Neuro-pediatric emergencies: clinical profile and outcomes
Imad Khojah, Osama Muthaffar, Hassan Alalawi, Anas Alyazidi, Maha Alghamdi, Ohud Alharbi, Latifa Almuharib, Mayar Alhuqaili

TL;DR
This study examines pediatric neurological emergencies in Saudi Arabia, focusing on demographics, reasons for visits, and outcomes.
Contribution
The study provides a detailed clinical profile of pediatric neurology cases in a Saudi ED, highlighting age-related variations.
Findings
Seizures and postictal states were the most common reasons for pediatric neurological ED visits.
Over a third of patients were triaged as 'resuscitation', indicating high severity.
Discharge was the most common outcome, with significant differences in presentation across age groups.
Abstract
Pediatric neurological emergencies are a significant concern, often leading to high rates of admission to pediatric intensive care units and increased mortality rates. In Saudi Arabia, the emergency department (ED) is the main entry point for most patients in the healthcare system. This study aimed to provide a comprehensive overview of pediatric neurology visits to the ED, analyzing patient demographics, clinical presentations, and outcomes. The retrospective study was conducted at a large tertiary care center and examined 960 pediatric patients with neurological emergencies out of 24,088 pediatric ED visits. The study population consisted mainly of male participants (56.5%) and 43.5% female participants, with a mean age of 5.29 ± 4.19 years. School-age children (6–12 years) represented the largest population group (29.1%), and over a third of patients were triaged as 'resuscitation'…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
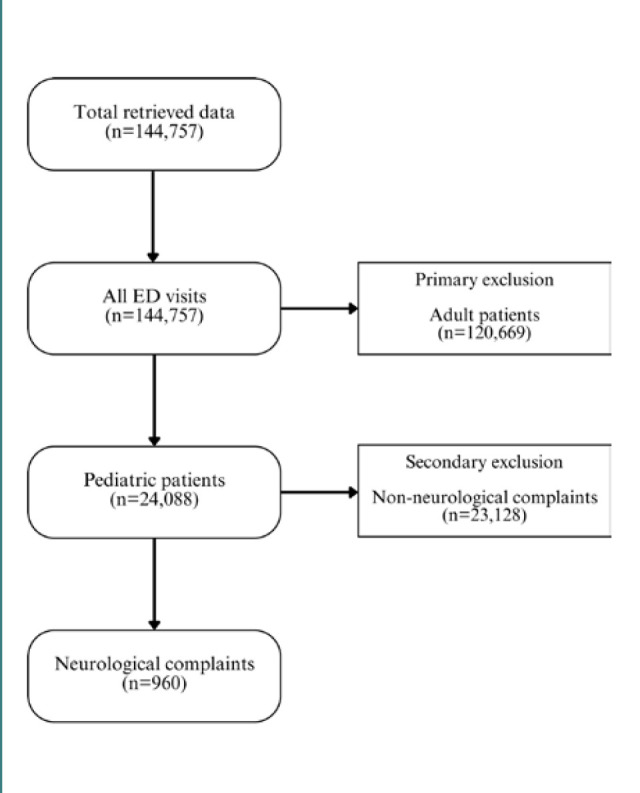 Figure 1
Figure 1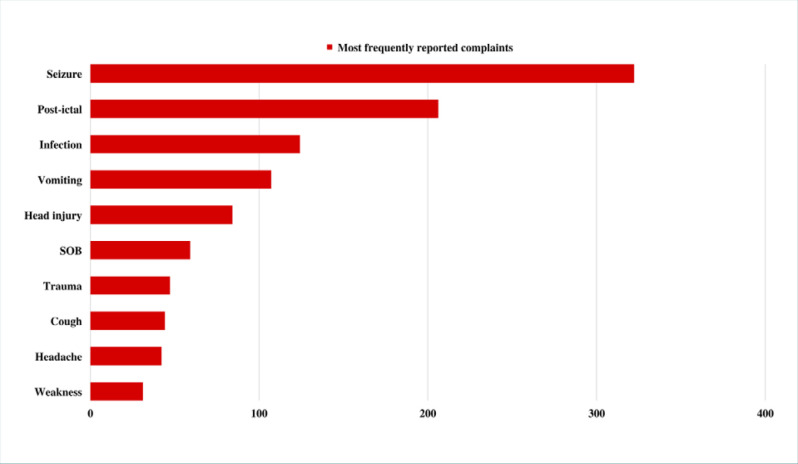 Figure 2
Figure 2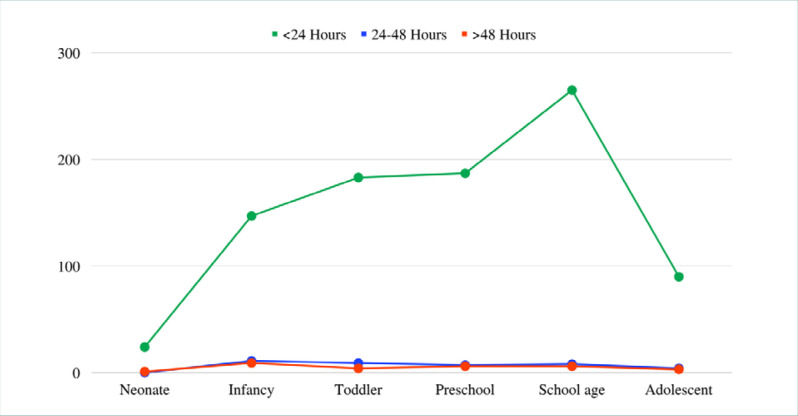 Figure 3
Figure 3| Characteristic | |
|---|---|
| Age, in years (mean ± SD) | 5.29 ± 4.19 |
|
| |
| Neonate (birth – 1 month) | 25 (2.6) |
| Infancy (1 month – 1 year) | 163 (17) |
| Toddler (1–3 years) | 196 (20.4) |
| Preschool (3–6 years) | 200 (20.8) |
| School-age (6–12 years) | 279 (29.1) |
| Adolescent (12–14 years) | 97 (10.1) |
|
| |
| Male | 542 (56.5) |
| Female | 418 (43.5) |
|
| |
| Saudi | 447 (46.6) |
| Non-Saudi | 513 (53.4) |
|
| |
| Priority 1 - Resuscitation | 332 (34.6) |
| Priority 2 - Emergent | 280 (29.2) |
| Priority 3 - Urgent | 331 (34.5) |
| Priority 4 - Less urgent | 11 (1.1) |
| Priority 5 - Non-urgent | 6 (0.6) |
|
| |
| Discharged | 558 (58.1) |
| Admitted | 394 (41.0) |
| AMA (against medical advice) | 4 (0.4) |
| LBT (left before treatment) | 3 (0.3) |
| Deceased (hospital death) | 1 (0.1) |
|
| |
| Seizure/Epilepsy | 529 (55.1) |
| Headache/Loss of consciousness | 23 (2.4) |
| Inflammation | 59 (6.1) |
| Cranial nerve palsy | 59 (6.1) |
| Neuromuscular | 14 (1.5) |
| Neoplasm | 55 (5.7) |
| Vascular | 92 (9.6) |
| Injury | 128 (13.3) |
| Abscess | 1 (0.1) |
|
| |
| Seizures | 317 (33.0) |
| Post-ictal | 187 (19.5) |
| Fever | 84 (8.8) |
| Head injury | 75 (7.8) |
| Shortness of breath | 35 (3.6) |
| Vomiting | 35 (3.6) |
| Trauma | 29 (3.0) |
| Headache | 26 (2.7) |
| Weakness | 23 (2.4) |
| Swelling | 20 (2.1) |
|
| |
| Less than 24 hours | 896 (93.3%) |
| 24-48 hours | 39 (4.1%) |
| More than 48 hours | 25 (2.6%) |
| Length of stay in hours (mean ± SD) | 10.56 ± 20.33 |
|
| |
| X-ray | 0.48 ± 0.94 |
| CT scan | 0.50 ± 0.77 |
| MRI | 0.05 ± 0.34 |
| Labs | 8.53 ± 6.39 |
| Medications | 3.19 ± 4.15 |
| Characteristic | Overall ( | Male ( | Female ( | |
|---|---|---|---|---|
| Age, in years (mean ± SD) | 5.29 ± 4.19 | 5.04 ± 3.90 | 5.60 ± 4.54 | 0.040 |
|
|
| |||
| Neonate (birth – 1 month) | 25 (2.6) | 14 (2.6) | 11 (2.6) | |
| Infant (1 month – 1 year) | 163 (17) | 87 (16.1) | 76 (18.2) | |
| Toddler (1-3 years) | 196 (20.4) | 122 (22.5) | 74 (17.7) | |
| Preschool (3-6 years) | 200 (20.8) | 110 (20.3) | 90 (21.5) | |
| School-age (6-12 years) | 279 (29.1) | 175 (32.3) | 104 (24.9) | |
| Adolescent (12-14 years) | 97 (10.1) | 34 (6.3) | 63 (15.1) | |
|
|
| |||
| Saudi | 447 (46.6) | 256 (47.2) | 191 (45.7) | |
| Non-Saudi | 513 (53.4) | 286 (52.8) | 227 (54.3) | |
|
|
| |||
| Priority 1 - Resuscitation | 332 (34.6) | 180 (33.2) | 152 (36.4) | |
| Priority 2 - Emergent | 280 (29.2) | 167 (30.8) | 113 (27.0) | |
| Priority 3 - Urgent | 331 (34.5) | 187 (34.5) | 144 (34.4) | |
| Priority 4 - Less urgent | 11 (1.1) | 5 (0.9) | 6 (1.4) | |
| Priority 5 - Non-urgent | 6 (0.6) | 3 (0.6) | 3 (0.7) | |
|
|
| |||
| Discharged | 558 (58.1) | 314 (57.9) | 244 (58.4) | |
| Admitted | 394 (41.0) | 222 (41.0) | 172 (41.1) | |
| AMA (against medical advice) | 4 (0.4) | 2 (0.4) | 2 (0.5) | |
| LBT (left before treatment) | 3 (0.3) | 3 (0.6) | 0 (0.0) | |
| Deceased (hospital death) | 1 (0.1) | 1 (0.2) | 0 (0.0) | |
|
|
| |||
| Seizure/Epilepsy | 529 (55.1) | 303 (55.9) | 226 (54.1) | |
| Headache/Loss of consciousness | 23 (2.4) | 17 (3.1) | 6 (1.4) | |
| Inflammation | 59 (6.1) | 31 (5.7) | 28 (6.7) | |
| Cranial nerve palsy | 59 (6.1) | 30 (5.5) | 29 (6.9) | |
| Neuromuscular | 14 (1.5) | 8 (1.5) | 6 (1.4) | |
| Neoplasm | 55 (5.7) | 26 (4.8) | 29 (6.9) | |
| Vascular | 92 (9.6) | 51 (9.4) | 41 (9.8) | |
| Injury | 128 (13.3) | 76 (14.0) | 52 (12.4) | |
| Abscess | 1 (0.1) | 0 (0.0) | 1 (0.2) | |
|
|
| |||
| Seizures | 317 (33.0) | 174 (32.1) | 143 (32.1) | |
| Post-ictal | 187 (19.5) | 118 (21.8) | 69 (16.5) | |
| Fever | 84 (8.8) | 54 (10.0) | 30 (7.2) | |
| Head injury | 75 (7.8) | 46 (8.5) | 19 (6.9) | |
| Shortness of breath | 35 (3.6) | 19 (3.5) | 16 (3.8) | |
| Vomiting | 35 (3.6) | 18 (3.3) | 17 (4.1) | |
| Trauma | 29 (3.0) | 15 (2.8) | 15 (3.3) | |
| Headache | 26 (2.7) | 14 (2.6) | 12 (2.9) | |
| Weakness | 23 (2.4) | 10 (1.8) | 13 (3.1) | |
| Swelling | 20 (2.1) | 9 (1.7) | 11 (2.6) | |
|
|
| |||
| Less than 24 hours | 896 (93.3%) | 499 (92.1) | 397 (95.0) | |
| 24–48 hours | 39 (4.1%) | 29 (5.4) | 10 (2.4) | |
| More than 48 hours | 25 (2.6%) | 14 (2.6) | 11 (2.6) | |
| Length of stay in hours | 10.56 ± 20.33 | 10.69 ± 21.93 | 10.39 ± 18.08 |
|
|
| ||||
| X-ray | 0.48 ± 0.94 | 0.46 ± 0.98 | 0.423 ± 0.88 | 0.589 |
| CT scan | 0.50 ± 0.77 | 0.51 ± 0.79 | 0.49 ± 0.74 | 0.744 |
| MRI | 0.05 ± 0.34 | 0.06 ± 0.37 | 0.03 ± 0.28 | 0.341 |
| Labs | 8.53 ± 6.39 | 8.33 ± 6.17 | 8.79 ± 6.67 | 0.267 |
| Medications | 3.19 ± 4.15 | 3.16 ± 4.15 | 3.23 ± 4.15 | 0.817 |
| Characteristic | Overall | Neonate (birth–1 month) | Infancy | Toddler (1–3 years) | Preschool (3–6 years) | School-age (6–12 years) | Adolescent (12–14 years) | |
|---|---|---|---|---|---|---|---|---|
| Age, in years | 5.29 ± 4.19 | 0.30 ± 0.031 | 0.54 ± 0.26 | 1.98 ± 0.61 | 4.46 ± 0.88 | 8.71 ± 1.60 | 13.15 ± 0.66 | 0.000 |
|
|
| |||||||
| Male | 542 (56.5) | 14 (56.0) | 87 (53.4) | 122 (62.2) | 110 (55.0) | 175 (62.7) | 34 (35.1) | |
| Female | 418 (43.5) | 11 (44.0) | 76 (46.6) | 74 (37.8) | 90 (45.0) | 104 (37.3) | 63 (64.9) | |
| Nationality | 0.000 | |||||||
| Saudi | 447 (46.6) | 7 (28.0) | 93 (57.1) | 106 (54.1) | 87 (43.5) | 120 (43.0) | 34 (35.1) | |
| Non-Saudi | 513 (53.4) | 18 (72.0) | 70 (42.9) | 90 (45.9) | 113 (56.5) | 159 (57.0) | 63 (64.9) | |
|
|
| |||||||
| Priority 1 - Resuscitation | 332 (34.6) | 4 (16.0) | 37 (22.7) | 66 (33.7) | 71 (35.5) | 102 (36.6) | 52 (53.6) | |
| Priority 2 - Emergent | 280 (29.2) | 18 (72.0) | 60 (36.8) | 50 (25.5) | 60 (30.0) | 75 (26.9) | 17 (17.5) | |
| Priority 3 - Urgent | 331 (34.5) | 3 (12.0) | 64 (39.3) | 76 (38.8) | 65 (32.5) | 96 (34.4) | 27 (27.8) | |
| Priority 4 - Less urgent | 11 (1.1) | 0 (0.0) | 2 (1.2) | 1 (0.5) | 4 (2.0) | 3 (1.1) | 1 (1.0) | |
| Priority 5 - Non-urgent | 6 (0.6) | 0 (0.0) | 0 (0.0) | 3 (1.5) | 0 (0.0) | 3 (1.1) | 0 (0.0) | |
|
|
| |||||||
| Discharged | 558 (58.1) | 1 (4.0) | 69 (42.3) | 112 (57.1) | 116 (58.0) | 184 (65.9) | 76 (78.4) | |
| Admitted | 394 (41.0) | 24 (96.0) | 93 (57.1) | 82 (41.8) | 82 (41.0) | 92 (33.0) | 21 (21.6) | |
| AMA (against medical advice) | 4 (0.4) | 0 (0.0) | 1 (0.6) | 2 (1.0) | 0 (0.0) | 1 (0.4) | 0 (0.0) | |
| LBT (left before treatment) | 3 (0.3) | 0 (0.0) | 0 (0.0) | 0 (0.0) | 2 (1.0) | 1 (0.4) | 0 (0.0) | |
| Deceased (hospital death) | 1 (0.1) | 0 (0.0) | 0 (0.0) | 0 (0.0) | 0 (0.0) | 1 (0.4) | 0 (0.0) | |
|
|
| |||||||
| Seizure/Epilepsy | 529 (55.1) | 10 (40.0) | 81 (49.7) | 101 (51.5) | 109 (54.5) | 160 (57.3) | 68 (70.1) | |
| Headache/Loss of consciousness | 23 (2.4) | 0 (0.0) | 4 (2.5) | 4 (2.0) | 4 (2.0) | 4 (1.4) | 7 (7.2) | |
| Inflammation | 59 (6.1) | 11 (44.0) | 20 (12.3) | 9 (4.6) | 8 (4.0) | 8 (2.9) | 3 (3.1) | |
| Cranial nerve palsy | 59 (6.1) | 0 (0.0) | 1 (0.6) | 8 (4.1) | 26 (13.0) | 18 (6.5) | 6 (6.2) | |
| Neuromuscular | 14 (1.5) | 0 (0.0) | 0 (0.0) | 6 (3.1) | 2 (1.0) | 4 (1.4) | 2 (2.1) | |
| Neoplasm | 55 (5.7) | 0 (0.0) | 0 (0.0) | 6 (3.1) | 7 (3.5) | 35 (12.5) | 7 (7.2) | |
| Vascular | 92 (9.6) | 4 (16.0) | 27 (16.6) | 22 (11.2) | 20 (10.0) | 17 (6.1) | 2 (2.1) | |
| Injury | 128 (13.3) | 0 (0.0) | 30 (23.4) | 40 (20.4) | 24 (12.0) | 32 (11.5) | 2 (2.1) | |
| Abscess | 1 (0.1) | 0 (0.0) | 0 (0.0) | 0 (0.0) | 0 (0.0) | 1 (0.4) | 0 (0.0) | |
|
|
| |||||||
| Seizures | 317 (33.0) | 4 (16.0) | 32 (19.6) | 61 (31.1) | 68 (34.0) | 101 (36.2) | 51 (52.6) | |
| Post-ictal | 187 (19.5) | 3 (12.0) | 46 (28.2) | 33 (16.8) | 39 (19.5) | 54 (19.4) | 12 (12.4) | |
| Fever | 84 (8.8) | 9 (36.0) | 20 (12.3) | 15 (7.7) | 12 (6.0) | 22 (7.9) | 6 (6.2) | |
| Head injury | 75 (7.8) | 0 (0.0) | 16 (9.8) | 27 (13.8) | 13 (6.5) | 16 (5.7) | 3 (3.1) | |
| Shortness of breath | 35 (3.6) | 3 (12.0) | 5 (3.1) | 8 (4.1) | 10 (5.0) | 7 (2.5) | 2 (2.1) | |
| Vomiting | 35 (3.6) | 0 (0.0) | 12 (7.4) | 6 (3.1) | 7 (3.5) | 10 (3.6) | 0 (0.0) | |
| Trauma | 29 (3.0) | 0 (0.0) | 7 (4.3) | 13 (6.6) | 8 (4.0) | 1 (0.4) | 0 (0.0) | |
| Headache | 26 (2.7) | 0 (0.0) | 0 (0.0) | 1 (0.5) | 7 (3.5) | 14 (5.0) | 4 (4.1) | |
| Weakness | 23 (2.4) | 0 (0.0) | 1 (0.6) | 4 (2.0) | 8 (4.0) | 7 (2.5) | 3 (3.1) | |
| Swelling | 20 (2.1) | 2 (8.0) | 13 (8.0) | 1 (0.5) | 2 (1.0) | 2 (0.7) | 0 (0.0) | |
|
|
| |||||||
| Less than 24 hours | 896 (93.3%) | 24 (96.0) | 147 (90.2) | 183 (93.4) | 187 (93.5) | 265 (95.0) | 90 (92.8) | |
| 24-48 hours | 39 (4.1%) | 0 (0.0) | 11 (6.7) | 9 (4.6) | 7 (3.5) | 8 (2.9) | 4 (4.1) | |
| More than 48 hours | 25 (2.6%) | 1 (4.0) | 5 (3.1) | 4 (2.0) | 6 (3.0) | 6 (2.2) | 3 (3.1) | |
| Length of stay in hours (mean ± SD) | 10.56 ± 20.33 | 14.97 ± 38.93 | 13.83 ± 35.84 | 8.74 ± 11.82 | 10.61 ± 17.03 | 9.71 ± 13.78 | 9.97 ± 10.83 | 0.185 |
|
| ||||||||
| X-ray | 0.48 ± 0.94 | 1.28 ± 1.21 | 0.58 ± 1.21 | 0.42 ± 0.79 | 0.46 ± 1.04 | 0.36 ± 0.78 | 0.27 ± 0.65 | 0.000 |
| CT scan | 0.50 ± 0.77 | 0.52 ± 0.87 | 0.54 ± 0.68 | 0.60 ± 0.84 | 0.54 ± 0.79 | 0.44 ± 0.77 | 0.33 ± 0.67 | 0.000 |
| MRI | 0.05 ± 0.34 | 0.04 ± 0.20 | 0.04 ± 0.19 | 0.05 ± 0.35 | 0.04 ± 0.33 | 0.07 ± 0.37 | 0.04 ± 0.41 | 0.954 |
| Labs | 8.53 ± 6.39 | 16.36 ± 7.24 | 9.49 ± 6.83 | 7.69 ± 6.06 | 8.31 ± 5.72 | 8.36 ± 6.70 | 7.57 ± 4.95 | 0.000 |
| Medications | 3.19 ± 4.15 | 6.48 ± 6.27 | 2.81 ± 3.57 | 2.79 ± 3.25 | 3.29 ± 4.88 | 3.07 ± 3.90 | 3.92 ± 4.64 | 0.000 |
| 95% Confidence interval | 95% Confidence interval | ||||||||
|---|---|---|---|---|---|---|---|---|---|
| Provisional diagnosis | Crude Odds ratio | Lower value | Upper value | Adjusted odds ratio | Lower value | Upper value | |||
| Neonate | Seizure/Epilepsy | 0.182 | 0.534 | 0.238 | 1.202 | 0.464 | 1.426 | 0.551 | 3.686 |
| Headache/Loss of consciousness* | 0.896 | 0.998 | |||||||
| Inflammation | 0.000 | 14.519 | 6.259 | 33.680 | 0.000 | 7.115 | 2.783 | 18.187 | |
| Cranial nerve palsy* | 0.382 | 0.997 | |||||||
| Neuromuscular* | 1.000 | 0.999 | |||||||
| Neoplasm* | 0.416 | 0.997 | |||||||
| Vascular | 0.447 | 1.833 | 0.615 | 5.461 | 0.628 | 0.752 | 0.238 | 2.380 | |
| Injury* | 0.091 | 0.996 | |||||||
| Abscess* | 1.000 | 1.000 | |||||||
| Infant | Seizure/Epilepsy | 0.150 | 0.770 | 0.549 | 1.078 | 0.284 | 1.242 | 0.835 | 1.847 |
| Headache/Loss of consciousness | 1.000 | 1.030 | 0.346 | 3.069 | 0.998 | 1.001 | 0.316 | 3.168 | |
| Inflammation | 0.001 | 2.718 | 1.541 | 4.797 | 0.089 | 1.712 | 0.921 | 3.185 | |
| Cranial nerve palsy | 0.002 | 0.079 | 0.011 | 0.572 | 0.006 | 0.062 | 0.008 | 0.459 | |
| Neuromuscular* | 0.178 | 0.999 | |||||||
| Neoplasm* | 0.001 | 0.997 | |||||||
| Vascular | 0.001 | 2.236 | 1.377 | 3.630 | 0.049 | 1.678 | 1.002 | 2.810 | |
| Injury | 0.050 | 1.609 | 1.027 | 2.521 | 0.021 | 1.808 | 1.094 | 2.988 | |
| Abscess* | 1.000 | 1.000 | |||||||
| Toddler | Seizure/Epilepsy | 0.295 | 0.835 | 0.609 | 1.143 | 0.152 | 0.755 | 0.514 | 1.109 |
| Headache/Loss of consciousness | 0.918 | 0.817 | 0.275 | 2.429 | 0.697 | 0.802 | 0.263 | 2.441 | |
| Inflammation | 0.396 | 0.687 | 0.332 | 1.423 | 0.289 | 0.660 | 0.306 | 1.423 | |
| Cranial nerve palsy | 0.237 | 0.595 | 0.278 | 1.275 | 0.191 | 0.596 | 0.274 | 1.294 | |
| Neuromuscular | 0.078 | 2.984 | 1.023 | 8.703 | 0.041 | 3.122 | 1.048 | 9.295 | |
| Neoplasm | 0.103 | 0.461 | 0.194 | 1.092 | 0.118 | 0.494 | 0.204 | 1.196 | |
| Vascular | 0.460 | 1.254 | 0.755 | 2.081 | 0.375 | 1.275 | 0.745 | 2.183 | |
| Injury | 0.002 | 1.970 | 1.304 | 2.975 | 0.001 | 2.171 | 1.370 | 3.441 | |
| Abscess* | 1.000 | 1.000 | |||||||
| Preschool | Seizure/Epilepsy | 0.910 | 0.970 | 0.709 | 1.326 | 0.849 | 0.964 | 0.659 | 1.409 |
| Headache/Loss of consciousness | 0.880 | 0.796 | 0.268 | 2.366 | 0.581 | 0.723 | 0.229 | 2.284 | |
| Inflammation | 0.210 | 0.579 | 0.270 | 1.241 | 0.128 | 0.537 | 0.241 | 1.197 | |
| Cranial nerve palsy | 0.000 | 3.292 | 1.918 | 4.886 | 0.000 | 3.479 | 1.990 | 6.082 | |
| Neuromuscular | 0.782 | 0.630 | 0.140 | 2.836 | 0.538 | 0.622 | 0.137 | 2.825 | |
| Neoplasm | 0.176 | 0.538 | 0.240 | 1.208 | 0.102 | 0.500 | 0.218 | 1.147 | |
| Vascular | 0.928 | 1.062 | 0.630 | 1.789 | 0.764 | 1.087 | 0.630 | 1.874 | |
| Injury | 0.612 | 0.860 | 0.535 | 1.382 | 0.547 | 0.854 | 0.512 | 1.426 | |
| Abscess* | 1.000 | 1.000 | |||||||
| School-age | Seizure/Epilepsy | 0.410 | 1.137 | 0.858 | 1.506 | 0.850 | 0.967 | 0.686 | 1.365 |
| Headache/Loss of consciousness | 0.310 | 0.507 | 0.171 | 1.503 | 0.150 | 0.442 | 0.145 | 1.343 | |
| Inflammation | 0.010 | 0.365 | 0.171 | 0.779 | 0.068 | 0.477 | 0.216 | 1.058 | |
| Cranial nerve palsy | 0.917 | 1.077 | 0.607 | 1.908 | 0.723 | 1.113 | 0.616 | 2.011 | |
| Neuromuscular | 1.000 | 0.976 | 0.304 | 3.138 | 0.823 | 1.144 | 0.351 | 3.732 | |
| Neoplasm | 0.000 | 4.741 | 2.685 | 8.372 | 0.000 | 7.785 | 4.183 | 14.488 | |
| Vascular | 0.026 | 0.524 | 0.304 | 0.905 | 0.078 | 0.599 | 0.339 | 1.059 | |
| Injury | 0.326 | 0.789 | 0.515 | 1.210 | 0.102 | 0.680 | 0.428 | 1.080 | |
| Abscess* | 0.645 | 1..000 | |||||||
| Adolescent | Seizure/Epilepsy | 0.002 | 2.045 | 1.298 | 3.222 | 0.306 | 1.347 | 0.761 | 2.386 |
| Headache/Loss of consciousness | 0.003 | 4.117 | 1.650 | 10.274 | 0.000 | 6.803 | 2.449 | 18.896 | |
| Inflammation | 0.272 | 0.460 | 0.141 | 1.498 | 0.924 | 0.939 | 0.261 | 3.382 | |
| Cranial nerve palsy | 1.000 | 1.008 | 0.421 | 2.409 | 0.717 | 1.188 | 0.468 | 3.014 | |
| Neuromuscular | 0.939 | 1.493 | 0.329 | 6.771 | 0.254 | 2.537 | 0.512 | 12.565 | |
| Neoplasm | 0.664 | 1.321 | 0.580 | 3.005 | 0.060 | 2.398 | 0.963 | 5.966 | |
| Vascular | 0.013 | 0.181 | 0.044 | 0.746 | 0.085 | 0.282 | 0.067 | 1.193 | |
| Injury | 0.001 | 0.123 | 0.030 | 0.506 | 0.003 | 0.113 | 0.027 | 0.478 | |
| Abscess | 1.000 | 1.000 | |||||||
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsCardiac Arrest and Resuscitation · Neonatal and fetal brain pathology · Emergency and Acute Care Studies
INTRODUCTION
Emergency departments (ED) are the primary point of contact for hospital care in many situations, including Saudi Arabia, where these serve as the main entry point to the healthcare system for most patients [1,2]. Moreover, despite the severity or complexity of the primary medical complaint, pediatric patients continue to receive care from the ED frequently. This often leads to overcrowding and prolonged waiting hours, which can impact the quality and quantity of care [3]. Among these pediatric ED visits, neurological emergencies represent a critical subset, encompassing severe and life-threatening conditions like epileptic conditions, stroke, central nervous system infections, and neurosurgical emergencies that require special attention and intensive care. Although these cases represent a small percentage of overall pediatric ED visits (2-15%) [4–6], they account for nearly three times the frequency of pediatric intensive care unit (PICU) admissions, with a mortality rate that can be up to 50% [7]. A progressive increase in ED visits is observable, especially among communities with chronic neurological diseases and among growing populations with greater risk factors and comorbidities [8]. Children with neurological emergencies present with a variety of symptoms when they arrive in the ED [9]. In coastal regions such as Jeddah, drowning can also be a significant contributor to both severe neurologic morbidity and accidental death [10]. Globally, demographic and clinical data regarding pediatric neuro-emergency visits vary among countries [4,11]. Specific data on pediatric neuro-emergencies in our local literature is extremely limited. Only a few reports assessed and explored the characteristics and clinical profile of certain disorders, such as status epilepticus, or were limited to a specific year period [12–15]. This study aimed to address this gap by providing a comprehensive overview of pediatric neurology visits to the ED in the local context. This research aims to inform strategies for maximizing care quality and improving healthcare staff training by analyzing patient demographics, clinical profiles, and outcomes. This comprehensive understanding is crucial for optimizing the management of pediatric neurological emergencies in the region.
MATERIAL AND METHODS
Study design and setting
This descriptive, retrospective cohort study adhered to the Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) checklist [16]. The study was conducted in a publicly operated tertiary care center that is funded and owned by the community and serves the entire community with a bed capacity of 750 beds and up to 900 beds in an emergency setting. The center receives an estimated 60,000 visits annually. The data for the emergency department record from 2019–2021 were retrieved directly from the hospital record to limit data entry errors. A total of 144,757 visits were retrieved; however, only pediatric patients were included in this study. Pediatric patients were defined as patients aged 14 years old or younger, all of whom were included. No other restrictions were applied at that stage. After including 24,088 pediatric patients, they were screened based on preliminary diagnosis (Figure 1). Patients with a neuro-related provisional diagnosis were included after identifying the clinical characteristics and assessing the severity of clinical presentation across multiple variables. The study aimed to correlate triage level with presentation severity and admission type. Finally, the large sample size contributed to the reliability of the study because every visit was included.
Flow chart of the inclusion criteria
Statistical analysis
The following variables were extracted: gender, age, nationality, provisional diagnosis, chief complaint, outcome, triage level, visit time, length of stay (LOS), date of admission, number of X-rays, magnetic resonance imaging (MRI), computerized tomography (CT), lab workups, and number of medications. Statistical analysis was performed using the Statistical Package for the Social Sciences (SPSS) version 26 (IBM Corp., Armonk, NY, USA) and SmartPLS 3 to test the relationship between the variables. Variables were distributed into qualitative and quantitative categories. Qualitative variables were described in frequency tables with percentages, and quantitative data were described with the mean and standard deviation (SD). The chi-square test was used to compare categorical variables. One-way analysis of variance (ANOVA) and multinomial logistic regression were used to predict the difference between demographic and clinical characteristics. All data utilized graphical presentation in the form of line charts and illustrated graphs. P values <0.05 were considered statistically significant.
RESULTS
Demographic and clinical characteristics
The study included 960 patients with a provisional neurological diagnosis. Table 1 describes patients' baseline characteristics. There were 542 (56.5%) male and 418 (43.5%) female patients. The average age of the patients was 5.29 ± 4.19 years, with the school-age group (6–12 years) being the most prevalent, comprising 279 (29.1%) of the total patients. Most patients were triaged as ‘priority 1: resuscitation’ (n = 332; 34.6%), followed by ‘priority 3: urgent’ (n = 331, 34.5%). Table 2 presents a comparison of various characteristics stratified by gender, while Table 3 provides a comparison based on different age groups.
Patients’ complaints
The most frequent chief complaint was seizures (n = 317, 33.0%) (Figure 2), followed by post-ictal state (n = 187, 19.5%). Most patients received a provisional diagnosis of seizures or epilepsy (n = 529, 55.1%). No statistically significant differences in provisional diagnosis or chief complaints were observed between genders (P = 0.454 and P = 0.346, respectively; Table 2). In contrast, there were statistically significant differences in provisional diagnosis and chief complaints when comparing different age groups (P >0.001 and P <0.001, respectively; Table 3). Table 4 presents a multinomial logistic regression comparing age groups to a specific provisional diagnosis.
Most commonly reported neurological complaints in pediatric patients
Patients’ outcomes
The most common outcome was discharge (n = 558, 58.1%), followed by admission (n = 394, 41.0%). The mean length of stay was 10.56 ± 20.33 hours (Figure 3), and most patients stayed for less than 24 hours (n = 896, 93.3%). No significant differences were found between gender and outcomes (P = 0.531) or length of stay (P = 0.826). Most male and female patients stayed less than 24 hours. However, outcomes varied significantly across age groups (P <0.001), while length of stay did not (P = 0.776, Table 3).
Average length of hospital stay by pediatric age group
DISCUSSION
The primary purpose of this study was to explore the current clinical and demographic characteristics of pediatric neuro-emergencies using hospital data from a tertiary care center. Nationwide, this study serves as the first of its kind to comprehensively review such characteristics. Our study included many age groups, from neonates to adolescents, with 960 patients, including 542 male and 418 female participants. The mean age of patients presenting to the ED in our study was 5.3 years, indicating that the majority of patients present at school age (n = 279). In comparison, the male group was larger than the female group. Moreover, seizure was the leading complaint, similar to the literature findings [9]. The majority of patients were triaged as ‘priority 1: resuscitation’ (34.6%). This is likely due to the study setting in a public tertiary care center, which receives many critically ill patients without major prerequisites. Our analysis of patient demographics revealed a significant impact of age on both treatment plans and provisional diagnosis (P = 0.000). This finding aligns with existing literature, emphasizing the unique characteristics and needs of different pediatric age groups [17]. Consistent with Kim et al. [18], our study found more visits from school-aged children compared to neonates. The admission rate was high in all age groups, particularly newborns requiring supervision and stabilization. This serves as important information, as some studies have reported inequalities in pediatric hospital admissions [19]. Moreover, the number of cases who left against medical advice was low across all age groups, potentially reflecting increased awareness among patients and families regarding the importance of medical care. Also, the most common provisional diagnosis across all groups was seizure, followed by injury and vascular injury. Seizures were more common between ages 3 and 12 and were the second most common in newborns, after inflammation. This supports other studies that concluded that seizures and headaches are the most frequent reasons for admitting pediatric patients presenting to ED with neuro-related complaints [4]. In Saudi Arabia, the prevalence of seizures increased over time, aligning with global trends and surpassing other neurological complaints. This increase is likely due to several risk factors present within the Saudi community, including a higher prevalence of genetic epilepsies due to high rates of consanguineous marriages [20–22]. This can explain the leading trend of seizure in our cohort in comparison to other neurological complaints. However, it is expected for seizures to be prevalent among ED neuro-related complaints, as they can affect 4–10% of the general pediatric population [23,24]. We observed a very low mortality rate of 0.1%, likely attributable to the nature of our non-trauma center where the study was conducted. Nevertheless, even in this setting, life-threatening diagnoses like neuromuscular disorders and neoplasms were observed, underscoring the importance and concern surrounding pediatric neurological emergencies. Cranial nerve palsy was more common in preschoolers than in neonates and infants, while headaches were rare in this age group. Other studies reported a mean age of cranial nerve injuries of 9 ± 6 years [25]. Furthermore, head injuries and neuromuscular injuries were more common in young children, according to preliminary diagnosis, and even between the ages of 1 month and 6 years. Of particular interest is that neoplasia was reasonably rare at young ages but common at school age. As seizures are common as a preliminary diagnosis, this was particularly worrying. Seizures and postictal states were the most common complaints across all age groups but less frequent in school-aged children. Fever was more prevalent in newborns and infants than in older children and adolescents. Infants also experienced head injuries more frequently, although previous studies suggest these injuries are typically benign [26]. As for the frequency of hospital stays, 896 of 960 visits were under 24 hours.
The retrospective study design could impact the results as the outcomes were assessed in a single center. We addressed this limitation by including a large and diverse sample, ensuring representative demographics. Additionally, electronic medical records facilitated access to high-quality data, enhancing the reliability of our findings. Other potential limitations include sample bias and the variability in participant demographics and numbers. Additionally, medication details and imaging protocols were unavailable for review. However, the large sample size and representative demographics help minimize the impact of these limitations on the overall conclusions of the study.
CONCLUSION
Pediatric neuro-emergencies continue to be a significant concern, contributing to mortality, morbidity, and increased hospital visits and lengths of stay. Variations were observed across different age groups, with consistent patterns emerging within each group, aligning with existing literature. Seizures remain a leading cause of admission compared to other neuro-related complaints. Specific groups demonstrated certain patterns, such as the prevalence of cranial nerve palsy among preschool patients. Expanding the current findings to analyze the characteristics and flow patterns would greatly benefit practitioners and researchers..
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Kayipmaz AE Demircan A Pandemic hospitals and reorganizing emergency departments Turk J Med Sci 202151 SI-13221322810.3906/sag-2106-16934284534 PMC 8771009 · doi ↗ · pubmed ↗
- 2Khattab E Sabbagh A Aljerian N Binsalleeh H Almulhim M Alqahtani A Emergency medicine in Saudi Arabia: a century of progress and a bright vision for the future Int J Emerg Med 20191211610.1186/s 12245-019-0232-031286863 PMC 6615245 · doi ↗ · pubmed ↗
- 3Kubicek K Liu D Beaudin C Supan J Weiss G Lu YA profile of nonurgent emergency department use in an urban pediatric hospital Pediatr Emerg Care 201228109778410.1097/PEC.0b 013e 31826 c 9aab 23023463 PMC 3464348 · doi ↗ · pubmed ↗
- 4Personnic J Titomanlio L Auvin S Dozières-Puyravel B Neurological disorders encountered in a pediatric emergency department Eur J Paediatr Neurol 202132869210.1016/j.ejpn.2021.03.01733862442 · doi ↗ · pubmed ↗
- 5Lewis DW Headache in the pediatric emergency department Semin Pediatr Neurol 200181465110.1053/spen.2001.2333111332866 · doi ↗ · pubmed ↗
- 6Alpern ER Stanley RM Gorelick MH Donaldson A Knight S Teach SJ Epidemiology of a pediatric emergency medicine research network: the PECARN Core Data Project Pediatr Emerg Care 200622106899910.1097/01.pec.0000236830.39194.c 017047467 · doi ↗ · pubmed ↗
- 7Kumar G Sharma V Kumar A Clinical Profile of Pediatric Neurology Disorders: A Study From a Semi-Urban Medical College in Northwestern India Cureus 20221410 e 3035910.7759/cureus.3035936407270 PMC 9665329 · doi ↗ · pubmed ↗
- 8Casado V Neurological patient care in emergency departments. A review of the current situation in Spain Neurologia 20112642338 English, Spanish 10.1016/j.nrl.2010.07.03321163207 · doi ↗ · pubmed ↗