Bilateral Renal Vein Thrombosis and Chylous Ascites in Phospholipase A2 Receptor-Associated Membranous Nephropathy: A Case Report
Kazushige Shiraishi, FNU Chesta, Yoshito Nishimura, Christina M Chong

TL;DR
This case report describes a rare combination of chylous ascites and bilateral renal vein thrombosis in a patient with PLA2R-associated membranous nephropathy, successfully treated with anticoagulation and rituximab.
Contribution
This is the first reported case of PLA2R-associated membranous nephropathy presenting with both chylous ascites and bilateral renal vein thrombosis.
Findings
PLA2R-associated membranous nephropathy can present with rare complications such as chylous ascites and bilateral renal vein thrombosis.
Anticoagulation and rituximab were effective in managing the patient's condition.
The case suggests a possible link between renal vein thrombosis and lymphatic fluid leakage leading to chylous ascites.
Abstract
Phospholipase A2 receptor (PLA2R)-associated membranous nephropathy is an important cause of nephrotic syndrome that can lead to a variety of systemic manifestations. Chylous ascites and bilateral renal vein thrombosis are rare manifestations in adult nephrotic syndrome, and there have been no reported cases demonstrating both chylous ascites and bilateral renal vein thrombosis in patients with PLA2R-associated membranous nephropathy. Here, we report the first case of PLA2R-associated membranous nephropathy complicated by renal vein thrombosis and chylous ascites successfully treated with anticoagulation and rituximab. A 65-year-old African American male presented with abdominal pain for four days, hematochezia for one day, and lower extremity edema for one year. Blood pressure was 158/73 mmHg and other vital signs were normal. Physical examination revealed abdominal distention,…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
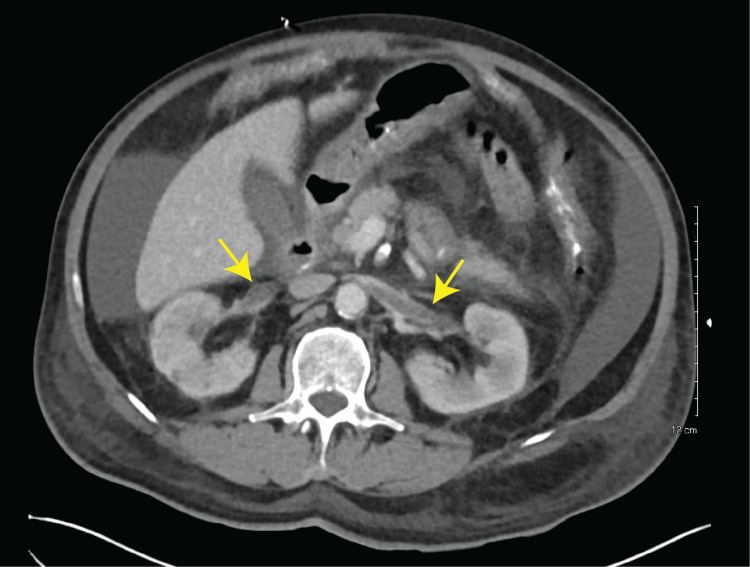 Figure 1
Figure 1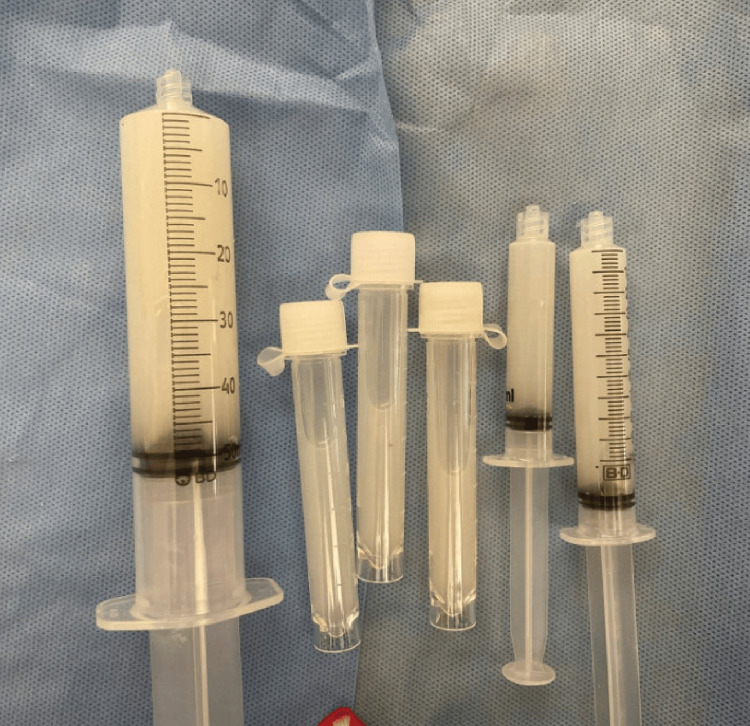 Figure 2
Figure 2|
Table | ||||
| WBC | 11.70 x 103/μL | Total cholesterol | 222 mg/dL | |
| Hemoglobin | 10.3 g/dL | HDL cholesterol | 41 mg/dL | |
| Hematocrit | 29.70% | Triglycerides | 245 mg/dL | |
| Platelet | 315 x 103/μL | Urine protein | (4+) | |
| Na | 141 mEq/L | 6.4 g/day | ||
| K | 2.9 mEq/L | Urine blood | Mod | |
| Cl | 115 mEq/L | Anti-PLA2R Antibody | 1:2560 | |
| Glucose | 112 mg/dL | ANA | <40 | |
| BUN | 15 mg/dL | ANCA | Negative | |
| Creatinine | 1.9 mg/dL | HBs Antigen | Negative | |
| Total protein | 5.0 g/dL | Anti-HBs Antibody | Positive | |
| Albumin | 2.0 g/dL | Anti-HBc Antibody | Negative | |
| AST (SGOT) | 17 IU/L | Anti-HCV Antibody | Negative | |
| ALT (SGPT) | 11 IU/L | Rapid Plasma Reagin | Non-reactive | |
| ALP | 118 IU/L | C3 | 119 mg/dL | |
| Total Bilirubin | <0.2 mg/dL | C4 | 46 mg/dL | |
| LDH | 329 IU/L | SPEP | No monoclonal protein | |
| PT-INR | 1.1 | UPEP | No monoclonal protein | |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsRenal Diseases and Glomerulopathies · Autoimmune Bullous Skin Diseases · Coagulation, Bradykinin, Polyphosphates, and Angioedema
Introduction
Phospholipase A2 receptor (PLA2R)-associated membranous nephropathy is one of the most common causes of nephrotic syndrome, resulting in diverse systemic manifestations [1]. Chylous ascites and renal vein thrombosis are rare complications of nephrotic syndrome [2], and their pathophysiology in the context of nephrotic syndrome is unclear. There have been no cases showing chylous ascites and bilateral renal vein thrombosis in a patient with PLA2R-associated membranous nephropathy. Herein, we present the first case of chylous ascites and bilateral renal vein thrombosis secondary to nephrotic syndrome due to PLA2R-associated membranous nephropathy successfully treated with anticoagulation and rituximab.
Case presentation
A 65-year-old African American male with a history of hypertension and peripheral artery disease presented with acute-onset abdominal pain for four days, hematochezia for one day, and worsening lower extremity edema up to the thigh for one year. One year prior to admission, the patient noticed bilateral lower extremity edema which extended to his thighs five months prior to admission. Four days prior to admission, the patient noticed abdominal distention then developed acute onset abdominal pain and hematochezia.
Physical examination revealed a well-nourished male in no distress with a blood pressure of 158/73 mmHg and normal temperature, pulse, and respirations. Cardiac and pulmonary examinations were normal. The abdomen was distended with periumbilical tenderness and normal bowel sounds without rebound or guarding. Shifting dullness was not clear. Bilateral pitting edema extending to the thighs was noted. Rectal examination showed bright red blood. Laboratory analysis (Table 1) was remarkable for hemoglobin 10.3 g/dL and findings suggesting nephrotic syndrome (blood urea nitrogen 15 mg/dL, creatinine 1.9 mg/dL [baseline 1.1 mg/dL, six years prior to admission], albumin 2.0 g/dL, total protein 5.0 g/dL, cholesterol 222 mg/dL, and triglycerides 245 mg/dL), with significant proteinuria of 6452 mg on 24-hour urine protein collection.
Abdominal contrast computed tomography (CT) showed non-occlusive bilateral renal vein thrombosis with moderate amount of ascites without other significant findings (Figure 1). Paracentesis was performed for his ascites to exclude the possibility of spontaneous bacterial peritonitis. Ascitic fluid was milky white (Figure 2), suggesting chylous ascites. Ascitic chemistry analysis revealed low cholesterol (10 mg/dL) and high triglycerides (131 mg/dL). Ascitic fluid culture was negative.
Abdominal CT scan with contrast revealed bilateral renal vein thrombosis and ascitesAbdominal CT scan with contrast showed bilateral renal vein thrombosis. Yellow arrows indicate renal vein thrombosis.
Chylous ascites obtained from paracentesisPicture showing milky white chylous ascites obtained by paracentesis performed on the day of admission.
On admission, the patient was started on an intravenous continuous heparin infusion for the treatment of bilateral renal vein thrombosis. On day three, the patient underwent esophagoduodenoscopy and colonoscopy to evaluate for any source of bleeding for his hematochezia and for malignancy given nephrotic syndrome. The studies showed few localized diminutive erosions with no bleeding and no stigmata of recent bleeding in the stomach and non-bleeding external and internal hemorrhoids, but were negative for detecting an active source of bleeding or malignancy. He did not have further signs of gastrointestinal bleeding, and the cause of hematochezia was thought to be secondary to gastric erosions or hemorrhoids.
Initial workup for nephrotic syndrome was positive for anti-PLA2R antibody titer at 1:2560. Additional negative workup included: antinuclear antibody (ANA); anti-neutrophil cytoplasmic antibody (ANCA); hepatitis B and C infection screening; HIV infection; rapid plasma reagin; and monoclonal protein from serum and urine protein electrophoresis (Table 1). Complement components 3 and 4 levels were not decreased. Kidney biopsy was offered but the patient opted out due to bleeding risk. Following Kidney Disease Improving Global Outcomes (KDIGO) clinical practice guidelines, the patient was diagnosed with membranous nephropathy based on anti-PLA2R antibody levels [3]. Chest CT was negative for malignancy that could explain his membranous nephropathy. The patient was considered at high risk for progressive loss of kidney function [3], and rituximab was started during the hospital stay, which successfully controlled the disease activity. The patient was eventually discharged on warfarin, torsemide, and lisinopril with nephrology follow-up. There was no ascites on physical examination one month after discharge.
Discussion
To our knowledge, this is the first case of PLA2R-associated membranous nephropathy complicated by bilateral renal vein thrombosis and chylous ascites successfully treated with anticoagulation and rituximab. The prevalence, characteristics, and management of chylous ascites in nephrotic syndrome remain unclear [4]. This uncertainty is likely because clinicians often do not perform paracentesis when ascites is present in patients with nephrotic syndrome, as they typically attribute the cause of ascites to third spacing. However, due to the possibility of concurrent infection or malignancy, paracentesis should be performed in these cases. Low ascitic cholesterol levels (10-62 mg/dL) and high ascitic triglycerides (90-529 mg/dL) with a triglyceride to cholesterol ratio greater than 7.0 were previously reported as good indicators for the diagnosis of chylous ascites in nephrotic syndrome [5]. Our patient’s laboratory findings were all consistent with these numbers.
The etiology of chylous ascites in nephrotic syndrome is unclear. Some studies attribute the causes to possible bowel edema induced by hypoalbuminemia [5-7]. Our case suggests a possible association between bilateral renal thrombosis and chylous ascites. A tempting hypothesis is that renal thrombosis increases renal lymphatic pressure, leading to leakage of lymphatic fluid into the peritoneal space. Similar pathophysiology of chylothorax is seen in patients with central venous thrombosis [8].
The renal lymphatic system has been suggested to act as a "safety valve" to protect the kidney from elevated intrarenal pressures in the setting of renal vein thrombosis [9]. This has been shown experimentally by occluding the renal vein in animals, causing a dramatic increase in lymphatic pressure as measured by catheterization of the renal capsule lymphatic vessel [10]. There are technical limitations to understanding the pathophysiology of chylous ascites in nephrotic syndrome because renal lymphatics cannot be visualized in humans with existing methods [9]. The invention of further imaging techniques, including injection of the probe into the renal interstitium, may be needed to elucidate the fundamental mechanisms of chylous ascites in nephrotic syndrome.
Conclusions
We are reporting a case of PLA2R-associated membranous nephropathy complicated by chylous ascites and bilateral renal vein thrombosis that was effectively treated with anticoagulation and rituximab. The effective treatment of our patient with both anticoagulation and rituximab highlights the potential efficacy of this treatment strategy in similar cases. Our case also raises interesting questions about the underlying pathophysiology linking membranous nephropathy, chylous ascites, and renal vein thrombosis. Further research is warranted to establish evidence-based treatment strategies for patients with PLA2R-associated membranous nephropathy with chylous ascites and renal vein thrombosis.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1M-type phospholipase A 2 receptor as target antigen in idiopathic membranous nephropathy N Engl J Med Beck LH Jr Bonegio RG Lambeau G 112136120091957127910.1056/NEJ Moa 0810457 PMC 2762083 · doi ↗ · pubmed ↗
- 2Renal vein thrombosis Eur J Vasc Endovasc Surg Asghar M Ahmed K Shah SS Siddique MK Dasgupta P Khan MS 2172233420071754355610.1016/j.ejvs.2007.02.017 · doi ↗ · pubmed ↗
- 3KDIGO 2021 clinical practice guideline for the management of glomerular diseases Kidney Int 0100202110.1016/j.kint.2021.05.02134556256 · doi ↗ · pubmed ↗
- 4Chylous ascites and the nephrotic syndrome. Report of a case, associated with renal vein thrombosis Am J Med Lindenbaum J Scheidt SS 830836441968564642810.1016/0002-9343(68)90262-3 · doi ↗ · pubmed ↗
- 5Chylous ascites in an adult patient with nephrotic syndrome due to membranous nephropathy Nephron Kato A Kohno S Ohtake T Takita T Hirshida A 3613628920011159840710.1159/000046103 · doi ↗ · pubmed ↗
- 6Chylous ascites and chylothorax due to the existence of transdiaphragmatic shunting in an adult with nephrotic syndrome Nephrol Dial Transplant Chen YC Kuo MC Chen HC Liu MQ Hwang SJ 150115022020051578463410.1093/ndt/gfh 791 · doi ↗ · pubmed ↗
- 7Chylous ascites and chylothorax due to membranous nephropathy Clin Nephrol Colak HB Alicil T Tekce H Oz D Erol A Aras F Kursat S 3333346720071754234510.5414/cnp 67333 · doi ↗ · pubmed ↗
- 8Chylothorax and central vein thrombosis, an under-recognized association: a case series Respirol Case Rep Kho SS Tie ST Chan SK Yong MC Chai SL Voon PJ 05201710.1002/rcr 2.221PMC 532587328250931 · doi ↗ · pubmed ↗