Appendiceal fecalith misdiagnosed as cecal stromal tumor: don't fall into the trap
Jinghao Li, Dan Liu, Deliang Li, Yangyang Zhou, Yue Zhao, Bingrong Liu

Abstract
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
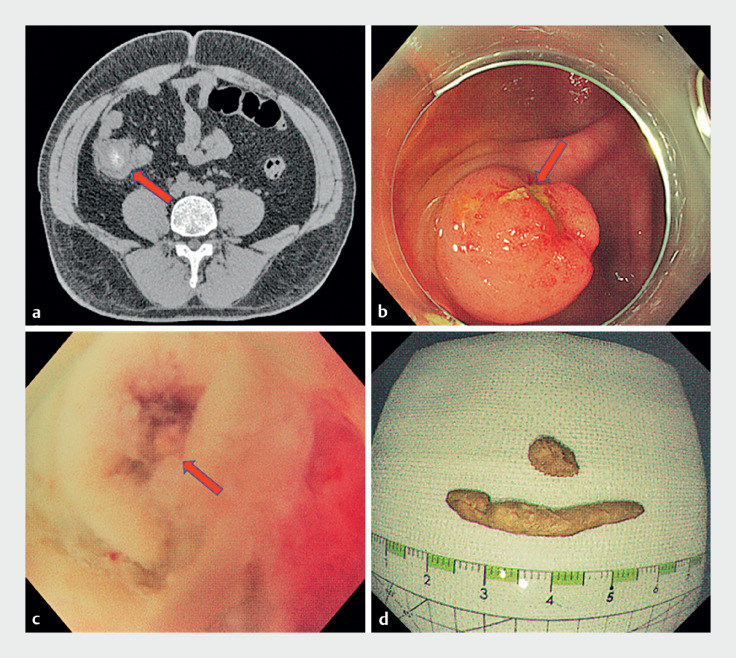 Fig. 1
Fig. 1- —The Key R&D Program of Henan Province
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsIntraperitoneal and Appendiceal Malignancies · Gastrointestinal disorders and treatments · Gastrointestinal Tumor Research and Treatment
A 30-year-old man presented with a 2-day history of hematochezia and a 4-year history of intermittent abdominal pain. Computed tomography scan revealed a low-density mass with central calcification in the cecum ( Fig. 1 a ). Colonoscopy showed a 15×15 mm cecal mass with a superficial ulcer ( Fig. 1 b ). A cecal submucosal tumor was considered. The surgeon recommended ileocecectomy or partial cecectomy. The patient was afraid of surgery and was transferred to our department.
Imaging studies and the cause of symptoms. a Computed tomography of the abdomen showed a cecal mass (arrow) with central calcification. b Colonoscopy showed a mass of approximately 15×15 mm with superficial ulceration (arrow) in the cecum. c The appendix opening (arrow). d The fecaliths.
We performed a second colonoscopy, which revealed that the mass originated from the appendix opening and the “ulcer” appeared to be fecalith-like substance. We made a diagnosis of appendiceal fecalith, not submucosal tumor. A snare was applied to resect the fecalith. With the appendiceal orifice opened ( Fig. 1 c ), a fecalith stump was found in the appendiceal cavity, which confirmed our diagnosis.
Subsequently, endoscopic retrograde appendicitis therapy (ERAT) was performed ( Video 1 ). A catheter was inserted into the end of the appendiceal cavity, normal saline was used to flush the cavity, and two large fecaliths were flushed out ( Fig. 1 d ). Pathologic examination revealed inflammatory tissue. The patient recovered uneventfully and stayed stable during follow-up.
We demonstrate an interesting case of appendiceal fecaliths mimicking appendiceal tumor, which is likely to be misdiagnosed. We performed a minimally invasive procedure, endoscopic retrograde appendicitis therapy, to deal with it, which avoided traumatic surgery for the patient.Video 1
This case suggests that appendiceal fecalith causing mucosal inflammation may be misdiagnosed as cecal submucosal tumor. ERAT has both therapeutic and diagnostic value.
Endoscopy_UCTN_Code_TTT_1AQ_2AH