Giant Aortic Arch Aneurysm Presenting as Ortner's Syndrome in Polycystic Kidney Disease: A Radiological Perspective
Arvinder Wander, Vandeep S Basra, Tejinder S Malhi, Ramandeep Singh

TL;DR
This paper presents a rare case of a giant aortic arch aneurysm in a patient with polycystic kidney disease, highlighting unusual clinical features.
Contribution
The paper reports a rare case of a giant aortic arch aneurysm in a patient with polycystic kidney disease.
Findings
Giant aortic arch aneurysms are rarely reported in patients with polycystic kidney disease.
The case presented has a unique clinical presentation, adding to the limited literature on this topic.
Abstract
Polycystic kidney disease (PKD) is a genetic disease characterized by the formation of multiple cysts in bilateral kidneys. While renal complications are predominant, cardiovascular manifestations such as aortic aneurysms can also occur. Although there are a few case reports of giant aortic arch aneurysms, to the best of our knowledge, this has been rarely reported in patients with PKD. Additionally, the clinical presentation of the index case is unique.
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
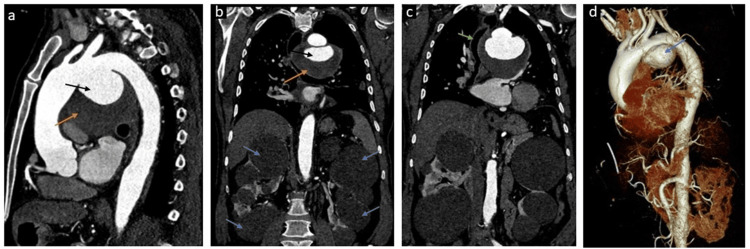 Figure 1
Figure 1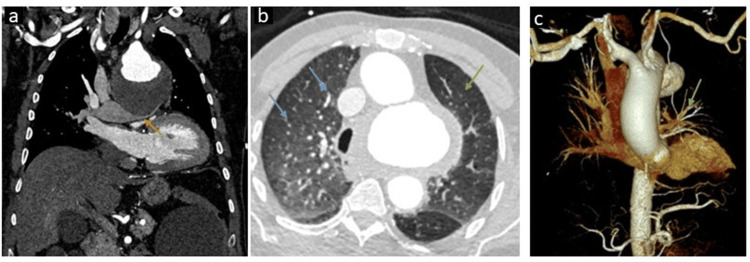 Figure 2
Figure 2| Investigation | Result | Unit | Reference range |
| White blood cells | 6.45 | x103 /μl | 4.00-11.00 |
| RBC | 4.71 | x106 /μl | 3.50-5.50 |
| Hemoglobin | 12.9 | gm/dl | 11.0-16.0 |
| Platelet | 190 | x103 /μl | 150-450 |
| Glycosylated hemoglobin | 5.5 | % | Normal < 5.7; prediabetic 5.7-6.4; diabetic > 6.4 |
| Urea | 60 | mg/dl | 15-45 |
| Creatinine | 1.4 | mg/dl | 0.6-1.10 |
| Cholesterol | 192 | mg/dl | <200 |
| Triglyceride | 148 | mg/dl | <150 |
| Morphological features |
| Total sac dimension (outer surface to outer surface) |
| Patent sac dimension (in case of mural thrombus) |
| Shape: fusiform or saccular |
| Mural characteristics |
| Presence of calcification |
| Presence of mural thrombus |
| Mural thickening |
| Atherosclerotic plaques |
| Location and relationship to aortic arch branches |
| Diameter of aorta proximal and distal to aneurysm |
| Location in terms of anatomical landing zones of aorta |
| Relation of the aneurysm with origins of aortic arch branches |
| Characterization of possible etiology |
| True versus pseudoaneurysm |
| Clue for mycotic aneurysm— adjacent soft tissue stranding, collection |
| Atherosclerotic changes in the aorta |
| Complications |
| Signs of impending rupture |
| Leak |
| Thrombosis |
| Strength of recommendation | Recommendations |
| Strong (benefit >>> risk) | In patients with an aortic arch aneurysm who have symptoms attributable to the aneurysm and are at low or intermediate operative risk, open surgical replacement is recommended. |
| Moderate (benefit >> risk) | In patients with an isolated aortic arch aneurysm who are asymptomatic and have a low operative risk, open surgical replacement at an arch diameter of ≥5.5 cm is reasonable. |
| Weak (benefit >/= risk) | In patients with an aortic arch aneurysm who are asymptomatic but meet criteria for intervention, but have a high risk from open surgical repair, a hybrid or endovascular approach may be reasonable. |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsAortic aneurysm repair treatments · Renal and Vascular Pathologies · Abdominal vascular conditions and treatments
Introduction
Autosomal dominant polycystic kidney disease (ADPKD) is an inherited disease characterized by the formation of multiple cysts in bilateral kidneys and less commonly in the liver, pancreas, and spleen [1]. As polycystin has been demonstrated to support the preservation of arterial integrity, various vascular abnormalities such as intracranial aneurysms, aortic aneurysms, and dissection of the coronary and vertebral arteries are associated with ADPKD [2].
Aortic arch aneurysms are uncommon and account for <10% of thoracic aortic aneurysms [3]. This article delineates an unusual scenario where a PKD-diagnosed individual manifested pressure symptoms due to a giant aortic arch aneurysm. To the best of our knowledge, giant aortic arch aneurysm is rarely reported in PKD patients.
Case presentation
A 58-year-old male with a known case of PKD presented with a change in voice and dysphagia for three months. He also complained of progressively worsening dyspnea on exertion and occasional chest discomfort for the past two months. He was hypertensive, which was fairly controlled on two antihypertensive drugs, namely telmisartan and amlodipine. He was a non-smoker and non-diabetic. Family history revealed PKD in his younger brother with no known cardiovascular disorders. Peripheral pulses were normal. Blood pressure was 140/96 mmHg in both arms. Cardiac auscultation revealed normal S1 and S2 heart sounds with no murmurs. Blood investigations (Table 1) such as complete blood count and lipid profile were normal except for mildly raised serum creatinine levels (1.4 mg/dL). The patient was referred to an ear, nose, and throat (ENT) surgeon for a laryngoscopy, which revealed left vocal cord palsy; however, no laryngeal growth was noted.
Imaging
Chest X-ray showed a large mediastinal opacity in the upper and mid-zones, causing right-sided tracheal shift. There was also gross enlargement of the aortic knob. Contrast-enhanced computed tomography (CECT) chest with aortogram was ordered to confirm the diagnosis. A contrast-enhanced computed tomography (CT) angiogram demonstrated a large saccular aneurysm arising from the inferior surface of the aortic arch, extending from the origin of the left common carotid artery to the descending thoracic aorta. It was partially thrombosed with a maximum external diameter of 9.5 cm and a maximum internal diameter of 6.8 cm (Figure 1).
Computed tomography angiograms demonstrating a giant aortic arch aneurysm in polycystic kidney disease patient(A) Sagittal image demonstrating a large aneurysm from the inferior surface of the arch of aorta (black arrow) and large intramural thrombus (orange arrow). (B) Coronal image demonstrating the same (black and orange arrows) and multiple variable-sized bilateral simple renal cortical cysts (blue arrows). (C) Coronal image showing rightward tracheal shift (green arrow) due to mass effect by the aneurysm. (D) 3D virtual rendering technique (VRT) image demonstrating aortic arch aneurysm (blue arrow).
The aneurysm was causing severe compression on the left pulmonary artery with resultant relative pulmonary oligemia on the left side (Figure 2).
Computed tomography demonstrating the mass effect on the left main pulmonary artery with resultant pulmonary oligemia(A) Coronal image demonstrating severe compression of the left main pulmonary artery (yellow arrow) by the giant aortic arch aneurysm. (B) Axial image in lung window at the level of bilateral upper lobes showing a reduced caliber of the segmental and subsegmental pulmonary arteries, with resultant hyperlucent left lung parenchyma suggesting oligemia (green arrow). Note the normal-sized right upper lobe segmental and subsegmental pulmonary arteries (blue arrows). (C) 3D virtual rendering technique (VRT) image demonstrating a marked reduction in the size of the left pulmonary vasculature (green arrow) at the level of the hilum due to compression of the left main pulmonary artery.
There was significant compression on the mid-thoracic esophagus and left recurrent laryngeal nerve. The trachea was shifted toward the right side; however, no significant luminal narrowing was seen. There was no evidence of significant atherosclerotic changes in the aorta and its branches. A note was made of multiple large simple cysts in bilateral kidneys. No aneurysm of coronary arteries or abdominal aorta or its branch was seen. Time of flight MR angiography of the brain revealed no intracranial aneurysm. CT reporting template for aortic arch aneurysm is shown in Table 2.
Outcome and follow-up
Given the size and location of the aneurysm, surgical intervention was deemed necessary. Hence, the patient was advised for surgical management of the aneurysm, but he refused at that time. However, he presented again after one month with acute chest pain, and, unfortunately, succumbed to acute aortic syndrome before any further management could be initiated.
Discussion
PKD predisposes patients to various cardiovascular complications, including intracranial aneurysms, mitral valve prolapse, and aortic aneurysms. The exact pathogenesis is unclear, but it is believed to be multifactorial gameplay involving genetic and hemodynamic factors. The presence of aortic aneurysms is uncommon in ADPKD patients and mostly involves the abdominal aorta [2]. The presence of hoarseness of voice and dysphagia due to the mass effect of giant aortic arch aneurysms in PKD patients makes our case really unique because such a combination has been rarely reported to date. Hoarseness of voice is due to the left recurrent laryngeal nerve compression as it courses adjacent to the aortic arch. Hoarseness occurring in the setting of cardiovascular cause is termed cardiovocal or Ortner's syndrome. This syndrome is associated with many cardiovascular diseases such as mitral valve disease, severe pulmonary hypertension, or congenital diseases [4]. However, it is rarely caused by an aortic aneurysm [4]. Dysphagia in the index cause was the result of compression on the esophagus by the aortic arch aneurysm. Cardiovocal syndrome, together with the presence of dysphagia, dyspnea, and chest pain in patients with aortic arch aneurysm, is a surgical indication for the treatment of aortic aneurysms [5].
Diagnosis of the aortic arch aneurysm was relatively late in the index case posing various clinical and surgical issues and ultimately patient morbidity. This highlights the importance of screening in ADPKD patients for early detection of aneurysms. Though screening for intracranial aneurysms is becoming a common practice in ADPKD patients, screening for aortic and coronary aneurysms is not frequent because they are uncommon. Due to their rarity, screening may not be appropriate for all ADPKD patients, but drawing special attention and timely screening of patients with additional risk factors such as hypertension, age > 60 years, and chest discomfort, might prevent grave prognosis. The other point to note is that the patient was asymptomatic until the last three months despite the large size of the aneurysm; therefore, even asymptomatic elderly patients of PKD may benefit from the screening.
According to the guidelines by the National Institute for Health and Care Excellence, screening for aortic aneurysm is recommended for all men aged 66 years and above or if there is a presence of risk factors such as hypertension. Recommendations for surgical and endovascular management of aortic arch aneurysms are given in Table 3 [5].
Conclusions
This case underscores the importance of recognizing cardiovascular manifestations in patients with PKD. A high index of suspicion, coupled with prompt diagnostic evaluation and multidisciplinary management, can lead to favorable outcomes in complex cases like giant aortic arch aneurysms. Early detection and intervention are paramount due to the increased risk of rupture associated with giant aortic arch aneurysms. Surgical repair remains the mainstay of treatment, although endovascular techniques may be considered in selected cases.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Renal Cystic Disease Stat Pearls [Internet]. Treasure Island, FL: Stat Pearls Publishing 8 2020 Goksu SY Leslie SW Khattar D Treasure Island, FL Stat Pearls Publishing 2020 https://www.ncbi.nlm.nih.gov/books/NBK 554504/32119391 · pubmed ↗
- 2Abdominal aortic aneurysm and autosomal-dominant polycystic kidney disease Kidney Int Takagi H Umemoto T 37667200510.1111/j.1523-1755.2005.091_2.x 15610268 · doi ↗ · pubmed ↗
- 3Natural history of thoracic aortic aneurysms J Vasc Surg Kuzmik GA Sang AX Elefteriades JA 5655715620122284090710.1016/j.jvs.2012.04.053 · doi ↗ · pubmed ↗
- 4Ortner's syndrome: a multifactorial cardiovocal syndrome Clin Cardiol Plastiras SC Pamboucas C Zafiriou T Lazaris N Toumanidis S 010033201010.1002/clc.20646 PMC 665337920552619 · doi ↗ · pubmed ↗
- 52022 ACC/AHA Guideline for the Diagnosis and Management of Aortic Disease: a report of the American Heart Association/American College of Cardiology Joint Committee on Clinical Practice Guidelines Circulation Isselbacher EM Preventza O Hamilton BJ 0482146202210.1161/CIR.0000000000001106 PMC 987673636322642 · doi ↗ · pubmed ↗