Estimating the human bottleneck for contact tracing
Maximilian D Broda, Petra Borovska, Diana Kollenda, Marcel Linka, Naomi de Haas, Samuel de Haas, Benjamin de Haas

TL;DR
This study estimates how well people remember recent contacts, which is important for effective contact tracing during outbreaks.
Contribution
The study quantifies how memory for contacts declines over time and identifies factors like age and memory aids that influence this decline.
Findings
Contact reporting declines as a power function of recall delay.
Younger people and those using memory aids report more contacts.
Older people and those without memory aids experience steeper declines in contact reporting.
Abstract
The SARS-CoV-2 pandemic has highlighted the importance of contact tracing for epidemiological mitigation. Contact tracing interviews (CTIs) typically rely on episodic memory, which is prone to decline over time. Here, we provide a quantitative estimate of reporting decline for age- and gender-representative samples from the United Kingdom and Germany, emulating >15,000 CTIs. We find that the number of reported contacts declines as a power function of recall delay and is significantly higher for younger subjects and for those who used memory aids, such as a scheduler. We further find that these factors interact with delay: Older subjects and those who made no use of memory aids have steeper decline functions. These findings can inform epidemiological modeling and policies in the context of infectious diseases.
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
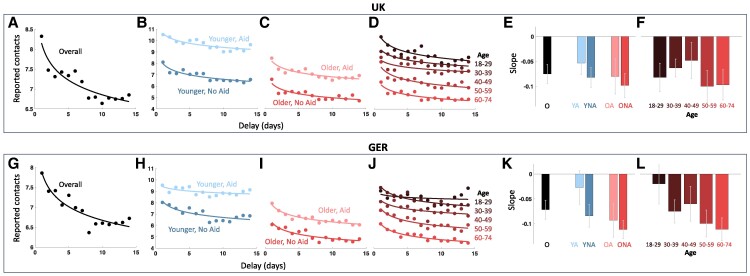 Fig. 1
Fig. 1| Overall | YA | YNA | OA | ONA | |
|---|---|---|---|---|---|
|
| |||||
| Intercept (95% CI) | 8.15 | 10.62 | 7.97 | 8.19 | 6.23 |
| Slope | −0.075 | −0.053 | −0.082 | −0.080 | −0.098 |
|
| 85% | 73% | 83% | 80% | 74% |
| ΔAIC | −9.12 | −2.27 | −5.38 | −8.92 | −7.52 |
|
| |||||
| Intercept (95% CI) | 7.87 | 9.42 | 8.13 | 7.80 | 6.25 |
| Slope | −0.072 | −0.027 | −0.084 | −0.093 | −0.112 |
|
| 84 | 36 | 70 | 91 | 80 |
| ΔAIC | −8.72 | −2.22 | −4.91 | −14.66 | −2.51 |
| Beta (95% CI) |
|
| |
|---|---|---|---|
|
| |||
| Intercept | 1.723 (1.684, 1.762) | 85.96 | <10−9 |
| Delay [log(days)] | −0.079 (−0.085, −0.074) | −27.93 | <10−9 |
| Aid use | 0.348 (0.302, 0.393) | 15.06 | <10−9 |
| Older | −0.292 (−0.337, −0.247) | −12.69 | <10−9 |
| Delay:Aid use | 0.024 (0.018, 0.030) | 7.42 | <10−9 |
| Delay:Older | −0.020 (−0.027, −0.014) | −6.22 | <10−9 |
|
| |||
| Intercept | 1.747 (1.708, 1.786) | 86.94 | <10−9 |
| Delay [log(days)] | −0.075 (−0.080, −0.069) | −25.46 | <10−9 |
| Aid use | 0.252 (0.207, 0.296) | 11.18 | <10−9 |
| Older | −0.293 (−0.337, −0.249) | −13.03 | <10−9 |
| Delay:Aid use | 0.041 (0.035, 0.048) | 12.55 | <10−9 |
| Delay:Older | −0.048 (−0.055, −0.042) | −14.53 | <10−9 |
- —European Research Council10.13039/501100000781
- —German Research Foundation10.13039/501100001659
- —Ministry of Higher Education10.13039/501100011821
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsCOVID-19 Digital Contact Tracing · Data-Driven Disease Surveillance · Privacy, Security, and Data Protection
Introduction
The SARS-CoV-2 pandemic has highlighted the importance of contact tracing for public health. Epidemiological mitigation can crucially depend on case isolation (1) which requires identification of infected individuals and their chain of contacts (1, 2). This is traditionally attempted by standardized contact tracing interviews (CTIs). Modeling suggested that CTIs suffered from severe speed limitations in the context of SARS-CoV2 (2, 3), leading many nations to implement digital contact tracing apps (CTAs) (4). However, CTAs suffered from limited adoption (5). This has led to the parallel use of traditional CTIs, requiring infected individuals to report contacts going back up to 10 days or more.
A principal bottleneck of CTIs is memory decline (6–10). Basic and applied research has shown that long-term episodic memory is susceptible to distortions, interference and loss of information (6, 8, 11–13). However, it is largely unclear how memory decline affects CTIs. What fraction of relevant contacts do people typically remember after a day, a week, or two? Does declining contact memory follow a linear (14), or power function (12, 13) of recall delay? And how is this modulated by age and the use of memory aids, such as a scheduler? Quantitative estimates of this bottleneck could provide lower bounds of under-reporting and thus inform epidemiological modeling and policies.
A major obstacle in the way of quantifying the decline of contact memory is the unknown ground truth, which is expected to vary over time. Ben may have met particularly many people during a birthday party last Saturday, while Max's number of contacts peaked during an office meeting on Wednesday. Pilot data indicate that individual contact reports can indeed vary by orders of magnitude across days.
Here, we aimed to overcome these challenges with the power of large samples. With the help of a panel provider, we recruited 15,015 subjects in April and May 2023, aiming at age- and gender-representative samples of the 18- to 74-year-old populations of the United Kingdom and Germany (GER). Subjects completed an online questionnaire designed in consultation with local health authorities (Gesundheitsamt, Landkreis Giessen, Germany) to emulate CTIs. Specifically, the questionnaire asked subjects to make use of memory aids such as a scheduler or calendar app wherever possible and provided a definition of relevant contacts. Then, subjects were asked to note such contacts on a sheet of paper, count them and enter their number into the survey, separately for increasingly wider domains of social interaction. Every subject repeated this procedure for each of the 14 preceding days in turn (i.e. with increasing reporting delay). Finally, subjects indicated their use of memory aids using a five-point Likert scale. A total of 13,407 interviews were included into the final analysis (6,733 and 6,674 for United Kingdom and GER, respectively; see Supplementary material for details).
We find that the average number of reported contacts indeed is subject to decline, following a power function of reporting delay. The slope and intercept of this decline interacts with age and the use of memory aids, indicating more severe contact memory decline for older subjects and those who reported no use of memory aids.
First, we computed the average number of reported contacts, separately for each reporting delay and sample (Fig. 1A and G). In both samples, reported contacts declined with delay. This relationship was captured well by power functions of the form
with AC corresponding to the average number of reported contacts, delay to the reporting delay in days, and factor b and exponent m to intercept and slope parameters, respectively. For the United Kingdom and GER, these power fits explained 85 and 84% of variance and had significantly negative exponents of −0.075 (95% CI: −0.095, −0.056) and −0.072 (95% CI −0.091, −0.053), respectively (black bars in Fig. 1E and K). The power decline functions provided a better explanation of the data than linear fits, as indicated by the Akaike Information Criterion (ΔAIC < −8.7 for both samples).
Memory decline for the United Kingdom and GER samples. Scatter points in (A–D) and (G–J) show the average number of reported contacts for 1–14 days of reporting delay. The corresponding line fits show the best fitting power functions. A and G) show the data for all respective subjects, B, C, H, and I) split the data according to age and aid use, indicated by hue and saturation as labeled. D and J) split the data into finer age brackets as indicated by hue, as labeled. Bars in (E, F) and (K, L) show the best fitting slopes of the corresponding power functions. Gray error bars indicate 95% confidence intervals. O, overall; YA, younger subjects using aids; YNA, younger subjects using no aids; OA, older subjects using aids; ONA, older subjects using no aids.
Next, we split the data according to median age (United Kingdom: 45, GER: 47) and the reported use of memory aids, such as a scheduler (55%/51% of United Kingdom/GER subjects reported no aid use, see Supplementary material; Fig. 1B, C, H, and I). We found moderate to strong evidence in favor of power over linear fits for each of the four resulting subdivisions (Table 1). As can be seen in Fig. 1, the overall number of reported contacts was substantially lower for older compared to younger subjects and for subjects who reported no use of memory aids compared to those who did. In addition to these intercept effects, the best fitting slope parameters indicated a steeper decline of reported contacts for older subjects and those who reported no use of memory aids (Fig. 1E and K; Table 1).
To test the statistical significance of these effects we entered the full datasets (not just the daily averages) into a Generalized Linear Mixed model (GLMM) of the form:
with a Poisson link function. That is, we modeled the number of reported contacts (C) as a function of the delay in days (log transformed to compensate for the nonlinearity of the memory decline), with additional binary fixed effects for aid and age group, as well as fixed effects for their interactions with delay, and a random effect for subject identity. All fixed effects (including the interaction terms) were highly significant, for both the United Kingdom (all |t| > 6, all P < 10^−9^) and GER (all |t| > 12, all P < 10^−9^) (Table 2). An additional GLMM splitting the age predictor into five brackets corroborated these results for both the United Kingdom (all |t| > 4, all P < 10^−5^) and GER (all |t| > 8, all P < 10^−9^). Fitting separate decline functions for each age bracket showed decreasing intercepts and trends for increasingly negative slopes (Fig. 1D, F, J, and L).
Taken together, these data provide strong evidence that contact reports in a CTI design used by practitioners decline as a power function of reporting delay. This underscores the substantial cognitive bottleneck for CTIs (6–8) and severity of underreporting even for minor delays. Contact tracing guidelines should utilize recently investigated strategies to mitigate underreporting and speed up the CTI process (6–8, 10, 15). Epidemiological models should take under-reporting, its dependence on delay and interactions with infection dynamics into account.
We found steeper declines of reported contacts for older subjects and those who reported no use of memory aids. The effects of age and aid use were substantial from the first day. This may partly reflect a smaller number of actual contacts for older participants and those who reported no use memory aids. But the interaction with delay clearly indicates more severe underreporting in these subjects. The strong effect of memory aids and frequent lack of their use suggests that CTI designs could profit from routine instructions on how to leverage prevalent memory aids (such as smartphones). This is in line with previous research showing that the design of CTIs can strongly influence the number of reported contacts (6, 7, 10, 15), including recent results showing that the relationship between the number of reported contacts and reporting delay is modulated by the direction of recall (15). Further research is needed to understand the different mechanisms at play and to optimize the design of CTIs.
Reassuringly, all our findings closely replicated across the United Kingdom and GER samples. Nevertheless, our estimates of memory decline may not readily generalize to populations with symptoms or different patterns of social contacts, or to lock-down situations. Further, our design is insensitive to the absolute intercept of under-reporting (which may be exacerbated by early forgetting, carelessness or dishonesty). We therefore consider our estimates lower bounds of under-reporting for the type of CTI design we tested.
Materials and methods
The study was approved by the institutional review board of FB06, Justus-Liebig University Giessen, and all subjects provided written informed consent. See Supplementary material and Supplementary Appendices for survey details.
Supplementary Material
pgae283_Supplementary_Data
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Hellewell J , et al 2020. Feasibility of controlling COVID-19 outbreaks by isolation of cases and contacts. Lancet Global Health 8:e 488–e 496.32119825 10.1016/S 2214-109X(20)30074-7PMC 7097845 · doi ↗ · pubmed ↗
- 2Kretzschmar ME , et al 2020. Impact of delays on effectiveness of contact tracing strategies for COVID-19: a modelling study. Lancet Public Health 5:e 452–e 459.32682487 10.1016/S 2468-2667(20)30157-2PMC 7365652 · doi ↗ · pubmed ↗
- 3Ferretti, L, et al 2020. Quantifying SARS-Co V-2 transmission suggests epidemic control with digital contact tracing. Science (New York, N.Y.)368:eabb 6936.32234805 10.1126/science.abb 6936 PMC 7164555 · doi ↗ · pubmed ↗
- 4Garry M , et al 2023. Hits and misses: digital contact tracing in a pandemic. Perspect Psychol Sci [online ahead of print]. 10.1177/17456916231179365.PMC 1031550537390338 · doi ↗ · pubmed ↗
- 5Vogt F , Haire B, Selvey L, Katelaris AL, Kaldor J. 2022. Effectiveness evaluation of digital contact tracing for COVID-19 in New South Wales, Australia. Lancet Public Health. 7:e 250–e 258.35131045 10.1016/S 2468-2667(22)00010-XPMC 8816387 · doi ↗ · pubmed ↗
- 6Mosser AE , Evans JR. 2019. Increasing the number of contacts generated during contact tracing interviews. Memory. 27:495–506.30295153 10.1080/09658211.2018.1529247 · doi ↗ · pubmed ↗
- 7Evans JR , et al 2022. Enhancing the effectiveness of contact tracing interviews: a randomized controlled experiment of an enhanced cognitive interview protocol. Am J Infect Control. 50:631–637.34971713 10.1016/j.ajic.2021.12.015 · doi ↗ · pubmed ↗
- 8Garry M , Hope L, Zajac R, Verrall AJ, Robertson JM. 2021. Contact tracing: a memory task with consequences for public health. Perspect Psychol Sci. 16:175–187.33301692 10.1177/1745691620978205 · doi ↗ · pubmed ↗