Deep invasive mucinous adenocarcinoma without surface amorphous pattern on inflammatory bowel disease: specific disease with specific characterization
Elena De Cristofaro, Clara Yzet, Louis-Jean Masgnaux, Jean Grimaldi, Jérôme Rivory, Tanguy Fenouil, Mathieu Pioche

Abstract
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
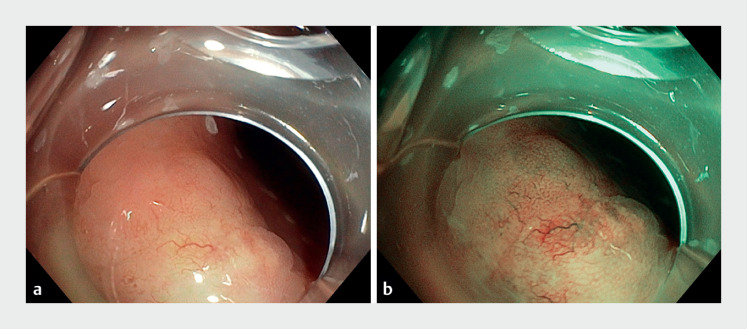 Fig. 1
Fig. 1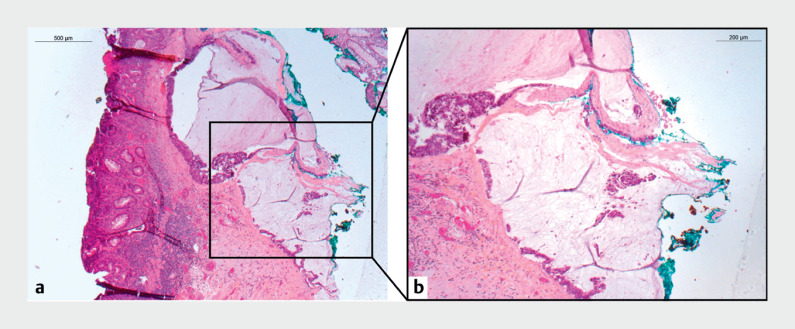 Fig. 2
Fig. 2Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsGastric Cancer Management and Outcomes · Gastrointestinal Tumor Research and Treatment · Colorectal Cancer Screening and Detection
Endoscopic characterization of deep invasive carcinoma using current classifications (CONECCT III, JNET III, NICE III) is effective but was not developed for neoplasias associated with inflammatory bowel diseases (IBDs). In IBD, dysplastic lesions often present as flat, non-granular laterally spreading tumors (LST-NGs) 1 2 . However, mucosal distortion caused by chronic inflammation and regenerative changes can conceal dysplasia, making the detection and characterization of the colonic lesions challenging 3 4 . The present case illustrates that deep invasive adenocarcinoma can occur with very slight mucosal changes in an IBD lesion ( Video 1 ).
Invasive adenocarcinoma in inflammatory bowel disease lesion with slight mucosal changes.Video 1
A 53-year-old woman was referred for endoscopic resection of a 15-mm IBD-related sigmoid lesion (previously diagnosed with high grade dysplasia on biopsy). The lesion was classified as LST-NG with a single and delineated area exhibiting a disorganized pattern ( Fig. 1 ). Endoscopic submucosal dissection (ESD) was indicated to ensure en bloc resection, and an adaptative traction strategy with A-TRACT was employed due to an expected strong fibrosis. The dissection phase proceeded smoothly until reaching the center of the lesion, where a pool of mucus emerged and spread out within the submucosal region. The procedure ended without adverse events facilitated by the use of an adaptative traction device and an underwater strategy during the dissection. The histopathology revealed an adenocarcinoma with submucosal invasion (R1 vertical margins and high risk features) and a mucinous lake within the lesion ( Fig. 2 ).
Non-granular laterally spreading tumor with a single and well-defined area exhibiting a disorganized pattern. a White light endoscopy. b Narrow band imaging.
a Histopathological examination at low power of the endoscopic submucosal dissection specimen found mucosal inflammatory changes admixed with few adenocarcinoma glands invading the lamina propria. They were associated with deep submucosal infiltrating glands floating in mucin pools. b At higher magnification, the neoplastic glands presented typical characteristics of invasive mucinous adenocarcinoma and reached the endoscopic resection margin.
It can be inferred that the whitish cloudy appearance in the submucosa may signal the presence of a mucinous component, implying a deeply invasive lesion with high risk features such as mucinous submucosal invasion. Consequently, it is frequently linked with a non-curative resection and could lead to stopping the dissection during the procedure. The challenge in characterizing IBD lesions should prompt the utilization of progressively advanced endoscopic technologies and techniques to ensure en bloc resection with an accurate histological evaluation.
Endoscopy_UCTN_Code_TTT_1AO_2AG_3AD
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Sugimoto S Naganuma M Iwao Y Endoscopic morphological features of ulcerative colitis-associated dysplasia classified according to the SCENIC consensus statement Gastrointest Endosc 20178563964627884517 10.1016/j.gie.2016.11.013 · doi ↗ · pubmed ↗
- 2Laine L Kaltenbach T Barkun ASCENIC international consensus statement on surveillance and management of dysplasia in inflammatory bowel disease Gastroenterology 20158163965110.1053/j.gastro.2015.01.03125702852 · doi ↗ · pubmed ↗
- 3Rutter MD Saunders BP Schofield G Pancolonic indigo carmine dye spraying for the detection of dysplasia in ulcerative colitis Gut 20045325626010.1136/gut.2003.01638614724160 PMC 1774934 · doi ↗ · pubmed ↗
- 4Vinsard DG Bruining DH East JE Interobserver agreement of modified Paris classification and histology prediction of colorectal lesions in patients with inflammatory bowel disease Gastrointest Endosc 20239779079836402202 10.1016/j.gie.2022.11.006 · doi ↗ · pubmed ↗