Clinical characteristics and outcomes of overt gastrointestinal bleeding in children undergoing haploidentical hematopoietic stem cell transplantation: a single-center retrospective analysis
Shanshan Qi, Lannan Zhang, Zhi Chen, Zhuo Wang, Lili Ding, Yu Du, Hao Xiong

TL;DR
This study examines gastrointestinal bleeding in children after a specific type of stem cell transplant, finding it is common and linked to worse outcomes.
Contribution
The study identifies risk factors for overt gastrointestinal bleeding in pediatric haploidentical stem cell transplant recipients.
Findings
Overt gastrointestinal bleeding occurred in 25.2% of pediatric haplo-HSCT patients.
Grade III–IV gut aGvHD, TMA, and CMV viremia are significant risk factors for overt GIB.
Overt GIB is associated with reduced overall survival and increased non-relapse mortality.
Abstract
Overt gastrointestinal bleeding (GIB) is a potentially serious and life-threatening condition in patients undergoing allogeneic hematopoietic stem cell transplantation (allo-HSCT). However, relatively little information is available regarding overt GIB in children. To assess the prevalence, clinical patterns, and outcomes of overt GIB in children undergoing haploidentical hematopoietic stem cell transplantation (haplo-HSCT). A total of 123 consecutive patients with malignant or non-malignant blood disorders who received haplo-HSCT were reviewed in our hospital between October 2017 and October 2022. Overt GIB was determined as hematemesis, melena or hematochezia. Continuous variables were compared by Mann Whitney U test. Categorical parameters were compared by the χ2 test or Fisher’s exact test. Kaplan-Meier curves and log-rank tests were used to assess overall survival (OS),…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
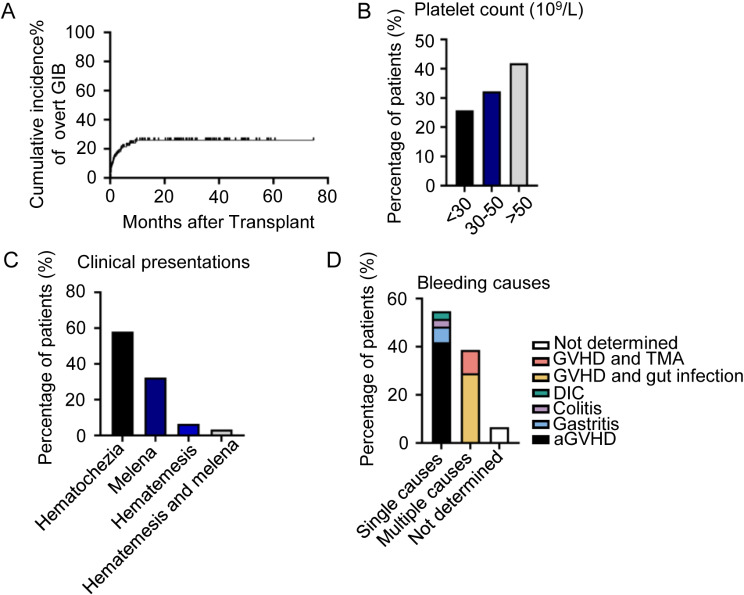 Figure 1
Figure 1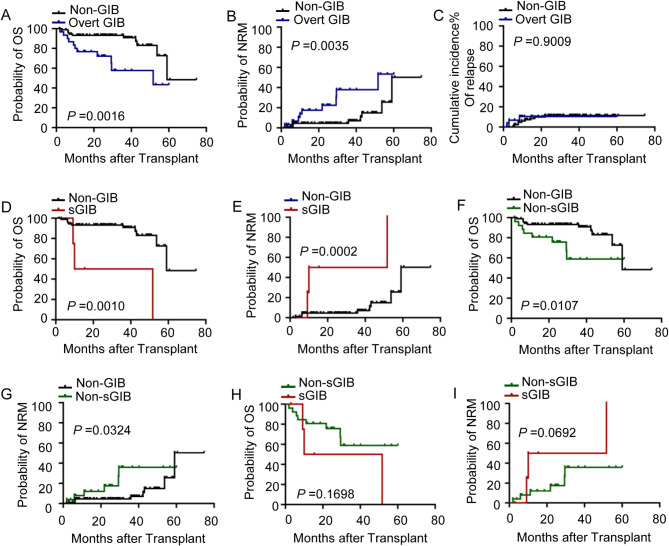 Figure 2
Figure 2- —Research Program on Applied Fundamentals and Frontier Technologies of Wuhan
- —Foundation Program of Wuhan Children’s Hospital
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsHematopoietic Stem Cell Transplantation · Immune Cell Function and Interaction · Platelet Disorders and Treatments
Introduction
Allogeneic hematopoietic stem cell transplantation (allo-HSCT) has been increasingly used to treat a wide range of malignant and non-malignant disorders in children [1–3]. However, its use has been limited by a lack of human leukocyte antigen (HLA)-matched donors. Only 50% of children who require an allo-HSCT will have an HLA-matched donor, and this percentage falls to less than 20% for some ethnic minority populations [4–6]. For patients without an HLA-matched donor, haploidentical hematopoietic stem cell transplantation (haplo-HSCT) is therefore an important alternative option [7, 8]. Along with the wide use of anti-thymocyte globulin (ATG)-based or post-transplant cyclophosphamide (PTCy)-based regimens, haplo-HSCT is feasible and achieves good results for a range of hematological diseases [9, 10].
With the extended application of haplo-HSCT, a variety of complications have become increasingly recognized. Gastrointestinal disorders are common after HSCT and usually caused by chemotherapeutic drugs, opportunistic infections, acute graft-versus-host disease (aGvHD) or coagulation abnormalities [11–13]. Gastrointestinal bleeding (GIB) is one of the most common manifestations of gastrointestinal disorders and is associated with significant mortality [14, 15]. However, the majority of literature on HSCT-associated GIB studies describe adult patients [16, 17], with relatively little information available for pediatric GIB, especially in a haplo-HSCT population.
Herein, we reviewed the incidence, causes, clinical features, outcomes, and risk factors for GIB in pediatric patients receiving haplo-HSCT in a single unit.
Methods
Patients
We retrospectively reviewed the medical records of patients received haplo-HSCT at Wuhan Children’s Hospital between October 2017 to October 2022. Overall, 123 patients underwent haplo-HSCT. Based on medical records, 31 patients were diagnosed with overt GIB. This study was approved by the Medical Ethics Committee of Wuhan Children’s Hospital, Tongji Medical College, Huazhong University of Science and Technology.
Preparative regimens, GvHD prophylaxis and stem cell sources
For patients diagnosed with acute myeloid leukemia or myelodysplastic syndromes who underwent haplo-HSCT, the conditioning regimens included cyclophosphamide (10 mg/kg/day on days − 8 and − 7), intravenous fludarabine (30 mg/m^2^/day from day − 6 to day − 2), oral semustine (250 mg/m^2^ on day − 6), and intravenous busulfan (1.1 mg/kg/day from day − 5 to day − 2). PTCy-based prophylactic regimens were used for GvHD prophylaxis. Cyclosporine, rabbit ATG, rituximab, mycophenolate mofetil and cyclosporine A were included. As described recently [18], donor lymphocyte infusion (DLI) was given depending on the clinical status.
For patients with acute lymphocytic leukemia, the conditioning regimens included total marrow irradiation (4 Gy/d on day − 10 and day − 9), etoposide (20 mg/kg/d on day − 6 and − 5), rabbit ATG (10 mg/kg from day − 4 to day − 2) and cyclophosphamide (60 mg/kg/d on day − 3 and − 2). For non-malignant disorders in our study, the conditioning regimens included cyclophosphamide (120 mg/kg from day − 8 to day − 7), intravenous fludarabine (40 mg/m^2^/day from day − 6 to day − 3), intravenous busulfan (1.1 mg/kg/day on day − 6 and day − 5) and rabbit ATG (10 mg/kg from day − 4 to day − 2). GvHD prophylaxis consisted of mycophenolate mofetil, short-term methotrexate and cyclosporine.
Acute GVHD (aGvHD) and chronic GVHD (cGvHD) were diagnosed and graded according to the established guidelines and criteria [19, 20]. Patients were evaluated for aGVHD occurring within 100 days after DLI.
All the patients received granulocyte colony-stimulating factor modified peripheral blood stem cell transplantation grafts.
Definitions
In terms of clinical outcomes, overall survival (OS) was defined as the interval from HSCT to death irrespective of disease state. Non-relapse mortality (NRM) was defined as death without previous relapse. Cytomegalovirus (CMV) viremia was defined as serum CMV-DNA was more than 1000 copies/mL. Diagnosis of intestinal infections was made based on gastrointestinal symptoms and laboratory examination results. Overt GIB was defined as the presence of hematemesis, melena or hematochezia. Severe GIB was defined as either (1) overt GIB resulting in hemorrhagic shock or (2) overt GIB leading to a decrease in hemoglobin of ≥ 2 g/dL or at least a 20% fall in hematocrit, and transfusion at least two units of packed red blood cells.
Attribution of GIB causes
The cause of GIB was determined by clinical review of endoscopic, histological and microbiological data. Gut GvHD was recognized as the sole cause of bleeding when the clinical and histological appearances were typical, and cultures or immunohistochemistry stains for viruses and fungi were negative. When there was evidence of gut GvHD and infection, both were regarded as the causes of bleeding [16, 21].
Other causes of bleeding, such as gastritis and ulcers, were based on clinical and endoscopic criteria.
Statistical analysis
Continuous variables in our study were presented as medians (ranges) and were compared using the Mann–Whitney test. Categorical variables were compared using Pearson’s Chi-square test or Fisher’s exact test. Logistic regression was used to examine correlations. OS, NRM and relapse were assessed by the Kaplan–Meier method and compared using the log-rank test. P-values < 0.05 were considered to be significant. Data were analyzed using R software, version 4.1.0. and Prism version 8.4.3.
Results
Baseline patient characteristics
Overt GIB occurred in 31 out of 123 patients after haplo-HSCT, giving an incidence of 25.2%. The baseline characteristics of the two groups are shown in Table 1. More patients with GIB experienced grade III-IV gut aGvHD, thrombotic microangiopathy (TMA), intestinal infection and cytomegalovirus (CMV) viremia than patients in the control group. There were no differences between the two groups in the distribution of age, gender, underlying diseases, HLA mismatching, blood type compatibility, donor-recipient sex mismatching, engraftment time, preparative regimens, GvHD prophylaxis and CMV DNA.
Table 1. Baseline characteristics in patients with overt GIB and matched controls after haplo-HSCTVariablesOvert GIB(n = 31)Non-GIB(n = 92)P valueAge at HSCT, yr (range)5.5 (0.8–16.2)5.8 (0.2–16.9)0.7664Gender (n, %) Male16 (51.6%)53 (57.6%)0.561 Female15 (48.4%)39 (42.4%)Median follow-up time after HSCT, m (range)22.5 (1.9–60.1)29.5 (1.7–74.8)0.2808Underlying disease, n (%)0.445 Aplastic anemia6 (19.4%)29 (31.5%) Acute myeloid leukemia14 (45.2%)32 (34.8%) Acute lymphoblastic leukemia2 (6.5%)11 (12.0%) Myelodysplastic syndromes5 (16.1%)8 (8.7%) Others4 (12.9%)12 (13.0%)Conditioning, n (%)0.182 CTX/Flu/Me-CCNU/Bu1939 CTX/Flu/Bu/ATG1042 TMI/VP-16/ATG/CTX211GvHD prophylaxis, n (%)0.068 PTCy-based regimens1939 ATG-based regimens1253ABO mismatch, n (%)17 (54.8%)49 (53.3%)0.713Donor-recipient sex mismatch, n (%)17 (54.8%)45 (48.9%)0.568Human leukocyte antigen, n (%) 5/1016 (51.6%)38 (41.3%)0.722 6/106 (19.4%)29 (31.5%) 7/105 (16.1%)12 (13.0%) 8/102 (6.5%)7 (7.6%) 9/102 (6.5%)6 (6.5%)MNC (×10^8^/kg, range)18.9 (7.60–35.72)16.12 (4.69–35.00)0.2409CD34^+^ (×10^6^/kg, range)11.42 (4.0–24.0)10.06 (3.34–21.98)0.2175Engraftment time, d (range) Neutrophil15 (11–35)14 (10–73)0.0933 Platelet16 (8–26)15 (10–40)0.322Gut aGvHD, n (%)< 0.0001 06 (19.4%)51 (54.4%) I–II14 (45.2%)34 (37.0%) III–IV11 (35.5%)7 (7.6%)< 0.0001Extensive cGvHD, n (%)5 (16.1%)10 (10.9%)0.439Sinusoidal obstruction syndrome4 (12.9%)6 (6.5%)0.269Thrombotic microangiopathy7 (22.6%)4 (4.3%)0.005Disseminated intravascular coagulation1 (3.2%)2 (2.2%)0.743Acute kidney injury1 (3.2%)4 (4.3%)0.784Hemorrhagic cystitis10 (32.3%)21 (22.8%)0.296Intestinal infection9 (29.0%)8 (8.7%)0.005CMV viremia24 (77.4%)39 (42.4%)0.001CMV DNA (×10^3^copies/mL)7.19 (1.28–489.0)3.11 (1.11–38.5)0.191Notes* *, Fanconi anemia, Hemophagocytic syndrome, Thalassemia, Wiskott-Aldrich syndrome, Severe combined immunodeficiency; aGvHD, acute graft versus host disease; ATG, anti-thymocyte globulin; Bu, busulfan; cGvHD, chronic graft versus host disease; CMV, cytomegalovirus; CTX, cyclophosphamide; GIB, gastrointestinal bleeding; Flu, fludarabine; HSCT, allogeneic hematopoietic stem cell transplantation; Me-CCNU, semustine; MNC, mononuclear cell; PTCy, posttransplant cyclophosphamide; TMI, total marrow irradiation; VP-16, etoposide
GIB after haplo-HSCT
The median time after haplo-HSCT for the overt GIB event to occur was 376 days (range, 58 − 1,275 days) (Fig. 1.A and Supplemental Fig. 1.A). A total of 18 (18/31, 58.1%) patients had thrombocytopenia (platelet count < 50 × 10^9^/L) before GIB (Fig. 1.B), and 3 (3/31, 9.7%) patients required transfer to the medical intensive care unit for closer monitoring and management. The clinical presentations during GIB were variable. Of the 31 patients, 18 patients had hematochezia (58.1%), 10 patients had melena (32.3%), 2 patients had hematemesis (6.4%), and 1 patient (3.2%) presented with both hematemesis and melena (Fig. 1.C). The causes of GIB were diverse, with the most common single cause of bleeding being gut aGvHD (13/31, 41.9%), followed by gastritis (2/31, 6.5%), colitis (1/31, 3.2%) and disseminated intravascular coagulation (DIC, 1/31, 3.2%). Multiple bleeding causes were found in 12 patients (12/31, 38.7%): gut GvHD (8 aGvHD and one moderate cGvHD) and gut infection both contributed to the occurrence of GIB in 9 patients (9/31, 29%), and 3 patients bled due to gut aGvHD and TMA (3/31, 9.7%). The causes of bleeding were not determined in two patients (2/31, 6.5%) (Fig. 1.D). The grade and treatment of GvHD were shown in Supplemental Fig. 1.B and C.
Fig. 1. Characteristics of patients with overt GIB. (A) Incidence of GIB after haplo-HSCT. (B) Proportion of GIB patients with different platelet counts. (C) Proportion of GIB patients with different clinical presentations. (D) Proportion of GIB patients with different bleeding causes. aGVHD, acute graft versus host disease; DIC, disseminated intravascular coagulation; GIB, gastrointestinal bleeding; TMA, thrombotic microangiopathy
Severe GIB after haplo-HSCT
Among patients with overt GIB, five patients (5/31, 16.1%) experienced severe GIB and presented with hematochezia (Table 2). For severe GIB, two cases were patients with aplastic anemia, two patients had acute myeloid leukemia, and one patient had myelodysplastic syndromes. All of the patients with severe GIB had thrombocytopenia. Two of these five patients died during the hospitalization for severe GIB, with causes of death recorded as DIC and TMA, respectively. No deaths were directly attributable to the GIB.
Table 2. Characteristics of patients with severe GIBCaseSexAge(yr)Underlying diseaseDonorABOmismatchHLAOccurrence time after HSCT(d)Platelet count(10^9^/L)GvHD GradeIntestinal infectionand pathogensCMV viremiaOutcomesCauses of death1Male6.0Aplastic anemiaFatherYes5/103712IIaGVHDNoNoAlive/2Male15.6Aplastic anemiaMotherNo5/102797ModeratecGVHDYes/CMVYesDeathTMA3Male1.6Acute myeloid leukemiaFatherYes5/102633IIIaGVHDYes/Clostridium difficileYesAlive/4Female15.0Acute myeloid leukemiaMotherYes5/1029436IVaGVHDNoYesDeathDIC5Female5.5Myelodysplastic syndromesFatherYes7/101823IVaGVHDYes/Enteropathogenic Escherichia coliYesAlive/Notes aGVHD, acute graft versus host disease; CMV, cytomegalovirus; cGVHD, chronic graft versus host disease; DIC, disseminated intravascular coagulation; TMA, thrombotic microangiopathy;: Occurring within 100 days after donor lymphocyte infusion
Outcomes
The median follow-up period was 26.3 months (range, 1.7–74.8 months). The OS of patients with GIB were significantly reduced (P = 0.0016, Fig. 2.A), and the NRM was higher in these patients than in those without GIB (P = 0.0035, Fig. 2.B). There was no significant difference in the cumulative incidence of relapse between patients with GIB and the control group (P = 0.9009, Fig. 2.C). In subgroup analyses, it was observed that both severe GIB and non-severe GIB patients had significantly inferior OS (both P < 0.05, Fig. 2.D and F) and higher NRM (both P < 0.05, Fig. 2.E and G) when compared with non-GIB patients. However, OS and NRM showed no difference between patients with severe GIB and non-severe GIB (both P > 0.05, Fig. 2.H and I).
Fig. 2. Clinical outcomes of patients with overt GIB after haplo-HSCT. A-C. Overall survival (A), non-relapse mortality (B) and incidence of relapse (C) for patients with or without GIB after haplo-HSCT. D-E. The impact of severe GIB on overall survival (D) and non-relapse mortality (E) after haplo-HSCT. F-G. The impact of non-severe GIB on overall survival (F) and non-relapse mortality (G) after haplo-HSCT. H-I. Comparison of overall survival (H) and non-relapse mortality (I) of patients with severe GIB and non-severe GIB. GIB, gastrointestinal bleeding; NRM, non-relapse mortality; OS, overall survival
Predictors for the occurrence of GIB
Patients with overt GIB had significantly higher cumulative incidences of III-IV gut aGvHD, TMA, CMV viremia and intestinal infection than those without GIB (Supplemental Fig. 2.A-D). To further identify the variables capable of predicting GIB after haplo-HSCT, univariate and multivariate analyses were carried out (Table 3). grade III-IV gut aGvHD, TMA, CMV viremia and intestinal infection were significantly related to the occurrence of GIB in the univariate analysis. In the multivariate analysis, grade III-IV gut aGvHD, TMA and CMV viremia retained their association with GIB.
Table 3. Risk factors for overt GIB after haplo-HSCTVariablesUnivariateMultivariateHR95%P valueHR95%P valueAge > 5.5 yr1.110.49–2.510.795Male0.7850.347–1.7760.561ABO mismatch0.930.41–2.120.879Donor-recipient sex mismatch0.780.34–1.780.569Acute kidney injury1.360.14–12.680.785Disseminated intravascular coagulation0.660.058–7.610.744Hemorrhagic cystitis0.620.25–1.520.298Sinusoidal obstruction syndrome0.470.12–1.790.270cGVHD0.5850.225–2.2210.552Grade III–IV gut aGvHD17.501.95–156.490.01019.211.78–207.790.015Thrombotic microangiopathy6.411.73–2.380.0054.241.01–17.760.048CMV viremia4.451.74–11.380.0024.251.38–10.740.010Intestinal infection3.651.23–10.780.0191.990.56–7.030.284Notes* aGVHD, acute graft versus host disease; CMV, cytomegalovirus; cGVHD, chronic graft versus host disease; *: the median age of overt GIB patients
Discussion
GIB in children can lead to substantial morbidity and mortality, especially in cases of severe GIB [14, 22, 23]. As haplo-HSCT is being used with increasing frequency for pediatric patients [24–26], systematic investigations of GIB are needed.
The published prevalence of overt GIB ranges from 5.9 to 39%, and severe GIB can constitute between 11.8% and 54.3% [14, 16, 27, 28]. In our study, our results indicated that overt GIB is a frequent complication in pediatric patients after haplo-HSCT (incidence of 25.2%). Fortunately, we found that 90.3% (28/31) of incidences of GIB in our study were either self-limited or controllable with supportive care only. Only 3 out of 31 (9.7%) patients experienced significant hemorrhage and required monitoring and management in an intensive care unit. While some studies have demonstrated that the severity of bleeding affects patient survival [16, 21], our results indicated that OS and NRM were not different between children with severe GIB and those with non-severe GIB.
There are reports that more than half of cases of intestinal bleeding occur within 100 days after transplantation [21, 27]. However, the timespan of GIB onset was relatively broad in our study, with GIB events occurring early after HSCT or more than a year after. Significantly, one case of bleeding was observed at 1275 days following HSCT, with the underlying etiology identified as colitis. However, we are uncertain whether the patient’s colitis is a complication of transplantation. In our study, single cause bleeding accounted for the majority followed by multifactorial bleeding (38.7%). Among these multiple bleeding causes, intestinal infection was second only to aGvHD. 5 kinds of pathogens were detected, including CMV (3 cases), norovirus (2 case), clostridium difficile (2 cases), salmonella (one case) and enteropathogenic Escherichia coli (one case).
In recent years, studies have revealed risk factors for hemorrhagic complications after HSCT, including severe thrombocytopenia, grade III–IV aGvHD, and TMA [14, 17, 28]. In addition, sinusoidal obstruction syndrome, acute kidney injury and viral hepatitis have been identified as causing an increased risk of GIB [16]. Similarly, we found grade III–IV aGvHD and TMA were independent risk factors for pediatric GIB following haplo-HSCT. We did not observe any cases of concurrent viral hepatitis and GIB, but CMV viremia was identified as an independent risk factor. At our center, the management of severe thrombocytopenia was timely, and therefore low platelet counts were not included in our risk analysis. In addition, we found that acute kidney injury and sinusoidal obstruction syndrome were not correlated with GIB after haplo-HSCT, potentially explained by the low number of events. In fact, GIB is one of the most common manifestations of GvHD. Since, GvHD not only directly induces the injury of gastrointestinal epithelium but also associated with CMV reactivation [29] and TMA [30].
Limitations of this study were the relatively small sample size and the retrospective design without a comparative group, which might be accompanied by some biases. Nevertheless, to the best of our knowledge, this is the first study to provide data regarding pediatric GIB after haplo-HSCT.
To conclude, our study shows that both severe and non-severe GIB after haplo-HSCT could decrease the OS and increase the NRM of pediatric patients. Furthermore, grade III–IV gut aGvHD, TMA and CMV viremia are risk factors for its development. In future research, prospective controlled trials and multicenter studies to understand the causes and optimal management of pediatric GIB will be essential.
Electronic supplementary material
Below is the link to the electronic supplementary material.
Supplementary Material 1
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Przepiorka D, Weisdorf D, Martin P et al. 1994 Consensus Conference on Acute GVHD Grading. Bone marrow transplantation 1995;15(6):825–828.7581076 · pubmed ↗
- 2Srinivasan A, Raffa E, Wall DA et al. Outcome of Haploidentical Peripheral Blood Allografts Using Post-Transplantation Cyclophosphamide Compared to Matched Sibling and Unrelated Donor Bone Marrow Allografts in Pediatric Patients with Hematologic Malignancies: A Single-Center Analysis. Transplantation and cellular therapy 2022;28(3):158.e 151-158.e 159.10.1016/j.jtct.2021.11.00934838785 · doi ↗ · pubmed ↗