Asciminib Use Highlighting Underlying Moyamoya Disease: A Case Report
Saloni Savani, Arpita Pawa, Naved Salim, Tithi Savani, Samip Master

TL;DR
A patient with chronic myeloid leukemia developed Moyamoya disease after starting asciminib therapy, suggesting a possible rare side effect.
Contribution
This case report highlights a potential association between asciminib use and the development of Moyamoya disease.
Findings
A patient with CML developed Moyamoya disease after starting asciminib therapy.
Discontinuation of asciminib led to improvement in the patient's symptoms.
No prior literature links asciminib to Moyamoya disease.
Abstract
We highlight here a case of Moyamoya disease (MMD) developed after treatment for chronic myeloid leukemia (CML). Moyamoya, a term meaning "a hazy puff of smoke" in Japanese, denotes a chronic occlusive cerebrovascular condition involving bilateral stenosis or closure of the terminal part of the internal carotid arteries (ICAs) and the proximal sections of the anterior cerebral arteries (ACAs) and middle cerebral arteries (MCAs) resulting in the development of abnormal vascular collaterals. A 40-year-old African-American female with a past medical history of CML presented to the oncology clinic with expressive aphasia. Of note, she was diagnosed with CML eight years ago and was previously treated with dasatinib and nilotinib with only partial remission. She tested positive for the T315I mutation and was initiated on asciminib therapy about a month before her symptoms surfaced.…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
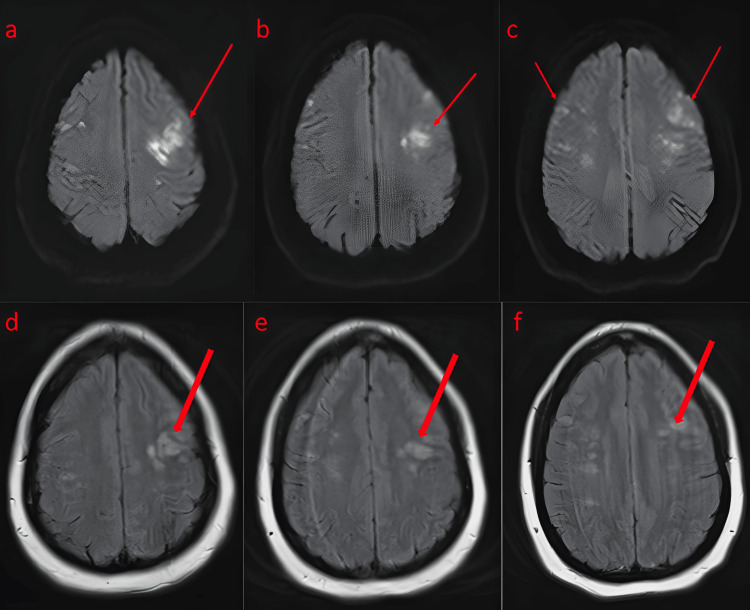 Figure 1
Figure 1 Figure 2
Figure 2| Results | |
| BCR-ABL Specimen Type, Blood | WB EDTA (VC) |
| BCR-ABL Fusion Form, Blood | 210 (VC) |
| BCR-ABL Final Diagnosis, Blood | See below |
| Comment: | Peripheral blood, BCR-ABL1 kinase domain mutation analysis: positive. Mutation identified in the BCR-ABL 1 kinase domain region. This mutation and its corresponding amino acid change is g. 133748283CT; p.Thr315lle (T315I). The T315I mutation is associated with pan-resistance to nearly all TKIs but is sensitive to ponatinib and asciminib |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsMoyamoya disease diagnosis and treatment · Macrophage Migration Inhibitory Factor · Peptidase Inhibition and Analysis
Introduction
Moyamoya disease (MMD) denotes a chronic occlusive cerebrovascular condition involving bilateral stenosis or closure of the terminal part of the internal carotid arteries (ICAs) and the proximal sections of the anterior cerebral arteries (ACAs) and middle cerebral arteries (MCAs), resulting in abnormal vascular collaterals. There are four presentations related to MMD: ischemic, epileptic, hemorrhagic, and other [1]. Moyamoya roughly translates to "a hazy puff of smoke" in Japanese. The collateral vessels formed to compensate for the progressive stenosis have a “hazy” or “smokey” appearance on cerebral angiographic imaging [2]. This disease is most prevalent in two different age ranges: approximately 10 years old and between 30 to 45 years old. Both children and adults commonly experience ischemic symptoms, including transient ischemic attacks (TIAs). However, adults are more prone to intracranial hemorrhages compared to children [3].
Asciminib is an allosteric inhibitor targeting breakpoint cluster region-abelson murine leukemia 1 (BCR-ABL1) kinase activity that has gained approval for treating patients diagnosed with chronic-phase chronic myeloid leukemia (CML) who have not responded to two prior lines of therapy or for those carrying the T315I mutation [4]. Common side effects of tyrosine kinase inhibitor (TKI) therapy include edema, nausea, hypothyroidism, vomiting, and diarrhea. TKI therapy has also been known to cause adverse cardiovascular effects such as hypertension, atrial fibrillation, and heart failure. Newer generation TKIs, such as nilotinib, have shown an increased association with vascular adverse events [5,6]. No literature currently reports microvascular or cerebrovascular events specifically associated with asciminib therapy.
This report aims to highlight the potential association between TKI therapy, specifically asciminib, and cardiovascular complications. We report here a patient with CML who developed expressive aphasia one month after being started on asciminib therapy and was found to have characteristic brain imaging findings consistent with MMD, introducing the possibility of the medication having a potential cardiovascular side effect profile.
Case presentation
A 40-year-old African-American female with a past medical history of CML presented to the oncology clinic with expressive aphasia. She reported difficulty speaking but denied any other neurological symptoms like numbness, weakness, or tingling. These symptoms began a month prior and she was evaluated in the emergency room with a computed tomography (CT) scan of the head, which was negative for any acute abnormalities. During her clinic visit, she continued to experience word-finding difficulty, and the decision was made to admit the patient for a full neurological workup. The patient was diagnosed with CML eight years ago and was previously treated with dasatinib and nilotinib with only partial remission. Further genetic testing was performed, which indicated that she was positive for the T315I mutation (Table 1). Following this, the patient was initiated on a specifically targeting ABL myristoyl pocket (STAMP) inhibitor, asciminib, about a month before her symptoms began.
During her admission, the patient underwent a brain magnetic resonance imaging (MRI) that revealed multiple foci of cortical/subcortical restricted diffusion in the cerebral hemispheres bilaterally, predominantly in the frontal lobes, with findings compatible with acute/subacute infarction (Figure 1).
MRI brain with diffusion-weighted imaging sequence showing multiple foci of cortical/subcortical restricted diffusion in the cerebral hemispheres bilaterally, including the temporal lobes (a) and subcortical regions (b). Lesions were found predominantly in the frontal lobes (c) within the watershed distribution, compatible with acute/subacute infarctions. Also shown are FLAIR images (d,e,f), which display acute/subacute infarctsMRI: magnetic resonance imaging
A CT angiogram of the head showed moderate to severe narrowing at the origins of the bilateral MCA-M1 segment and ACA-A2 segment, which were patent distally, concerning Moyamoya syndrome (Figure 2).
CT angiogram head and neck: moderate to severe narrowing at the origins of the bilateral MCA M1 segment and ACA A2 segment, which were patent distally. (a) Coronal view, (b) sagittal view, and (c) transverse view (red arrows identifying affected areas)CT: computed tomography; MCA: middle cerebral artery; ACA: anterior cerebral artery
Given the lack of cardiovascular risk factors, underlying vasculitis was considered a differential, and a battery of autoimmune investigations was sent, all of which were negative. Additionally, these imaging findings were consistent with that of MMD. The patient followed closely with neurology and oncology. Due to the high index of suspicion, asciminib was discontinued, and the patient was referred for bone marrow transplant evaluation and concurrently started on cytarabine + peginterferon. The patient had improvement in her symptoms of aphasia after the drug was discontinued and returned to her baseline functional status.
Discussion
Asciminib, a STAMP inhibitor, has been used in patients with chronic-phase CML resistance or the setting of intolerance to ≥2 prior TKIs and those with T315I mutation [12]. The emergence of the T315I mutation stands as the primary resistance mechanism observed in patients with CML against both first- and second-generation TKIs [13]. T315I mutation is a change in the BCR-ABL fusion protein that confers resistance to most TKIs necessitating the use of other agents. Asciminib attaches to a myristoyl site on the BCR-ABL1 protein. This binding action effectively traps BCR-ABL1 in an inactive state, employing a mechanism different from other ABL kinase inhibitors [11]. Over the past decade, ponatinib has been the primary treatment choice in this scenario. However, when administered at its maximum dose (45 mg/day), there is a considerable risk of serious vascular occlusive events. Lower doses reduce this risk but also diminish effectiveness. These recent therapeutic advancements mean that for many resistant chronic-phase CML patients who have failed multiple TKIs, two options are now available: adjusted-dose ponatinib and asciminib [14].
Asciminib treatment continues until either the disease worsens or side effects become intolerable. Side effects are more common with higher doses and affect almost all patients. These side effects include anemia, neutropenia, muscle pain, fatigue, headache, rash, and diarrhea. Some severe but less common adverse events may occur such as severe bone marrow suppression, pancreatitis, high blood pressure, hypersensitivity reactions, embryo-fetal toxicity, and cardiovascular toxicity [15].
MMD is a chronic condition characterized by bilateral progressive narrowing of the terminal intracranial portion of the ICA and the circle of Willis. Its underlying cause remains unknown. MMD is often associated with inherited conditions such as sickle cell disease or trait, down syndrome, and neurofibromatosis type 1 as well as acquired conditions including head and/or neck irradiation, chronic meningitis, skull base tumors, atherosclerosis of skull base arteries, arteriosclerosis, and cerebral vasculitis. MMD exhibits a bimodal age distribution with the first peak occurring during the first decade of life and the second peak occurring in the fourth decade. The most frequent manifestation in Moyamoya patients is cerebral ischemic events such as TIAs or ischemic infarcts. Intracerebral hemorrhage predominantly occurs in adult patients with MMD. Seizures can occur in both adults and children. Symptoms can be classified based on their cause: those resulting from cerebral ischemia (such as stroke, TIA, and seizures) and those arising from the development of collateral vessels that compensate for ischemia (such as hemorrhage and headaches) [16].
New generation TKIs, including nilotinib and ponatinib, have been shown to cause cerebrovascular complications, including ischemic stroke [17]. Our report here represents a case of underlying MMD, which was unmasked in a patient recently initiated on asciminib therapy. Whether the patient had developed MMD secondary to underlying stroke risk factors or the previous use of TKIs known to predispose to stroke remains uncertain. The literature on the association between this medication and cardiovascular side effects is sparse [18]. However, our report highlights the potential for the drug to cause significant cardiovascular side effects.
Given our findings, patients placed on TKI therapy for CML need to be managed with extra precautions. This is especially important in cases involving patients with other comorbidities for stroke including renal disease, diabetes, hypertension, and cancer. Lifestyle modification should be emphasized in these patients. Optimal blood pressure control may also be necessary to mitigate the risk of developing MMD in patients started on TKI therapy.
Conclusions
This case underscores the importance of exercising extra caution when considering asciminib treatment for patients with pre-existing stroke risk factors or a history of stroke. As such, careful observation and expectant management are imperative to ensure patient safety and optimize therapeutic outcomes.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Moyamoya disease: a summary Neurosurg Focus Burke GM Burke AM Sherma AK Hurley MC Batjer HH Bendok BR 026200910.3171/2009.1.FOCUS 0831019335127 · doi ↗ · pubmed ↗
- 2Moyamoya disease and syndrome: a review Radiol Bras Demartini Z Jr Teixeira BC Koppe GL Gatto LA Roman A Munhoz RP 31375520223521066210.1590/0100-3984.2021.0010 PMC 8864689 · doi ↗ · pubmed ↗
- 3Moyamoya disease Front Neurol Neurosci Fujimura M Bang OY Kim JS 2042204020162796017510.1159/000448314 · doi ↗ · pubmed ↗
- 4Asciminib: a new therapeutic option in chronic-phase CML with treatment failure Blood Yeung DT Shanmuganathan N Hughes TP 3474347913920223546818010.1182/blood.2021014689 · doi ↗ · pubmed ↗
- 5Adverse effects of tyrosine kinase inhibitors in cancer therapy: pathophysiology, mechanisms and clinical management Signal Transduct Target Ther Shyam Sunder S Sharma UC Pokharel S 262820233741475610.1038/s 41392-023-01469-6PMC 10326056 · doi ↗ · pubmed ↗
- 6Tyrosine kinase inhibitors and vascular adverse events in patients with chronic myeloid leukemia: a population-based, propensity score-matched cohort study Oncologist Chen MT Huang ST Lin CW Ko BS Chen WJ Huang HH Hsiao FY 9749822620213441822010.1002/onco.13944 PMC 8571737 · doi ↗ · pubmed ↗
- 7European Leukemia Net recommendations for the management of chronic myeloid leukemia: 2013 Blood Baccarani M Deininger MW Rosti G 87288412220132380370910.1182/blood-2013-05-501569 PMC 4915804 · doi ↗ · pubmed ↗
- 8BCR-ABL kinase domain mutation analysis in chronic myeloid leukemia patients treated with tyrosine kinase inhibitors: recommendations from an expert panel on behalf of European Leukemia Net Blood Soverini S Hochhaus A Nicolini FE 1208121511820112156204010.1182/blood-2010-12-326405 · doi ↗ · pubmed ↗