Successful gastroduodenal stenting using the endoscopic ultrasound-guided rendezvous technique by Treitz ligament puncture
Shin Yagi, Susumu Hijioka, Kohei Okamoto, Yoshikuni Nagashio, Mark Chatto, Yutaka Saito, Takuji Okusaka

Abstract
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
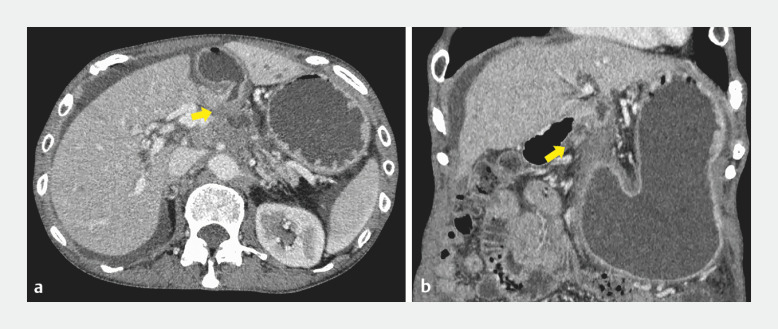 Fig. 1
Fig. 1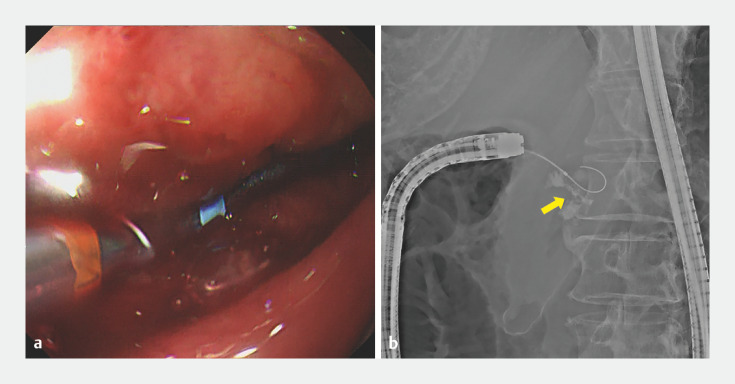 Fig. 2
Fig. 2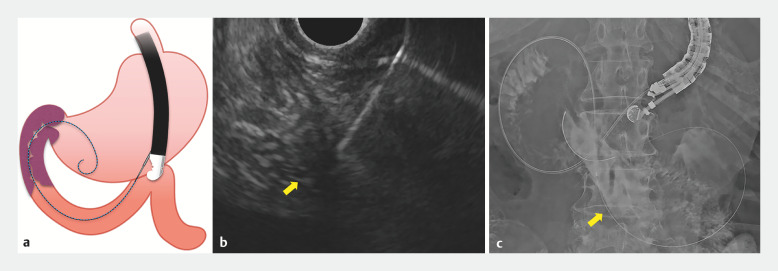 Fig. 3
Fig. 3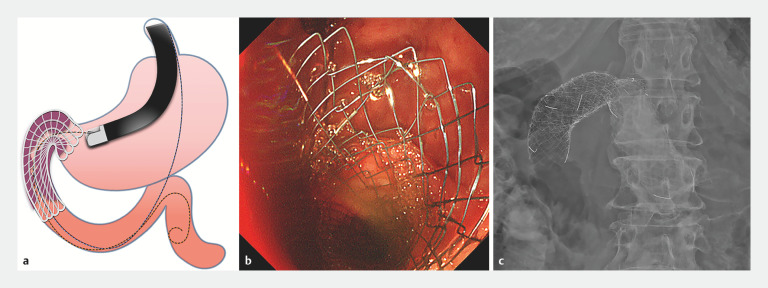 Fig. 4
Fig. 4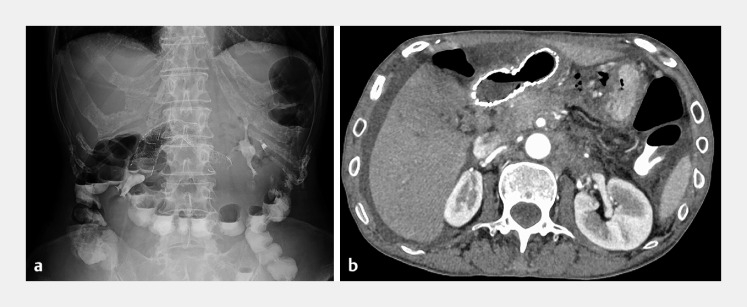 Fig. 5
Fig. 5- —National Cancer Center Research and Development Fund
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsEsophageal and GI Pathology · Gastrointestinal Tumor Research and Treatment · Biliary and Gastrointestinal Fistulas
Endoscopic gastroduodenal stenting is a widely performed treatment for malignant gastric outlet obstruction (GOO); however, occasionally, the guidewire cannot be passed through the stenosis 1 2 3 . Here, we report a case of successful gastroduodenal stenting using the rendezvous technique with endoscopic ultrasound (EUS) for malignant GOO, which we believe to be the first report of gastroduodenal stenting using the rendezvous technique with EUS.
A 60-year-old woman undergoing chemotherapy for pancreatic cancer presented with vomiting. Computed tomography (CT) showed gastric dilatation and stenosis from the gastric pylorus to the duodenal bulb due to pancreatic cancer ( Fig. 1 ). Endoscopic placement of a gastroduodenal stent was attempted, but the guidewire could not be passed through the stenosis ( Fig. 2 ). Therefore, we decided to puncture the Treitz ligament from the stomach using EUS and place a gastroduodenal stent using the rendezvous technique ( Video 1 ). Using EUS, we continuously delineated the descending part of the duodenum to the Treitz ligament from within the stomach, then punctured the Treitz ligament closest to the gastric wall with a 19-gauge needle, and a guidewire was advanced from the duodenum retrogradely through the stenosis into the stomach ( Fig. 3 ). The scope was then changed to a duodenoscope and a guidewire was advanced from the stomach across the stenosis in an antegrade fashion using the rendezvous technique. Two uncovered gastroduodenal stents were placed in series to cover the stenosis ( Fig. 4 ).
Computed tomography scan images showing gastric dilatation and stenosis (arrow) from the gastric pylorus to the duodenal bulb due to pancreatic cancer on: a axial view; b coronal view.
Failed attempts to pass through the stenosis (arrow) using an endoscopic catheter and guidewire are shown on: a endoscopic image; b radiographic image.
Puncture of the Treitz ligament (arrow) from the stomach is shown on: a a schematic image; b endoscopic ultrasound image; c radiographic image, with the retrograde guidewire (arrow) advanced from the duodenum into the stomach.
Successful placement of a gastroduodenal stent using the rendezvous technique with endoscopic ultrasound is shown on: a a schematic image; b endoscopic image; c radiographic image.
A gastroduodenal stent is placed using the endoscopic ultrasound-guided rendezvous technique by puncture of the Treitz ligament.Video 1
A CT scan and abdominal radiograph performed the day after the procedure showed no migration of the gastroduodenal stent and resolution of the GOO ( Fig. 5 ). The patient was able to eat and was discharged 5 days after the treatment, with no adverse events.
Improvement in the gastric dilatation is seen 1 day after gastroduodenal stent placement on: a radiographic image; b computed tomography scan image.
In this case, a gastroduodenal stent was successfully placed using the rendezvous technique with EUS. This method may be useful for cases of malignant GOO in which the guidewire cannot be passed through the stenosis.
Endoscopy_UCTN_Code_TTT_1AS_2AI
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Hamada T Hakuta R Takahara N Covered versus uncovered metal stents for malignant gastric outlet obstruction: Systematic review and meta-analysis Dig Endosc 20172925927110.1111/den.1278627997723 · doi ↗ · pubmed ↗
- 2van Halsema EE Rauws EA Fockens P Self-expandable metal stents for malignant gastric outlet obstruction: A pooled analysis of prospective literature World J Gastroenterol 201521124681248110.3748/wjg.v 21.i 43.1246826604654 PMC 4649130 · doi ↗ · pubmed ↗
- 3Yamashige D Hijioka S Nagashio Y Incidence and factors associated with stent dysfunction and pancreatitis after gastroduodenal stenting for malignant gastric outlet obstruction Endosc Int Open 202412 E 367E 37638464977 10.1055/a-2261-2833 PMC 10919994 · doi ↗ · pubmed ↗