Double Trouble: An Unusual Presentation of Bilateral Penile Fracture
Kishor M, Deepak Ghuliani, Sushanto Neogi, Shiva Kiran Addu, Abhinav Singh

TL;DR
A rare case of a 38-year-old man with a double penile fracture during sexual activity was successfully treated with surgery.
Contribution
This paper presents a rare case of bilateral penile fracture and emphasizes the importance of timely surgical intervention.
Findings
Bilateral tunica albuginea ruptures were confirmed via examination and ultrasound.
Surgical repair led to full recovery without complications.
Prompt recognition and treatment are critical to prevent long-term issues.
Abstract
A penile fracture results from the rupture of the tunica albuginea due to blunt trauma to an erect penis and is a rare urological emergency. Double penile fractures involving both corpora cavernosa injuries are extremely uncommon. We report the case of a 38-year-old male who experienced acute penile pain, swelling, and a "cracking" sound during sexual intercourse. Examination and ultrasound confirmed bilateral tunica albuginea ruptures and hematoma. The surgical repair involved hematoma evacuation and suturing of the tears. The patient recovered without complications. This case highlights the necessity for prompt recognition and surgical intervention in double penile fractures to prevent long-term complications and ensure optimal recovery.
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
 Figure 1
Figure 1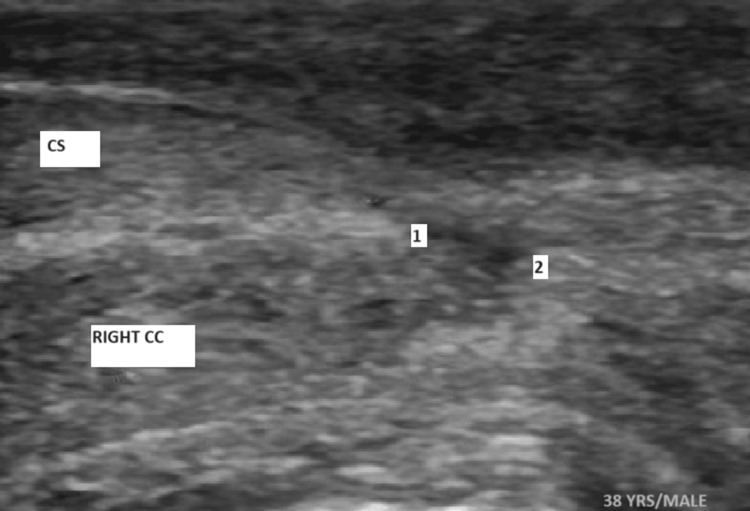 Figure 2
Figure 2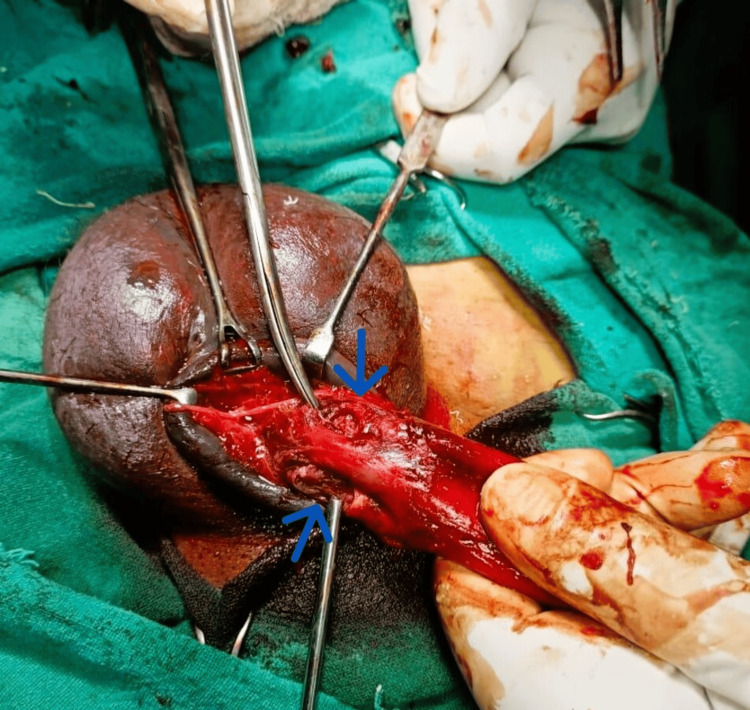 Figure 3
Figure 3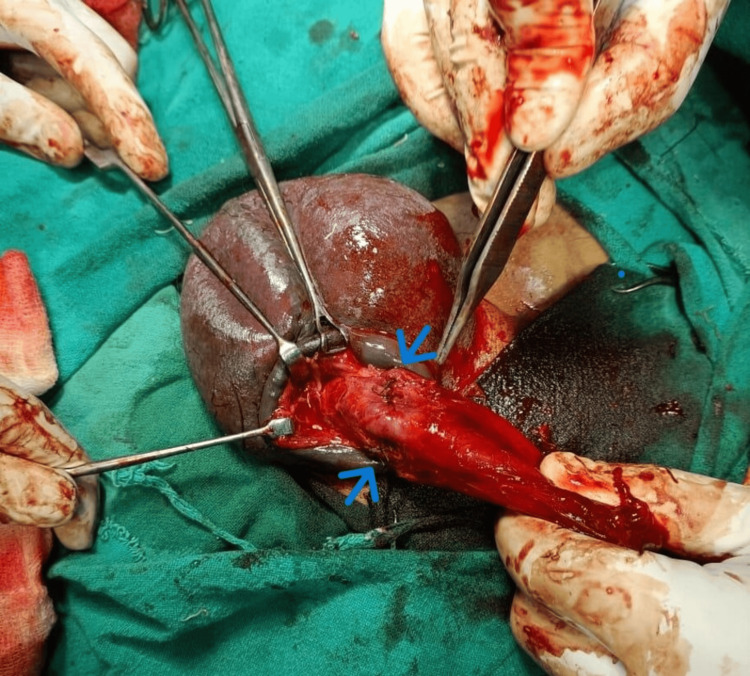 Figure 4
Figure 4 Figure 5
Figure 5| Grade | Description |
| 1 | Contusion or hematoma without urethral injury |
| 2 | Laceration involving the tunica albuginea without urethral injury |
| 3 | Laceration involving the tunica albuginea with urethral injury |
| 4 | Laceration involving the tunica albuginea with injury to the corpus spongiosum |
| 5 | Complete disruption of the penis including urethral injury |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsLibraries, Manuscripts, and Books · Archaeology and Cultural Heritage · Historical Art and Architecture Studies
Introduction
Penile fracture is an uncommon but serious urological condition resulting from the rupture of the tunica albuginea due to blunt trauma to an erect penis [1]. The tunica albuginea is a tough fibrous layer that surrounds the corpora cavernosa, and its rupture typically occurs during vigorous sexual intercourse or masturbation. In the United States, the estimated incidence is approximately 1 in 175,000 hospital admissions annually [2].
Double penile fractures, involving simultaneous ruptures of both corpora cavernosa, are exceedingly rare. There is limited literature on the exact incidence, but it is considered to be less than 2% of all penile fracture cases [3]. This report presents a unique case of a 38-year-old male with a double penile fracture following sexual intercourse.
Case presentation
A 38-year-old male presented to the emergency department 14 hours after experiencing acute penile pain and swelling during sexual intercourse. He reported hearing a sudden "cracking" sound, followed by immediate pain, penile deformity, and scrotal edema. Physical examination revealed a swollen, deviated penis with notable hematoma and scrotal edema with no blood at the tip of the urethral meatus, features suggestive of penile fracture (Figure 1). Urgent penile ultrasound also confirmed disruption of the tunica albuginea near the root of the penis, with a substantial hematoma present, no urethral injury was detected (Figure 2).
Penile deformity with penile and scrotal hematoma
Ultrasonographic image showing a defect in the tunica albuginea (between 1 and 2) of right CCPoints 1 and 2 represent the defect in the tunica albuginea.CC: Corpus cavernosum, CS: Corpus spongiosum
The patient was taken to the operating room for urgent surgical exploration. A circumferential subcoronal degloving incision was performed, exposing the penile shaft. Intraoperatively, there were bilateral corpus cavernosal tears near the penile root with hematoma with American Association for the Surgery of Trauma (AAST) grade 2 for penile fracture (Figure 3). The hematoma was meticulously evacuated, and the bilateral tears in the tunica albuginea were repaired using vicryl 3-0 absorbable sutures with a simple interrupted technique (Figure 4).
Bilateral cavernosal tear near penile root (arrows)
Post repair of bilateral tunica albuginea near root of penis using vicryl 3–0 sutures (arrows)
Postoperatively, the patient was discharged with a prescription for amoxicillin-clavulanate 625 mg to be taken thrice daily for seven days, along with a Foley catheter in situ. He was instructed to abstain from sexual activity and masturbation for at least four weeks and was educated on performing daily home dressing. The Foley catheter was subsequently removed after one week. At the third-week follow-up, the surgical site appeared healthy and free of discharge, and the patient reported no penile curvature during erection. He expressed satisfaction with the overall outcome (Figure 5).
Third-week follow-up showing significant reduction in edema of scrotum and penis with the suture line appearing healthy
Discussion
Penile fracture typically presents with immediate penile pain, swelling, and hematoma following trauma to an erect penis [4]. The incidence of penile fracture varies globally but is generally considered rare. Higher incidences have been reported in regions where cultural practices involve vigorous sexual activity or aggressive penile manipulation [5]. Bilateral corpus cavernosal tears, although rare, present similarly but may involve more extensive hematoma and deformity. The exact incidence of double penile fractures is not well documented, but it is believed to be less than 2% of all penile fracture cases [3].
The AAST has developed a grading system for penile fracture to help standardize the severity of the injury and guide treatment [6]. Table 1 explains the AAST grading of penile injury.
The algorithm for diagnosing penile fracture begins with clinical evaluation, which includes assessing the patient's history of trauma events and conducting a physical examination to check for penile swelling, ecchymosis, and deformity. An initial diagnosis is based on clinical suspicion derived from the history and physical exam [1]. If the diagnosis is uncertain or a urethral injury is suspected, imaging studies are recommended. Ultrasound, a non-invasive modality, can confirm the presence of tunica albuginea tears and detect hematoma [7]. An MRI offers high-resolution images of soft tissue structures, though it is less commonly used due to higher cost and limited availability in emergency settings [8]. By following this algorithm, healthcare providers can effectively diagnose and manage penile fractures.
Prompt surgical intervention is the mainstay of treatment for penile fractures to prevent long-term complications such as erectile dysfunction and penile curvature. The goal of surgery is to evacuate the hematoma, repair the tunica albuginea tear(s), and address any associated injuries, such as urethral damage [9]. Absorbable sutures are typically used to repair the tunica albuginea to minimize foreign body reactions and enhance healing [10].
This case highlights the importance of considering bilateral penile fracture in patients presenting with severe penile trauma and deformity. Surgical repair involves evacuation of the hematoma and meticulous suturing of the tunica albuginea to restore penile integrity and function.
Conclusions
A double penile fracture is a rare but serious urological emergency requiring prompt recognition and surgical management. This case demonstrates successful treatment through timely intervention, resulting in favorable functional outcomes. Clinicians should maintain a high index of suspicion for bilateral fractures in cases of significant penile trauma to ensure optimal patient recovery.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Progesterone: a novel adjunct to intravesical chemotherapy BJU Int Lewin J Cooper A Birch B 7367419020021241075810.1046/j.1464-410x.2002.03013.x · doi ↗ · pubmed ↗
- 2Factors associated with condom use among sexually active US adults, National Survey of Family Growth, 2006-2010 and 2011-2013 J Sex Med Nasrullah M Oraka E Chavez PR Johnson CH Di Nenno E 5415501420172836497910.1016/j.jsxm.2017.02.015PMC 5477642 · doi ↗ · pubmed ↗
- 3Does timing of presentation of penile fracture affect outcome of surgical intervention?Urology el-Assmy A el-Tholoth HS Mohsen T Ibrahiemel-HI 138813917720112144028910.1016/j.urology.2010.12.070 · doi ↗ · pubmed ↗
- 4Effect of transurethral resection of the prostate on erectile function: a prospective comparative study Int J Impot Res Jaidane M Arfa NB Hmida W Hidoussi A Slama A Sorba NB Mosbah F 1461512220101994085410.1038/ijir.2009.56 · doi ↗ · pubmed ↗
- 5Penile Fracture: Rupture of the Penis Corpora Urology Textbook Sawh C Crane D Ong C Wong C 2023 https://www.urology-textbook.com/penile-fracture.html#google_vignette
- 6Organ injury scaling: spleen and liver (1994 revision)J Trauma Moore EE Cogbill TH Jurkovich GJ Shackford SR Malangoni MA Champion HR 323324381995789770710.1097/00005373-199503000-00001 · doi ↗ · pubmed ↗
- 7Penile fracture: our experience in a tertiary care hospital Urol Ann Sanyal R Chatterjee U 273152013
- 8DNA damage in bovine sperm does not block fertilization and early embryonic development but induces apoptosis after the first cleavages J Androl Fatehi AN Bevers MM Schoevers E Roelen BA Colenbrander B Gadella BM 1761882720061630421210.2164/jandrol.04152 · doi ↗ · pubmed ↗