast agent nephropathy. Previous studies have found that ultrasound-guided PBMV, percutaneous closure of atrial septal defects, ventricular septal defects, and patent foramen ovale have all achieved good results.4 In this case, PBMV of mitral valve stenosis under pure ultrasound guidance was more effective than double guidance with X-ray and ultrasound. Both methods significantly reduced transvalvular gradient differences and increased the valve opening area. However, pure ultrasound guidance reduced radiation-related injuries to medical staff and patients.5 Therefore, pure ultrasound guidance,6 especially PBMV guided by TTE, reduces radiation-related damage and can be the preferred guidance method for PBMV.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Koren O , Israeli A, Rozner E, Darawshly N, Turgeman Y. Clinical and echocardiographic trends in percutaneous balloon mitral valvuloplasty. Eur Heart J 2021; 42:1572.10.1186/s 13019-021-01442-w PMC 801768733794935 · doi ↗ · pubmed ↗
- 2Turi ZG. The 40th anniversary of percutaneous balloon valvuloplasty for mitral stenosis: current status. Struct Heart 2022; 6:100087.37288059 10.1016/j.shj.2022.100087 PMC 10242581 · doi ↗ · pubmed ↗
- 3Hellmuth W , Philip H, Francis S, Anton D. Transcatheter heart valve interventions for patients with rheumatic heart disease. Front Cardiovasc Med 2023; 10:1234165.37771665 10.3389/fcvm.2023.1234165 PMC 10525355 · doi ↗ · pubmed ↗
- 4Pan XB , Ou-Yang WB, Pang KJ, Zhang FW, Wang SZ, Liu Y, et al Percutaneous closure of atrial septal defects under transthoracic echocardiography guidance without fluoroscopy or intubation in children. J Interv Cardiol 2015; 28:390–5.26077469 10.1111/joic.12214 · doi ↗ · pubmed ↗
- 5Li YD , Pang KJ, Xu N, Wang H. The application value of simple ultrasound and dual guidance of ultrasound and X-ray in percutaneous intervention treatment of mitral valve stenosis balloon dilation. J Shanxi Med Univ 2021; 52:1001–4.
- 6Islam S , Khan J, Khan S. Balloon mitral valvuloplasty: a re-emerging technique enhanced with real-time, three-dimensional transoesophageal cardiac ultrasound/echocardiography (3D-TOE). BMJ Case Rep 2023; 16. doi:10.1136/bcr-2022-253123.PMC 990626936750298 · doi ↗ · pubmed ↗