Unexpected extraluminal omental bleeding during endoscopic full-thickness resection for a gastric subepithelial lesion
Chaoqin Wang, Suhuan Liao, Silin Huang, Bo Li, Guang Yang, Jianzhen Ren, RenJie Chang

Abstract
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
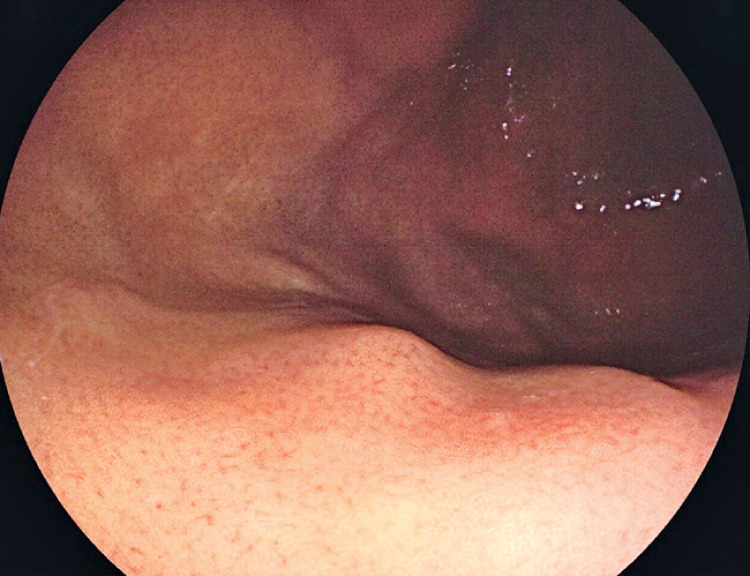 Fig. 1
Fig. 1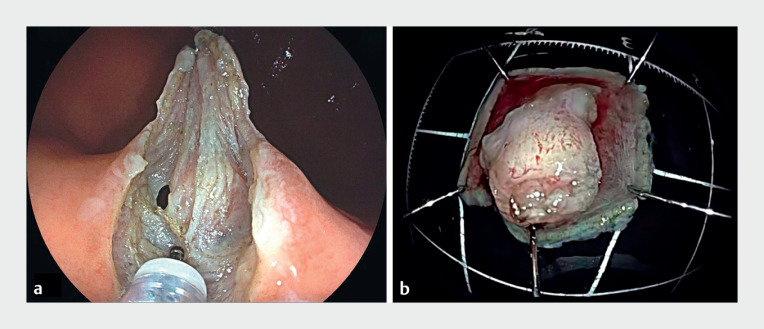 Fig. 2
Fig. 2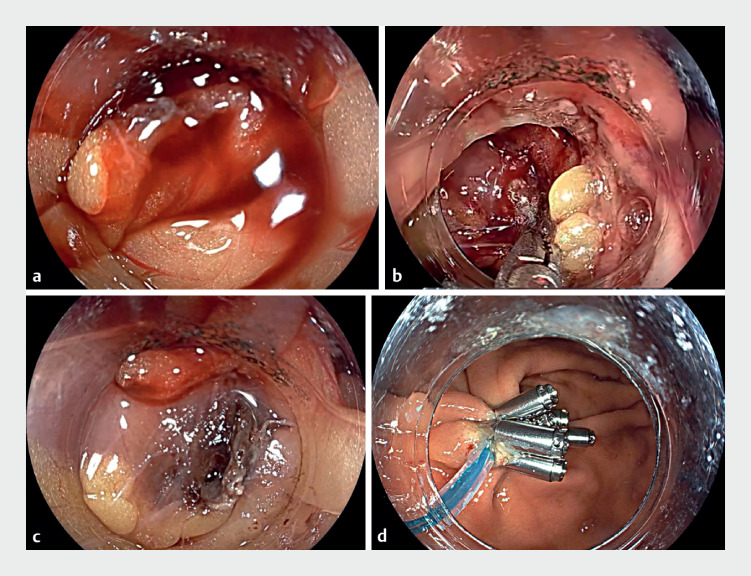 Fig. 3
Fig. 3- —National Natural Science Foundation of China
- —Guangdong Province Clinical Teaching Base Teaching Reform Research Project
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsGastrointestinal Tumor Research and Treatment · Gastrointestinal disorders and treatments · Gastric Cancer Management and Outcomes
Endoscopic full-thickness resection (EFTR) has become the treatment of choice for subepithelial lesions (SELs) that originate from the muscularis propria and/or exhibit exophytic growth patterns 1 . Bleeding is a recognized risk associated with endoscopic resection procedures, occurring both intraoperatively and postoperatively, predominantly from the resection site 2 , with electrocoagulation a well-established technique for achieving hemostasis 3 4 . There have been no previous reports of omental bleeding caused by EFTR. We report a case of extraluminal omental bleeding induced during EFTR for a gastric SEL, which was successfully managed with endoscopic hemostasis ( Video 1 ).
Unexpected omental bleeding occurring during endoscopic full-thickness resection for a subepithelial lesion is successfully managed with endoscopic electrocoagulation.Video 1
A 41-year-old woman underwent gastroscopy, which revealed an 8-mm SEL in the upper gastric body ( Fig. 1 ). She was hospitalized and subsequently underwent EFTR. Intraoperatively, it was confirmed that the lesion was originating from the muscularis propria, with significant exophytic growth ( Fig. 2 a ). Unexpectedly, during the resection, there was a sudden influx of blood into the stomach from the abdominal cavity, with no bleeding observed at the incision site. Once the expeditious and complete removal of the lesion had been completed ( Fig. 2 b ), active bleeding from the omentum was identified, located extraluminally to the stomach wall ( Fig. 3 a ). Consequently, we used disposable hemostatic forceps for electrocoagulation (Soft coagulation, effect level 4, power 80 W) ( Fig. 3 b ) to achieve successful hemostasis ( Fig. 3 c ), ultimately closing the incision with a nylon suture and clips ( Fig. 3 d ). Postoperatively, the patient received antibiotic therapy for 72 hours, and serial hematologic assessments showed no decline in her hemoglobin levels. The patient was discharged 3 days postoperatively, without any other complications having occurred.
Endoscopic view showing a subepithelial lesion, measuring approximately 8 mm in diameter, in the upper part of the gastric body.
Appearance of the tumor: a during the endoscopic full-thickness resection procedure; b following resection.
Endoscopic views showing: a continuous extraluminal omental bleeding; b endoscopic electrocoagulation being performed; c the appearance after successful hemostasis; d closure of the defect with a nylon suture and metal clips.
To the best of our knowledge, this is the first report of omental bleeding induced by EFTR and successfully managed with endoscopic electrocoagulation; it provides valuable insights into the management of complications arising from endoscopic therapeutic interventions.
Endoscopy_UCTN_Code_CPL_1AH_2AZ_3AF
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Deprez PH Moons LMGOʼToole D Endoscopic management of subepithelial lesions including neuroendocrine neoplasms: European Society of Gastrointestinal Endoscopy (ESGE) Guideline Endoscopy 20225441242910.1055/a-1751-574235180797 · doi ↗ · pubmed ↗
- 2Xiu H Zhao CY Liu FG Comparing about three types of endoscopic therapy methods for upper gastrointestinal submucosal tumors originating from the muscularis propria layer Scand J Gastroenterol 2019541481148631814460 10.1080/00365521.2019.1692064 · doi ↗ · pubmed ↗
- 3Aslanian HR Sethi A Bhutani MSASGE guideline for endoscopic full-thickness resection and submucosal tunnel endoscopic resection Video GIE 2019434335010.1016/j.vgie.2019.03.01031388606 PMC 6669323 · doi ↗ · pubmed ↗
- 4Ono H Yao K Fujishiro M Guidelines for endoscopic submucosal dissection and endoscopic mucosal resection for early gastric cancer (second edition)Dig Endosc 20213342010.1111/den.1388333107115 · doi ↗ · pubmed ↗