Clinical characterisation of exacerbations of severe eosinophilic asthma occurring on mepolizumab and placebo
Imran Howell, Daniel J. Bratton, Gareth Hynes, Steven W. Yancey, Liam G. Heaney, Ian D. Pavord, Rahul Shrimanker

TL;DR
This study compares asthma flare-ups in patients on mepolizumab and placebo, finding differences in lung function and recovery.
Contribution
The study provides new insights into the nature of asthma exacerbations during mepolizumab treatment.
Findings
Mepolizumab-treated exacerbations show less peak expiratory flow reduction compared to placebo.
Symptom scores are similar between mepolizumab and placebo groups during exacerbations.
Symptoms recover more slowly in mepolizumab-treated patients, suggesting less prednisolone responsiveness.
Abstract
Mepolizumab, a monoclonal antibody targeting interleukin (IL)-5, depletes circulating eosinophils and reduces exacerbations of severe eosinophilic asthma [1]. However, some people continue to exacerbate potentially due to different, less corticosteroid-responsive mechanisms [2]. To characterise the changes in symptom and lung function seen in on-biologic exacerbations, we conducted a post hoc comparison of diary card data from prednisolone-treated exacerbations occurring during treatment with mepolizumab or placebo in three placebo-controlled trials [1, 3, 4]. Asthma exacerbations in people treated with mepolizumab result in less peak expiratory flow reduction than placebo but similar symptom scores. Symptoms recover slower, indicating these exacerbations may be less prednisolone responsive. https://bit.ly/3xQsFRB
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
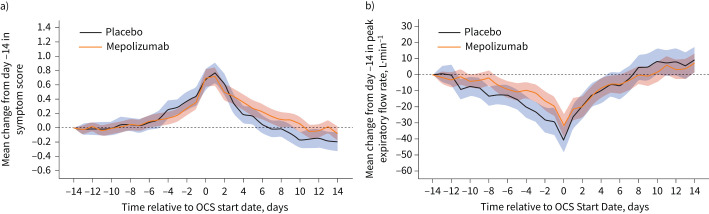 Figure 1
Figure 1- —NIHR Oxford Biomedical Research Centrehttp://dx.doi.org/10.13039/501100013373
- —GlaxoSmithKlinehttp://dx.doi.org/10.13039/100004330
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsAsthma and respiratory diseases · Respiratory and Cough-Related Research · Inhalation and Respiratory Drug Delivery
To the Editor:
Mepolizumab, a monoclonal antibody targeting interleukin (IL)-5, depletes circulating eosinophils and reduces exacerbations of severe eosinophilic asthma [1]. However, some people continue to exacerbate potentially due to different, less corticosteroid-responsive mechanisms [2]. To characterise the changes in symptom and lung function seen in on-biologic exacerbations, we conducted a post hoc comparison of diary card data from prednisolone-treated exacerbations occurring during treatment with mepolizumab or placebo in three placebo-controlled trials [1, 3, 4].
Diary card data were reviewed from three studies involving 1743 patients with severe eosinophilic asthma: DREAM [1], a 52-week study of three doses of mepolizumab (75, 250 or 750 mg intravenously, 4 weekly) versus placebo; MENSA [3], a 32-week study of two doses of mepolizumab (75 mg i.v. or 100 mg subcutaneously (s.c.), 4 weekly) versus placebo; and MUSCA [4], a 24-week study of mepolizumab 100 mg s.c., 4 weekly) versus placebo. All studies recruited patients with two or more exacerbations in the previous year and evidence of eosinophilic airway inflammation. As similar efficacy on exacerbation rate reduction has been shown across all doses of mepolizumab, these were combined.
Patients completed an electronic daily diary card during treatment, including a six-point symptom score assessing asthma symptoms in the previous 24 h (0: no symptoms; 5: worst symptoms) and a best-of-three morning peak expiratory flow (PEF) (in litres per minute). Exacerbations were defined as worsening symptoms requiring rescue oral corticosteroids (OCS) for ≥3 days. Exacerbations with ≥20 days of diary data in the period from 14 days prior to and after starting OCS (defined as day 0) were included in the analysis. Change from day −14 (i.e. 14 days prior to starting OCS) in PEF and symptom score were compared between treatment arms using unpaired t-tests. Rate of change in endpoints in the 7 days after OCS initiation (i.e. days 0–7) were compared between treatments using linear regression. For individuals with multiple events, within-subject means were derived prior to analysis.
During the studies, 322 (52%) patients on placebo and 419 (37%) patients on mepolizumab experienced one exacerbation or more. Sufficient diary card PEF data were available for 1021 exacerbations (473 occurring in 247 subjects on placebo and 548 in 331 subjects on mepolizumab). Sufficient symptom data were available for 1026 exacerbations (476 occurring in 248 patients on placebo and 550 in 332 patients on mepolizumab). Baseline mean±sd characteristics were similar between mepolizumab and placebo respectively: age 50±12 versus 50±13 years, female sex 63% versus 66%, body mass index 28.9±6.1 versus 28.4±6.5 kg·m^−2^, pre-bronchodilator forced expiratory volume in 1 s (FEV_1_) 57.3±17.2% versus 59.3±16.6% of predicted, geometric mean blood eosinophil count 0.23±1.1 versus 0.34±1.0 cells per mm^3^, day −14 PEF 245±108 versus 262±107 L·min^−1^ and day −14 symptom score 1.4±1.4 versus 1.6±1.3.
Exacerbations on placebo were associated with a larger mean drop in PEF compared to mepolizumab at day 0 versus day −14 (−39.0 versus −29.5 L·min^−1^, mean difference (95% CI) 9.5 (0.6–19.6) L·min^−1^) (figure 1), representing a 15% and 12% decrease from day −14 respectively. PEF from day 0 to 7 recovered at 4.8 and 3.6 L·min^−1^ per day (mean difference 1.2 (−0.2–2.6) L·min^−1^), representing a percentage of the total fall in PEF recovered per day of 12% for both treatments. The mean increase in daily symptom score at day 0 compared to day −14 was 0.64 and 0.68 points for placebo and mepolizumab (mean difference 0.03 (−0.15–0.22)) (figure 1), representing an increase of 44% and 45% from day −14 respectively. The rate of recovery of symptom scores from day 0 to 7 was 0.49 versus 0.40 points per week (mean difference 0.09 (−0.01–0.19) points per week), representing 19% and 13% of the total drop recovered per day for the placebo and mepolizumab groups (figure 1). The profile of symptoms and PEF from day −14 to 14 did not differ by mepolizumab dose.
In patients treated with mepolizumab, exacerbations resulted in shallower PEF reduction but similar increases in symptom scores. In contrast, the rate of recovery following treatment with prednisolone was similar for PEF but tended to be slower for symptoms scores. These findings suggest that some exacerbation events occurring in patients treated with mepolizumab are different and less prednisolone responsive. This supports the exacerbation heterogeneity in the MEX study. MEX characterised the exacerbations on mepolizumab and identified two groups: an exhaled nitric oxide fraction (FENO) and sputum eosinophil high group, and a FENO and sputum eosinophil low group who were often pathogen positive [2]. However, MEX did not assess clinical recovery after treatment with prednisolone.
In patients with COPD, noneosinophilic exacerbations are associated with a shallower fall in lung function and a slower symptom recovery after treatment with prednisolone compared to eosinophilic events [5]. Similarly, our findings suggest a distinct phenotype of exacerbation not prevented by mepolizumab treatment and less responsive to prednisolone. The presence of a mepolizumab-unresponsive exacerbation type is supported by results from two large placebo-controlled studies of mepolizumab in eosinophilic COPD. Exacerbations treated with antibiotics alone were not prevented by mepolizumab treatment, whereas OCS-treated events were prevented in a blood eosinophil-dependent manner [6].
We acknowledge that the changes in PEF at exacerbation and the differences in rate of recovery in symptoms were small. These were post hoc exploratory analyses, so we did not perform any hypothesis testing. Our findings should therefore be regarded as hypothesis generating rather than definitive. They provide some support for the view that on-biologic exacerbation mechanisms are heterogeneous. One possibility is that anti-IL-5 treatment shifts the balance to an increased proportion of infective exacerbations, although patients displaying broader epithelial activation may still be prednisolone-responsive [7]. Better characterisation of exacerbations based on their biology might prevent prednisolone use with an unfavourable risk/benefit balance.
There are additional limitations to our study. First, ∼20% of exacerbations were excluded due to insufficient diary card data. This was unlikely to cause bias because these patients had similar baseline characteristics to included patients. Second, we included all doses of mepolizumab as they have similar efficacy. We observed no relationship between mepolizumab dose and the profile of exacerbations, so it is unlikely that higher doses, which reduce sputum eosinophils more completely [1], affect the response to prednisolone. Third, we used mean data from each patient to reduce the possibility of frequently exacerbating patients skewing the analysis, which may be overly conservative. Fourth, our earlier study [8] identified a shallower increase in symptom scores but a similar fall in FEV_1_ between on-mepolizumab versus placebo exacerbations, whereas this study showed a reduction in PEF fall but no difference in symptom scores. The use of different measures of symptoms and lung function complicates this comparison. Collectively, both studies imply less severe and prednisolone-responsive events in patients treated with mepolizumab. Fifth, since FENO and blood eosinophils were not measured at exacerbation, we cannot comment on the biological characterisation of the exacerbations. Finally, to account for potential bias and overtreatment with prednisolone, all exacerbations in the DREAM and MENSA clinical trials were corroborated by diary card review. Since a very low percentage of events were rejected, this was not applied to the more recent MUSCA study. Nevertheless, this validation step could have reduced the true between-treatment differences in exacerbation severity.
Prospective studies are needed to determine whether mepolizumab exacerbation events have different inflammatory mechanisms, triggers and oral corticosteroid response [9].
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Pavord ID, Korn S, Howarth P, et al. Mepolizumab for severe eosinophilic asthma (DREAM): a multicentre, double-blind, placebo-controlled trial. Lancet 2012; 380: 651–659. doi:10.1016/S 0140-6736(12)60988-X 22901886 · doi ↗ · pubmed ↗
- 2Mc Dowell PJ, Diver S, Yang F, et al. The inflammatory profile of exacerbations in patients with severe refractory eosinophilic asthma receiving mepolizumab (the MEX study): a prospective observational study. Lancet Respir Med 2021; 9: 1174–1184. doi:10.1016/S 2213-2600(21)00004-733971168 · doi ↗ · pubmed ↗
- 3Ortega HG, Liu MC, Pavord ID, et al. Mepolizumab treatment in patients with severe eosinophilic asthma. N Engl J Med 2014; 371: 1198–1207. doi:10.1056/NEJ Moa 140329025199059 · doi ↗ · pubmed ↗
- 4Chupp GL, Bradford ES, Albers FC, et al. Efficacy of mepolizumab add-on therapy on health-related quality of life and markers of asthma control in severe eosinophilic asthma (MUSCA): a randomised, double-blind, placebo-controlled, parallel-group, multicentre, phase 3b trial. Lancet Respir Med 2017; 5: 390–400. doi:10.1016/S 2213-2600(17)30125-X 28395936 · doi ↗ · pubmed ↗
- 5Bafadhel M, Mc Kenna S, Terry S, et al. Blood eosinophils to direct corticosteroid treatment of exacerbations of chronic obstructive pulmonary disease: a randomized placebo-controlled trial. Am J Respir Crit Care Med 2012; 186: 48–55. doi:10.1164/rccm.201108-1553 OC 22447964 PMC 3400995 · doi ↗ · pubmed ↗
- 6Pavord ID, Chanez P, Criner GJ, et al. Mepolizumab for eosinophilic chronic obstructive pulmonary disease. N Engl J Med 2017; 377: 1613–1629. doi:10.1056/NEJ Moa 170820828893134 · doi ↗ · pubmed ↗
- 7Howell I, Yang F, Brown V, et al. Anti-inflammatory effects of oral prednisolone at stable state in people treated with mepolizumab: a proteomic and bulk transcriptomics analysis. med Rxiv 2024; pre print [10.1101/2024.02.14.24302812]. · doi ↗
- 8Shrimanker R, Pavord ID, Yancey S, et al. Exacerbations of severe asthma in patients treated with mepolizumab. Eur Respir J 2018; 52: 1801127. doi:10.1183/13993003.01127-201830464012 · doi ↗ · pubmed ↗