Hybrid Repair of Infected Femoral Artery Pseudoaneurysm: Stent Graft Placement and Artificial Graft Replacement
Hirotaka Yamauchi, Soichiro Kageyama, Akinori Kojima, Hideo Morita, Takeki Ohashi

TL;DR
A 70-year-old cancer patient with an infected femoral artery pseudoaneurysm was successfully treated with a hybrid procedure combining stent graft placement and artificial graft replacement.
Contribution
The paper presents a novel hybrid surgical approach for managing infected pseudoaneurysms in patients who cannot tolerate more invasive procedures.
Findings
The hybrid treatment effectively controlled the infected pseudoaneurysm in a patient with a history of cancer.
The procedure avoided a highly invasive abdominal surgery, resulting in a favorable postoperative recovery.
Antibiotic therapy alone was insufficient, but combined with hybrid surgery, it led to successful infection control.
Abstract
A femoral artery pseudoaneurysm is the most prevalent complication of femoral access due to the artery's accessibility and frequent use for catheterization and blood tests. An infected femoral artery pseudoaneurysm is often life-threatening and challenging to manage. A 70-year-old male with a history of tongue cancer treatments, including resection, lymph node dissection, and radiation chemotherapy, visited his previous physician for a fever and was prescribed oral antibiotics, but the fever persisted, accompanied by pain and a mass in the left groin. An enhanced CT revealed an infected pseudoaneurysm of the left femoral artery. The fever's etiology was unclear but likely stemmed from a blood draw from the femoral artery during a prior visit, resulting in a pseudoaneurysm that became infected. The patient was transferred to our hospital due to management challenges. Blood cultures from…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
 Figure 1
Figure 1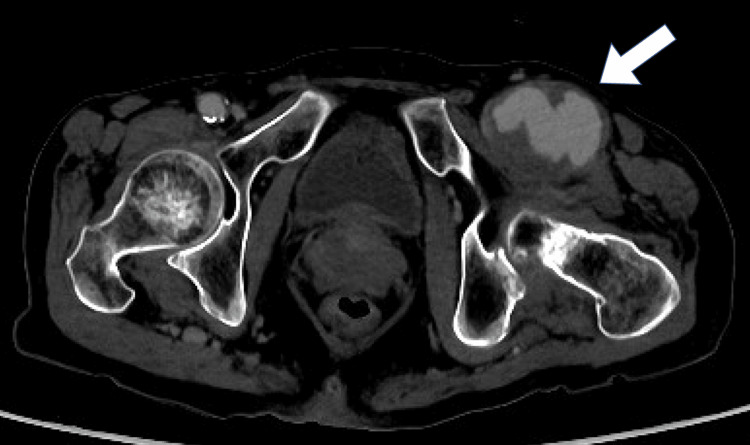 Figure 2
Figure 2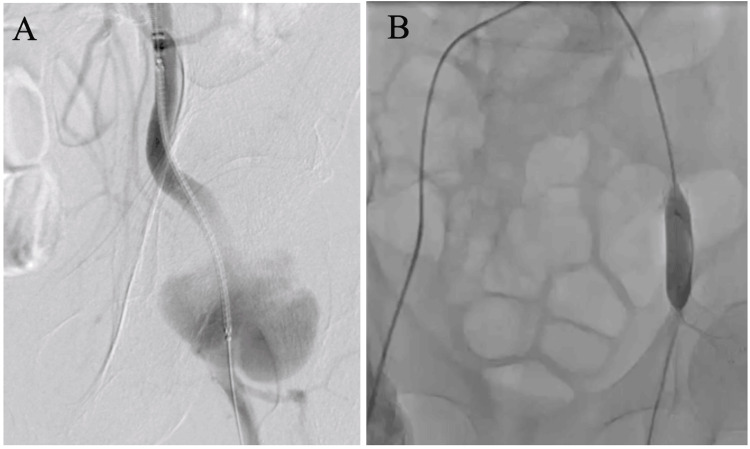 Figure 3
Figure 3 Figure 4
Figure 4| Laboratory analysis | Results | Normal range |
| White blood cell counts (/μL) | 7,600 | 3,300-8,600 |
| Hemoglobin (g/dL) | 11.9 | 13.7-16.8 |
| Platelet count (×103/μL) | 473 | 158-348 |
| Creatine kinase (U/L) | 26 | 59-248 |
| Lactate dehydrogenase (U/L) | 171 | 124-222 |
| Aspartate aminotransferase (U/L) | 80 | 13-30 |
| Alanine aminotransferase (U/L) | 39 | 10-42 |
| γ-glutamyl transpeptidase | 45 | 13-64 |
| Total bilirubin (mg/dL) | 0.2 | 0.4-1.5 |
| Direct bilirubin (mg/dL) | 0.1 | 0.1-0.3 |
| Alkaline phosphatase (U/L) | 126 | 38-113 |
| Amylase (mg/dL) | 61 | 44-132 |
| Creatinine (mg/dL) | 0.58 | 0.65-1.07 |
| Blood urea nitrogen (mg/dL) | 13.7 | 8.0-20.0 |
| Uric acid (mg/dL) | 2.3 | 3.7-7.8 |
| Sodium (mEq/L) | 139 | 138-145 |
| Potassium (mEq/L) | 4.2 | 3.6-4.8 |
| Chloride (mEq/L) | 102 | 101-108 |
| Total cholesterol (mg/dL) | 150 | 142-248 |
| HDL-cholesterol (mg/dL) | 34 | 38-90 |
| LDL-cholesterol (mg/dL) | 104 | 65-163 |
| C-reactive protein (U/L) | 9.21 | 0.00-0.14 |
| Blood sugar (mg/dL) | 124 | 73-109 |
| HbA1c (NGSP) (%) | 6.4 | 4.9-6.0 |
| Activated partial thromboplastin time (sec) | 36.0 | 26.0-38.0 |
| Prothrombin time (% in the normal range) | 57.9 | 80.0-120.0 |
| Fibrinogen (mg/dL) | >800 | 200-400 |
| Laboratory analysis | Results | Normal range |
| White blood cell counts (/μL) | 6,500 | 3,300-8,600 |
| Hemoglobin (g/dL) | 12.4 | 13.7-16.8 |
| Platelet count (×103/μL) | 221 | 158-348 |
| Creatine kinase (U/L) | 33 | 59-248 |
| Lactate dehydrogenase (U/L) | 202 | 124-222 |
| Aspartate aminotransferase (U/L) | 43 | 13-30 |
| Alanine aminotransferase (U/L) | 27 | 10-42 |
| γ-glutamyl transpeptidase | 25 | 13-64 |
| Total bilirubin (mg/dL) | 0.5 | 0.4-1.5 |
| Direct bilirubin (mg/dL) | 0.1 | 0.1-0.3 |
| Alkaline phosphatase (U/L) | 109 | 38-113 |
| Amylase (mg/dL) | 62 | 44-132 |
| Creatinine (mg/dL) | 0.83 | 0.65-1.07 |
| Blood urea nitrogen (mg/dL) | 21.9 | 8.0-20.0 |
| Uric acid (mg/dL) | 3.5 | 3.7-7.8 |
| Sodium (mEq/L) | 146 | 138-145 |
| Potassium (mEq/L) | 4.5 | 3.6-4.8 |
| Chloride (mEq/L) | 107 | 101-108 |
| C-reactive protein (U/L) | 0.22 | 0.00-0.14 |
| Blood sugar (mg/dL) | 96 | 73-109 |
| Activated partial thromboplastin time (sec) | 29.8 | 26.0-38.0 |
| Prothrombin time (% in the normal range) | 74.7 | 80.0-120.0 |
| Fibrinogen (mg/dL) | 387 | 200-400 |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsVascular Procedures and Complications · Infectious Aortic and Vascular Conditions · Aortic aneurysm repair treatments
Introduction
The femoral artery is highly accessible and frequently utilized for catheterization and blood tests. A pseudoaneurysm of the femoral artery is the most prevalent complication at the femoral access site, arising post-catheterization, anastomosis of the native artery and artificial graft, trauma, or infection [1]. Notably, infected femoral artery pseudoaneurysm (IFAP) is often life-threatening and challenging to manage. Treating IFAP necessitates open surgical repair, which carries a high complication rate [2-4].
Recent advancements have made endovascular stent-graft placement an effective and minimally invasive alternative technique for aneurysm treatment, particularly as a temporary bridge for critically ill patients [5].
In this report, we describe a case of IFAP caused by a blood draw puncture to the groin, despite the infection source being unknown. A hybrid repair was performed to minimize invasiveness for a patient with carcinoma in situ who was at high risk. This treatment may be beneficial for patients who are unsuitable for highly invasive procedures.
Case presentation
A 70-year-old male patient was transferred to our department for further evaluation and management of an infected pseudoaneurysm of the left femoral artery, occurring during chemotherapy for tongue cancer. The patient had previously undergone tongue resection and lymph node dissection for tongue cancer, resulting in a tracheotomy and gastrostomy. Additionally, a central venous port was implanted for chemotherapy and radiation therapy. However, due to persistent cancer recurrences, the patient was reluctant to continue the current chemotherapy regimen.
During a visit to his previous physician for a fever, he was prescribed amoxicillin, an oral antibiotic. Despite this, the fever persisted, and pain accompanied by a mass in the left groin was observed. A CT scan indicated the presence of inguinal cellulitis, and the antibiotic regimen was adjusted to levofloxacin. Three days later, the patient presented with a pulsatile mass and worsening pain. Enhanced CT imaging confirmed the diagnosis of an infected pseudoaneurysm of the left femoral artery (Figure 1).
The previous hospital's enhanced CT shows a pseudoaneurysm with diameter of 41 x 50 mmThe arrow indicates the failed vessel wall and the leaking blood, which is compressing the surrounding tissue.CT: computed tomography
The Duke classification was not met except for blood culture, including UCG, infectious endocarditis was negative, and the etiology of the fever was unclear. It was hypothesized that a blood draw from the femoral artery during the previous visit led to the formation of a pseudoaneurysm that subsequently became infected. Consequently, surgical intervention was deemed necessary, and the patient was referred to our hospital 10 days after the initial visit to the previous physician. Methicillin-sensitive Staphylococcus aureus was identified in the blood culture at the previous hospital, and antibiotic treatment was switched to intravenous cefazolin.
Upon arrival, the patient was alert with a blood pressure of 108/69 mmHg, a heart rate of 71 beats per minute, a respiratory rate of 16 breaths per minute, and a body temperature of 36.6°C. Laboratory tests showed elevated C-reactive protein, indicating an active infection (Table 1).
Although stent graft placement or artificial vessel replacement was considered, we opted for an extended course of antibiotic therapy for a minimum of two weeks, potentially up to a month, pending multiple negative blood cultures and normalization of inflammatory markers. Initially, antibiotics were administered to manage the infection, and a negative blood culture was achieved at our hospital, with subsequent blood tests showing significant improvement (Table 2).
However, the aneurysm demonstrated clear signs of enlargement, necessitating emergency surgical intervention (Figure 2).
Enhanced CT at the time of emergency surgery reveals an enlarged pseudoaneurysmThe allow indicates a pseudoaneurysm enlarged to 46 x 56 mm.CT: computed tomography
Given the rapid expansion of the aneurysm and the associated risk of anastomotic failure due to the extensive replacement required, we selected a hybrid approach involving stent grafting from the external iliac artery to the proximal femoral artery, followed by artificial vessel replacement (Figure 3).
Hybrid repair performed in two stagesA: Viabahn®️ (10 x 100 mm) placed from the left external iliac artery to the common iliac artery. B: Mustang®️ (10 x 40 mm) was used to block blood flow at the stent graft site and anastomosed with PROPATEN®️ (8 mm).
The infected pseudoaneurysm extended from the left external iliac artery to the CFA. Typically, such a procedure would require abdominal access to replace the external iliac artery, which is considerably more invasive. Instead, we employed a hybrid strategy that involved implanting a stent graft from the external iliac artery to the proximal CFA, followed by artificial vessel replacement from this point to the femoral artery bifurcation. The artificial vessel was end-to-end anastomosed on both sides. The postoperative course was uneventful, and follow-up enhanced CT imaging confirmed the absence of complications such as vascular collapse (Figure 4).
3D CT imaging demonstrates that the stent graft and artificial vessels remain intact and do not exhibit any signs of failure3D: three-dimensional, CT: computed tomography
Twelve days post-surgery, the patient was transferred back to the previous hospital for continued rehabilitation due to discharge difficulties. Over a follow-up period of two months, the patient was discharged and appeared to be in good health. Unfortunately, the cancer had metastasized to his lungs and was progressing. Should the patient's condition worsen, palliative care will be considered. In this case, we successfully managed the infected pseudoaneurysm despite the impossibility of achieving a radical cure for cancer, demonstrating that hybrid therapy can be an effective strategy for patients who are not candidates for more invasive treatments.
Discussion
The complication rate associated with IFAP is elevated, and the procedure is inherently highly invasive [2-4]. Endovascular stent-graft placement is an efficacious and minimally invasive alternative technique, particularly as a provisional measure for critically ill patients [5]. In this case, the patient was able to circumvent laparotomy and mitigate procedural invasiveness through a combination of artificial vessel replacement and stent-grafting techniques.
In previous reports, IFAPs are most frequently attributed to drug abuse. The standard procedure for IFAPs involves ligation of the CFA without subsequent revascularization, which, although common, poses significant risks of claudication, ischemia, and potential amputations [6]. Since drug-induced pseudoaneurysms are uncommon in our country, catheter procedures and femoral artery punctures are the primary causes. Given the high risk of ischemia and lower extremity amputation when collateral blood vessels are not well-developed, simple ligation of the CFA is not considered standard treatment. Treatment that includes revascularization is generally regarded as the standard of care. The principles of standard management dictate that the deployment of a covered stent is unlikely to succeed as a treatment option for infected pseudoaneurysms. This is because exclusion, rather than excision, of the pathology may result in a confined infection and contamination of the newly placed device, potentially leading to limb- and life-threatening consequences [7]. Emergency percutaneous stent graft implantation followed by secondary surgical repair was performed in this case. The stent graft was extended to the external iliac artery, with the peripheral side anastomosed to the artificial vessel.
If the anastomosis becomes infected, an anastomotic pseudoaneurysm could develop, posing a risk of life-threatening rupture. Stent grafting has been reported to be effective in treating infected anastomotic pseudoaneurysms [8]. There are also objections to placing stent grafts in all the common femoral arteries, and placement in designated "no stent zones" is not appropriate [9]. Consequently, we minimized the use of stent grafts in these areas by utilizing an artificial blood vessel.
Conclusions
Although surgery remains the preferred procedure for repairing IFAPs, the combination of stent graft placement followed by pseudoaneurysm resection, surgical debridement, partial vascular replacement, and antimicrobial therapy has proven to be a viable, less invasive option in emergency pseudoaneurysm surgery. The results of this study are presented in the following sections: Hybrid surgery may be the most favored treatment for patients who are not suitable candidates for major surgery, in terms of both safety and efficacy.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Management trends for postcatheterization femoral artery pseudoaneurysms JAAPA Madia C 151832201910.1097/01.JAA.0000558236.60240.0231094871 · doi ↗ · pubmed ↗
- 2A prospective evaluation of surgically treated groin complications following percutaneous cardiac procedures Am Surg Lumsden AB Miller JM Kosinski AS Allen RC Dodson TF Salam AA Smith RB 3rd 132137601994 https://pubmed.ncbi.nlm.nih.gov/8304645/8304645 · pubmed ↗
- 3Contemporary management of postcatheterization pseudoaneurysms Circulation Webber GW Jang J Gustavson S Olin JW 2666267411520071751547910.1161/CIRCULATIONAHA.106.681973 · doi ↗ · pubmed ↗
- 4Current treatment methods for postcatheterization pseudoaneurysms J Vasc Interv Radiol Morgan R Belli AM 6977101420031281703710.1097/01.rvi.0000071089.76348.6a · doi ↗ · pubmed ↗
- 5Current hybrid interventions in vascular surgery: merging past and present Mo Med Huffman J Nichols WK Bath J 3813861182021 https://www.ncbi.nlm.nih.gov/pmc/articles/PMC 8343637/34373675 PMC 8343637 · pubmed ↗
- 6Common femoral artery ligation and local debridement: a safe treatment for infected femoral artery pseudoaneurysms J Vasc Surg Arora S Weber MA Fox CJ Neville R Lidor A Sidawy AN 9909933320011133183910.1067/mva.2001.114212 · doi ↗ · pubmed ↗
- 7Infection with fatal outcome after endovascular metallic stent placement Radiology Therasse E Soulez G Cartier P Passerini L Roy P Bruneau L Gaboury L 3633651921994802939810.1148/radiology.192.2.8029398 · doi ↗ · pubmed ↗
- 8Hybrid repair of ruptured infected anastomotic femoral pseudoaneurysms: emergent stent-graft implantation and secondary surgical debridement J Vasc Surg Klonaris C Katsargyris A Vasileiou I Markatis F Liapis CD Bastounis E 9389454920091914732010.1016/j.jvs.2008.10.063 · doi ↗ · pubmed ↗