A Case of Acute Respiratory Distress Syndrome Following Non-thoracic Trauma in a Patient With Idiopathic Pulmonary Fibrosis
Yukinori Hirooka, Soichiro Ota, Noriko Torizawa, Chihiro Maekawa, Youichi Yanagawa

TL;DR
A 72-year-old man with idiopathic pulmonary fibrosis developed acute respiratory distress syndrome after a moderate fall, highlighting the rare but severe complications in such patients.
Contribution
This case report explores the rare occurrence of ARDS following non-thoracic trauma in a patient with IPF.
Findings
ARDS developed in a patient with IPF after a moderate fall and high-altitude exposure.
The patient's respiratory condition rapidly deteriorated despite medical interventions.
Multiple potential contributing factors, including trauma-induced cytokines and environmental exposures, were considered.
Abstract
A 72-year-old man with idiopathic pulmonary fibrosis (IPF) was on home oxygen therapy at 1 L/min. He fell approximately 3 m onto a concrete surface while painting the roof of his home and was emergently transported to a local hospital due to pain in his lower back and right lower limb. His initial Krebs von den Lungen level decreased with medical treatments but has shown an increasing trend over the past three respiratory outpatient visits. His other medical conditions, including dyslipidemia, lumbar pain, and allergic rhinitis, were treated with several drugs prescribed by a nearby clinic. At the previous hospital, an increased oxygen demand of around 5 L via mask was noted, although other vital signs were stable. A plain whole-body computed tomography (CT) scan revealed pulmonary edema, a fracture of the right femoral neck, and a fracture of the third lumbar vertebral body. During…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
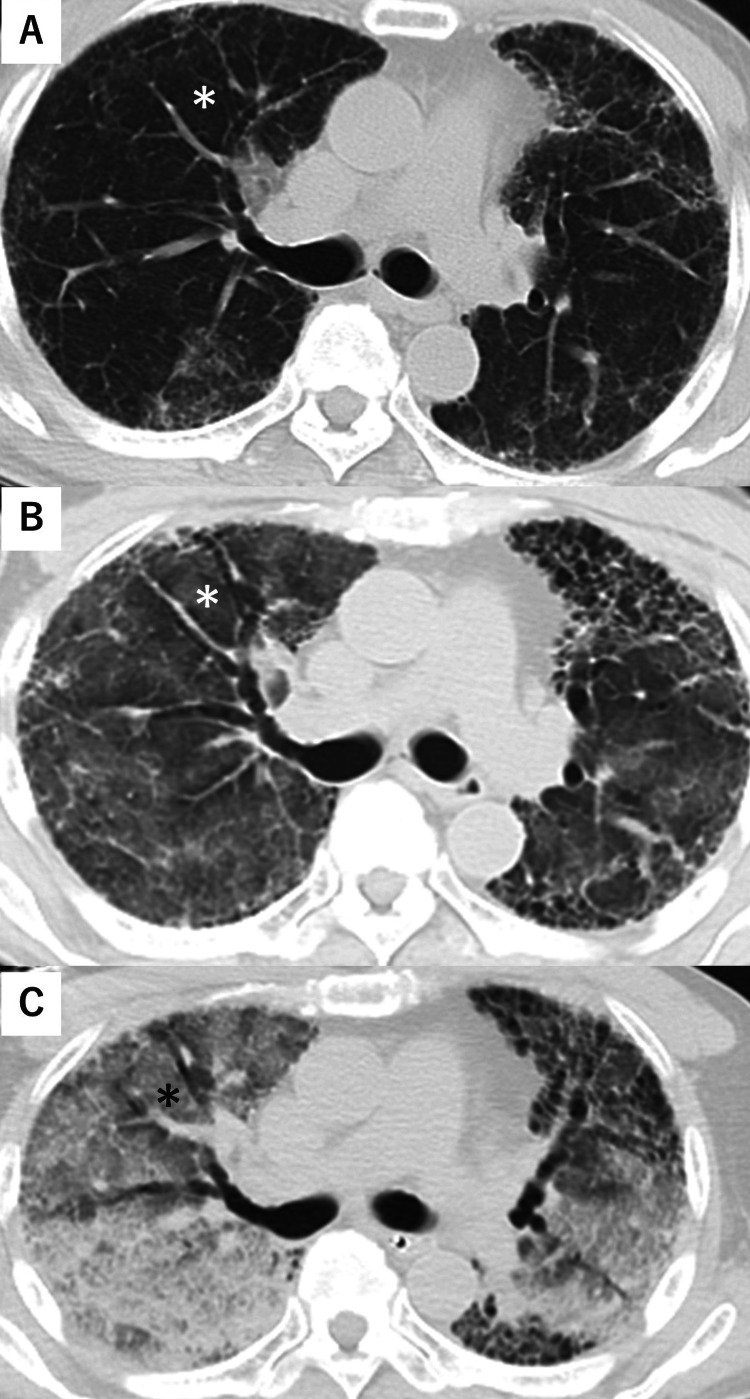 Figure 1
Figure 1| Item | Result | Unit |
| Total Protein | 7.3 | g/dL |
| Glucose | 245 | mg/dL |
| White Blood Cells | 17.3 x 109 | /L |
| Albumin | 3.1 | g/dL |
| Blood Urea Nitrogen | 7.9 | mg/dL |
| Platelets | 221.0 x 109 | /L |
| Total Bilirubin | 1.3 | IU/L |
| Creatinine | 0.9 | mg/dL |
| Alanine Aminotransferase | 29 | IU/L |
| Aspartate Aminotransferase | 41 | IU/L |
| Gamma-Glutamyltransferase | 20 | IU/L |
| Alkaline Phosphatase | 96 | IU/L |
| Lactate Dehydrogenase | 591 | IU/L |
| Creatine Phosphokinase | 486 | IU/L |
| Sodium | 143 | mEq/L |
| Potassium | 3.8 | mEq/L |
| Chloride | 103 | mg/dL |
| C-Reactive Protein | 1.9 | mg/dL |
| Brain Natriuretic Peptide | 35.1 | mg/dL |
| Prothrombin Time International Normalized Ratio | 0.93 | |
| Activated Partial Thromboplastin Time | 24.7 | s |
| Fibrinogen | 296 | mg/dL |
| Fibrinogen Degradation Products | 88.5 | μg/mL |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsInterstitial Lung Diseases and Idiopathic Pulmonary Fibrosis · Respiratory Support and Mechanisms · Pneumothorax, Barotrauma, Emphysema
Introduction
Acute respiratory distress syndrome (ARDS) is characterized by sudden severe oxygen deficiency in the lungs, often with abnormal chest x-ray findings showing fluid in both lungs. This condition is not fully explained by heart failure or excess body fluid. ARDS can be triggered by various factors such as pneumonia, severe infection outside the lungs, aspiration, severe injury, pancreatitis, burns, inhaling smoke or toxic chemicals, drug overdose, coagulopathy, receiving multiple blood transfusions, or unstable circulation [1-3]. The initial insult leads to uncontrolled inflammation and activation of cytokine. Damage to the alveolar epithelial-endothelial barrier can occur directly from lung injuries, which primarily affect the lung tissue, or indirectly from injuries outside the lungs, which primarily affect the vascular endothelium due to widespread inflammation [1]. This damage causes fluid rich in proteins to leak into the lungs, disrupts the function of surfactant, and impairs the exchange of oxygen and carbon dioxide. ARDS can lead to changes in lung function, including reduced ability of the lungs to expand, increased areas of physiological dead space, and increased shunt. There is heterogeneity in outcomes among previous studies, with the 28-day mortality of ARDS remaining high, ranging from 10% to 67% [1].
Idiopathic pulmonary fibrosis (IPF) is a chronic fibrotic lung disease characterized by dry cough, fatigue, and progressive exertional dyspnea [4]. In this debilitating condition, lung parenchyma and architecture are destroyed, compliance is lost, and gas exchange is compromised. This leads inexorably to respiratory failure and death within 3-5 years of diagnosis. The etiopathogenesis of IPF is not fully understood, and treatment options are limited. Pathological features of IPF include extracellular matrix remodeling, fibroblast activation and proliferation, immune dysregulation, cell senescence, and the presence of aberrant basaloid cells [4].
We herein report a case of ARDS following moderate non-thoracic and non-head trauma in a patient with IPF, and discuss the mechanisms involved.
Case presentation
A 72-year-old man with IPF under the care of our respiratory department, receiving home oxygen therapy at 1 L/min, fell from his home roof at a height of 2.5-3 m and sustained injuries. He was found by a neighbor who called for emergency assistance when he was unable to move. Five years ago, he was diagnosed with IPF after presenting with a treatment-resistant cough. At our hospital, his medication history included nintedanib 300 mg, L-carbocisteine 1500 mg, and lansoprazole 15 mg daily. Consequently, his initial Krebs von den Lungen (KL-6) level of 1409 U/mL (normal <500 U/mL) decreased to 504 U/mL, but had shown an increasing trend over the past three respiratory outpatient visits. His other medical conditions included dyslipidemia, lumbar pain, allergic rhinitis, and insomnia, for which he was prescribed atorvastatin, loxoprofen, levocetirizine, fluticasone propionate, carbetapentane, and dihydrocodeine/methylephedrine by a nearby clinic. He had no history of allergies, smoking, or drinking, and his activities of daily living were independent.
Upon contact with the paramedics, his SpO_2_ was 86% despite receiving oxygen at 3 L/min via nasal cannula, indicating poor oxygenation. He had mild tachycardia with a heart rate of 103 beats per minute, but his blood pressure was maintained. He was transported by ambulance to a nearby hospital, where a computed tomography (CT) scan revealed a fracture of the right femoral neck, a fracture of the third lumbar vertebral body, and pulmonary edema. He was then transferred to our hospital by ambulance for surgical intervention. During transport over the 834 m-high Amagi Pass, which is a mix of artificial forests including cedar and cypress trees, the patient experienced oxygen desaturation. Assisted ventilation with a bag valve mask (BVM) under high-concentration oxygen supplementation was initiated, but just before arrival at the hospital, SpO_2_ could not be measured. It took about 3 h from the time of injury to arrival at the hospital.
On arrival, the patient had a Glasgow Coma Scale score of E3V3M5, blood pressure of 195/126 mmHg, heart rate of 64 beats/min, SpO_2_ of 44% (under oxygen supplementation at 15 L/min with BVM ventilation), respiratory rate of 10 breaths/min, and a temperature of 36.8°C. On physical examination, pronounced coarse crackles were auscultated bilaterally. Arterial blood gas analysis (with oxygen at 15 L/min) showed a pH of 7.258, pCO_2_ of 46.9 mmHg, pO_2_ of 29.7 mmHg, HCO_3_^-^ of 20.2 mmol/L, and lactate of 7.6 mmol/L. Echocardiography revealed hyperdynamic movement and right ventricular dilatation. A 12-lead electrocardiogram showed atrial fibrillation. While preparing for emergency endotracheal intubation, the patient vomited frothy liquid. His pulse rate decreased, and there was a sudden decrease in cardiac wall motion, resulting in a near-cardiac arrest state. After stabilizing circulation with pressor agents, a plain and enhanced CT scan was performed. Ground-glass opacities in both lungs had worsened. The enhanced CT did not show obvious embolism in the pulmonary arteries (Figure 1).
Chest computed tomography (CT) (upper [A]: 4 years before; middle [B]: referral hospital; lower [C]: on arrival)On the CT scan from four years ago, the ground-glass opacity is not clearly defined (A). At the referral hospital, diffuse ground-glass opacities appeared (B). After transfer to our hospital, the ground-glass opacity has worsened (C). Focusing on the right segment 3 (), the difference is evident.*
The rapid tests for influenza and COVID-19 at the time of arrival were negative. The patient's laboratory results are shown in Table 1.
Considering the pathophysiology of ARDS, management was initiated with a low tidal volume/high positive end-expiratory pressure ventilation strategy, but oxygenation did not improve. Additionally, CO_2_ gradually accumulated as seen in the arterial blood gas analysis, and the patient died in the emergency room. No autopsy was performed.
Discussion
We discuss the mechanism of rapid deterioration in respiratory status during transport. First, regarding the possibility of cardiogenic pulmonary edema, the patient exhibited a hyperdynamic state on arrival according to cardiac ultrasound, no ST changes were observed on the 12-lead electrocardiogram, and brain natriuretic peptide (BNP) levels were almost within the normal range, leading to the conclusion that at least the respiratory function deterioration during transport was unlikely due to cardiogenic pulmonary edema [5,6]. Even if there is no decrease in ejection fraction, the possibility of diastolic heart failure (heart failure with preserved ejection fraction) remains. Unfortunately, in this case, the measurement of the E/Ea ratio (used for echocardiographic assessment of left ventricular filling pressure) was not performed [7]. However, it should be noted that in this case, BNP levels were barely elevated, blood pressure was usually not high, and the diffuse ground-glass opacity observed on the CT image was atypical for pulmonary edema caused by heart failure [8]. Therefore, the possibility of heart failure with preserved ejection fraction was considered low. Secondly, regarding respiratory dysfunction induced by trauma, there were no signs of chest contusions, and traumatic pulmonary edema due to direct blunt force trauma causing blood-gas barrier disruption was ruled out [9]. The possibility of fat embolism syndrome following trauma cannot be ruled out; however, it is extremely rare for respiratory function to deteriorate so rapidly with femoral neck or lumbar vertebral fractures. Additionally, the imaging indicates worsening pulmonary edema, which is not consistent with deterioration caused by fat embolism [10]. While respiratory status can deteriorate rapidly due to trauma-induced cytokines and lung damage from damage-associated molecular patterns, it is exceedingly rare for respiratory function to deteriorate so rapidly even with more severe trauma [11]. Thirdly, considering the possibility of acute interstitial pneumonia preceding the trauma, with the respiratory condition deteriorating rapidly during transport, it is not uncommon for endogenous diseases to precede trauma, especially in the elderly [12]. In the present case, there is a possibility of acute exacerbation of interstitial pneumonia complicating the underlying lung fibrosis. Previous reports indicate that 193 out of 1019 (18.9%) cases of lung fibrosis have experienced acute exacerbation. In this case, the patient has consistently shown elevated C-reactive protein (CRP) and lactate dehydrogenase (LDH) levels, and a gradual increase in KL-6 levels over the past three respiratory outpatient visits, suggesting an ongoing acute exacerbation. It is possible that the patient fell ill while working due to the acute exacerbation, despite no symptoms of collagen diseases such as rheumatoid arthritis or dermatomyositis being observed clinically. In addition, tests conducted three years ago showed negative rheumatoid factor, anti-cyclic citrullinated peptide antibody, and antinuclear antibody, ruling out ARDS due to acute interstitial pneumonia associated with collagen diseases [13]. While the possibility of developing ARDS from inhaling dust while working on the roof cannot be ruled out, and the possibility of pneumonia caused by medication prescribed at the hospital, COVID-19, and other viral infections besides influenza cannot be denied, the possibilities remain open [14,15]. Furthermore, due to the rapid deterioration in respiratory status during transport, there is a possibility that the patient was exposed to pollen while passing through the Mt. Amagi Pass, leading to a sudden worsening of respiratory status [16]. Additionally, while Mt. Amagi Pass is not a high-altitude pass, being less than 1000 m, which is not particularly problematic for healthy individuals, it may have had a negative impact on patients with respiratory distress [17]. Finally, it could be due to ARDS caused by hypoxemic pulmonary edema. It is clinically known that hypoxemia can increase pulmonary artery pressure, leading to the formation or exacerbation of pulmonary edema [18,19]. Although the patient's respiratory status deteriorated rapidly just before reaching the hospital, it is possible that hypoxemia-induced pulmonary edema exacerbated the condition. If the patient had received early tracheal intubation with a lung-protective strategy, such as low-tidal volume ventilation, permissive hypercapnia, and/or the use of neuromuscular blockers or steroids, he might have had a better chance of survival [19,20].
Conclusions
We present a case of IPF who sustained a femoral neck fracture and a lumbar vertebral body fracture and experienced a rapid deterioration in respiratory function, leading to respiratory failure, during transfer to our hospital, resulting in death. Considering the possibility of an acute exacerbation of IPF prior to the injury, this report discusses the possibility of developing ARDS due to trauma-induced cytokines and lung damage from damage-associated molecular patterns, the possibility of inhaling dust while working on the roof, pneumonia caused by the prescribed medication, viral infections, exposure to pollen and/or high altitude while passing through the mountain pass, and hypoxemia-inducing pulmonary edema. When hypoxemia progresses rapidly, prompt intervention is essential to prevent further deterioration in respiratory status, highlighting the importance of vigilance in such cases.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Acute respiratory distress syndrome in adults: Diagnosis, outcomes, long-term sequelae, and management Lancet Gorman EA O'Kane CM Mc Auley DF 1157117040020223607078810.1016/S 0140-6736(22)01439-8 · doi ↗ · pubmed ↗
- 2Experience with trauma-induced ARDS: A retrospective study of US wartime casualties 2003-2015 J Spec Oper Med Nam JJ Mc Cravy MS Haines KL 11111622202210.55460/MTVH-ONCM 36525023 · doi ↗ · pubmed ↗
- 3Mild to moderate to severe: What drives the severity of ARDS in trauma patients?Am Surg Daher P Teixeira PG Coopwood TB 808812842018 https://pubmed.ncbi.nlm.nih.gov/29981606/29981606 · pubmed ↗
- 4Idiopathic pulmonary fibrosis: Current and future treatment Clin Respir J Glass DS Grossfeld D Renna HA Agarwala P Spiegler P De Leon J Reiss AB 84961620223500152510.1111/crj.13466 PMC 9060042 · doi ↗ · pubmed ↗
- 5Advancing precision medicine for the diagnosis and treatment of acute respiratory distress syndrome J Clin Med Rizzo AN Aggarwal NR Thompson BT Schmidt EP 15631220233683609810.3390/jcm 12041563 PMC 9966442 · doi ↗ · pubmed ↗
- 6Novel biomarkers in early detection of heart failure: A narrative review Cureus Kayani M Fatima N Yarra PC 016202410.7759/cureus.53445 PMC 1090937938435138 · doi ↗ · pubmed ↗
- 7Novel echocardiographic markers for left ventricular filling pressure prediction in heart failure with preserved ejection fraction (ECHO-PREDICT): A prospective cross-sectional study Ann Med Surg (Lond) Suleman M Saqib M Mumtaz H Iftikhar M Raza A Rauf Butt S Talha KM 538453958520233791567410.1097/MS 9.0000000000001287 PMC 10617904 · doi ↗ · pubmed ↗
- 8Ground-glass opacity (GGO): A review of the differential diagnosis in the era of COVID-19Jpn J Radiol Cozzi D Cavigli E Moroni C Smorchkova O Zantonelli G Pradella S Miele V 7217323920213390054210.1007/s 11604-021-01120-w PMC 8071755 · doi ↗ · pubmed ↗