Anterior Levator Muscle Resection and Switch in a Patient With Severe Blepharoptosis and Poor Bell’s Phenomenon: A Case Report
Fatema Aljufairi, Lee Cheuk Lam, Jake Uy Sebastian, Kenneth Lai, Kelvin Chong

TL;DR
A new surgical technique called 'levator switch' is introduced to correct severe eyelid drooping in patients with poor eye movement.
Contribution
The novel 'levator switch' technique repurposes resected tissue to improve eyelid function while preserving glandular structures.
Findings
The 'levator switch' successfully elevated the eyelid margin and stabilized the palpebral fissure height.
The procedure preserves the tarsus and meibomian glands, offering advantages over existing methods.
It minimizes postoperative corneal exposure in patients with poor Bell’s phenomenon.
Abstract
This case report describes a novel surgical technique, the "levator switch," for correcting severe blepharoptosis in a 65-year-old man with poor Bell's phenomenon following previous bilateral ptosis surgery. He presented with recurrent ptosis, weak levator function, and excessive frontalis muscle use. The technique involves a sequential approach: anterior levator resection followed by repurposing the resected tissue as a posterior lamellar graft to the lower tarsal border. This elevates the eyelid margin while maintaining a stable palpebral fissure height. The levator switch addresses ptosis from poor levator function and minimizes postoperative corneal exposure. It offers advantages over the existing tarsal switch procedure by preserving the tarsus and meibomian glands, thus maintaining eyelid stability and contour.
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
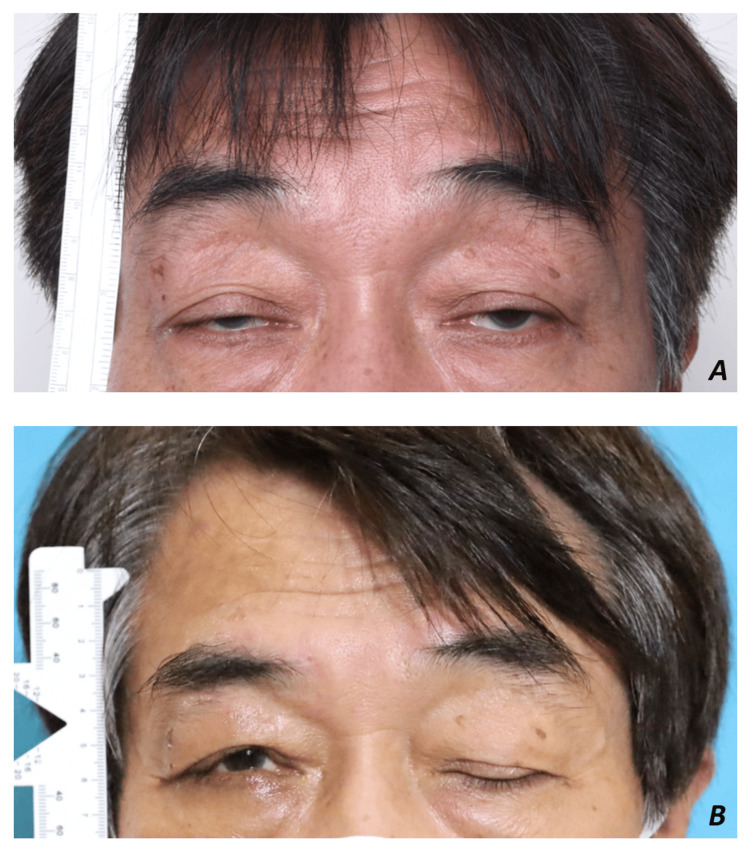 Figure 1
Figure 1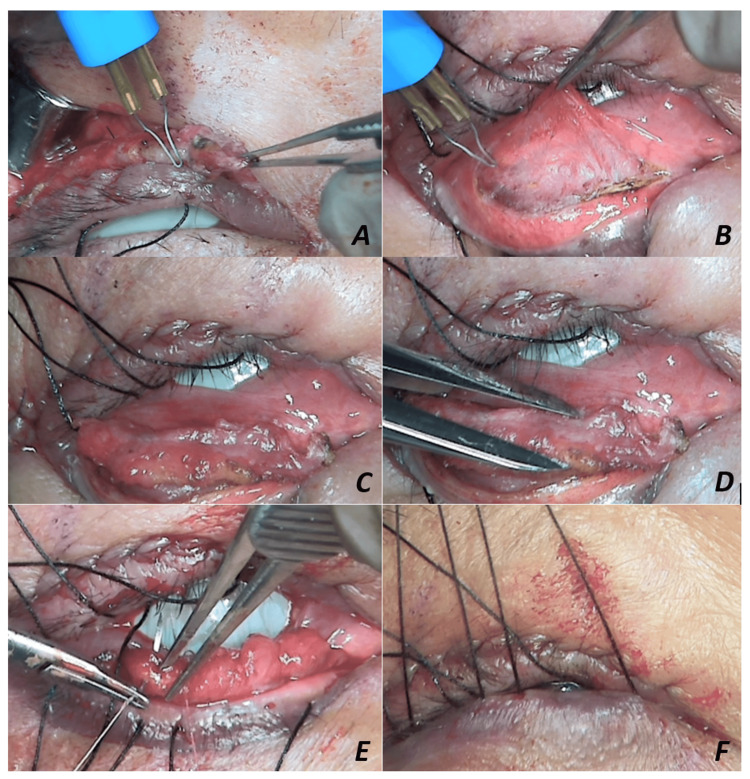 Figure 2
Figure 2| Author (year) | No. of cases | Methods | Outcomes | MRD1 (Median) | MRD2 (Median) | Palpebral fissure |
| DeMartelaere et al. (2006) [ | 26 eyelids (14 patients) | Posterior approach tarsal switch procedure | Thirteen patients (93%) recovered fully. Fourteen patients had palpebral fissure repositioned cephalad. No intraoperative complications. Fourteen patients were satisfied. One patient developed lagophthalmos postoperative. | NA | NA | NA |
| Lucci et al. (2009) [ | 9 eyelids (6 patients) | Posterior approach tarsal switch procedure | The palpebral fissure repositioned cephalad, unmasking their visual axis in the primary position, leading to improvement in their head position. No exposure symptoms postoperatively. | NA | NA | 4.1 mm (range, 3 to 5 mm) |
| Lenake and McNab (2017) [ | 6 eyelids (9 patients) | Posterior approach tarsal switch procedure | No intraoperative complications. No significant corneal exposure. No revision required over a follow-up period of six to 52 months (mean 16 months). | Median: 4.5 mm; mean: 2.3 mm (+1.5 mm) | Median: 2.5 mm; mean: 1.6 mm (-0.5 mm) | NA |
| Meneghim et al. (2018) [ | 18 eyelids (11 patients) | Anterior approach tarsal switch procedure | Postoperatively: Good lid margin contour Improved chin position. Patients were satisfied with the surgical outcomes. One patient's lower lid was poorly positioned and a tarsal strip procedure was done for correction. One patient at 10 months postoperatively had a recurrence of ptosis corrected with resection of the levator aponeurosis. One patient developed punctate keratitis postoperatively, which improved with topical lubricants. | From 0.0 mm to 1.0 mm (median, +1.75 mm; mean, +2.3 mm; range, +0 to 7 mm) | From 4.5 mm to 3.0 mm (median, -1.5 mm; mean, -1.8 mm) | From 4.0 mm to 4.0 mm (mean, +0.8 mm; range, −1.5 to 7 mm) |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsFacial Rejuvenation and Surgery Techniques · Facial Nerve Paralysis Treatment and Research · Botulinum Toxin and Related Neurological Disorders
Introduction
Blepharoptosis, also known as ptosis, refers to the drooping of the upper eyelid in a straight-ahead gaze [1]. This condition can be caused by congenital factors present at birth or acquired later in life. Acquired ptosis can have various causes, including aponeurotic, neurogenic, myogenic, traumatic, and mechanical [2]. Myopathic ptosis can cause impaired ocular movement and weak orbicularis oculi muscle, which results in poor Bell's phenomenon that increases the risk of corneal exposure postoperatively [3].
The surgical correction of ptosis can be a challenging task, particularly in cases where the levator muscle function is suboptimal [4]. The severity of the condition requires a specialized approach tailored to the specific needs of the patient. However, while tarsal resection can improve the appearance of the eyelid, it can also lead to corneal exposure, dry eyes, and meibomian gland dysfunction [5]. Anterior levator muscle switch is a novel surgical technique used to address patients with severe blepharoptosis with co-existing poor Bell's phenomenon. We present a case of anterior levator muscle resection and switch procedure in a patient with severe blepharoptosis with a high risk of corneal exposure.
This article was presented as a meeting abstract in the World Society of Ophthalmic Plastic Reconstructive & Aesthetic Surgery (WSOPRS) Meeting 2023 and as a video in the American Academy of Ophthalmology (AAO) Annual Meeting 2023.
Case presentation
A 65-year-old gentleman underwent bilateral muller muscle conjunctival resection, tarsectomy, and later bilateral levator resection for recurrent ptosis done elsewhere two years prior to presentation. He presented with bilateral recurrent ptosis (margin reflex distance 1 (MRD1) = 0 mm, MRD2 = 5 mm), poor levator function (5 mm), poor Bell’s phenomenon, and severe frontalis overaction (Figure 1A).
A: Right eye preoperative clinical photo. B: Right eye postoperative clinical photo.
Surgical technique
The surgical procedure was performed under local anesthesia through an eyelid crease skin incision. A sequential operative approach was adopted by anterior levator resection. The desired level of the anterior levator advancement was secured to the superior tarsal border, and intraoperative lid height and contour adjustments were done with the patient upright. The redundant levator aponeurosis (5-6 mm) was resected (Figure 2A) and transferred as a posterior lamellar spacer graft for the lower eyelid positioned between the inferior tarsal border and the recessed lower lid retractors (Figures 2B, 2C) to elevate the MRD2, thus keeping a stable palpebral fissure height (5 mm) (Figure 2D). The graft was then secured with 6-0 Vicryl (Figure 2E). Bandage contact lens and frost traction sutures were applied to the lower eyelid and placed on upward traction postoperatively (Figure 2F).
A: Redundant levator aponeurosis excision. B: Lower eyelid retractor recession. C: Repurposed aponeurosis as a lower-lid posterior lamellar graft. D: Fashioning the height of the resected levator aponeurosis. E: Suturing of aponeurosis to the inferior tarsal border. F: Frost sutures on the upward traction.
At three months postoperative, the left visual axis was unobstructed with MRD1 = 2 mm, MRD2 = 3 mm, and <1 mm lagophthalmos (Figure 1B).
Discussion
Several methods have been used to treat ptosis, namely, Müller’s muscle conjunctival resection tarsal resection, tarsal switch, levator advancement, and frontalis slings or flaps surgery. Each technique has its own advantages and sets of drawbacks.
The correction of ptosis often leaves the cornea exposed postoperatively. The tendency to undercorrect ptosis surgery is well justified, especially in the presence of suboptimal Bell’s phenomenon and preexisting dry eye disease, which may lead to eventual ptosis recurrence. We propose elevating MRD1 and MRD2 using the resected levator aponeurosis to provide a single solution for such a situation. The resulting correction provides an upward shift of the palpebral fissure height, freeing the visual axis while maintaining a stable palpebral fissure height, which safeguards the cornea from postoperative exposure. These outcomes allow the patient to resume daily activities with less discomfort, improve aesthetics, mitigate the risk of ocular damage, and improve their overall quality of life [6,7]. A literature review on tarsal switch surgery and their respective outcomes and adverse events are outlined in Table 1.
Previous tarsal switch techniques have been reported to increase the MRD1 while decreasing the MRD2 [8], and while it remains an effective means for correcting severe ptosis, it was associated with MGD due to the tarsal plate resection. Two published works on tarsal switches reported postoperative myopathic lagophthalmos as a recurring complication [5,8].
Conclusions
Corneal exposure and dry eye are common in patients with myopathic ptosis. The novel levator switch technique offers an effective alternative treatment to correct ptosis with both poor and normal levator muscle function, when Bell's phenomenon is absent or poor. This procedure minimizes the risk of corneal exposure and preserves the meibomian glands by sparing tarsal plate resection. However, further large-scale studies are required to definitively confirm its long-term efficacy.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Congenital and acquired blepharoptosis Curr Opin Ophthalmol Sakol PJ Mannor G Massaro BM 3353391019991062154810.1097/00055735-199910000-00010 · doi ↗ · pubmed ↗
- 2The mechanistic classification of ptosis Ophthalmology Frueh B 10191021871980701752410.1016/s 0161-6420(80)35135-x · doi ↗ · pubmed ↗
- 3The posterior approach tarsal switch procedure for myopathic ptosis: a modified technique Ophthalmic Plast Reconstr Surg Lenake MN Mc Nab AA 1291313320172701524210.1097/IOP.0000000000000673 · doi ↗ · pubmed ↗
- 4Levator resection for minimal ptosis: another simplified operation Arch Ophthalmol FARM SEJ 4934966519611369829310.1001/archopht.1961.01840020495005 · doi ↗ · pubmed ↗
- 5Tarsal switch levator resection for the treatment of blepharoptosis in patients with poor eye protective mechanisms Ophthalmology Demartelaere SL Blaydon SM Shore JW 2357236311320061715713910.1016/j.ophtha.2006.06.055 · doi ↗ · pubmed ↗
- 6Tarsal switch procedure for the surgical rehabilitation of the eyelid and socket deficiencies of the anophthalmic socket Ophthalmic Plast Reconstr Surg Massry GG Hornblass A Rubin P Holds JB 3333401519991051121310.1097/00002341-199909000-00006 · doi ↗ · pubmed ↗
- 7Tarsal switch levator for mitochondrial myogenic ptosis [Article in Portoguese]Arq Bras Oftalmol Lucci LM Fonseca Junior NL Sugano DM Silvério J 1591637220091946632110.1590/s 0004-27492009000200005 · doi ↗ · pubmed ↗
- 8Tarsal switch using an anterior approach to correct severe ptosis Arch Plast Surg Meneghim RL Ferraz LB Galindo-Ferreiro A Khandekar R Sanchez-Tocino H Schellini S 1651704520182956646710.5999/aps.2017.00465 PMC 5869425 · doi ↗ · pubmed ↗