Giant left atrium in a patient with Marfan syndrome
Felipe Israel López-Trejo, Elias Noel Andrade-Cuellar, Edil Rosalio Argueta Machado

Abstract
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
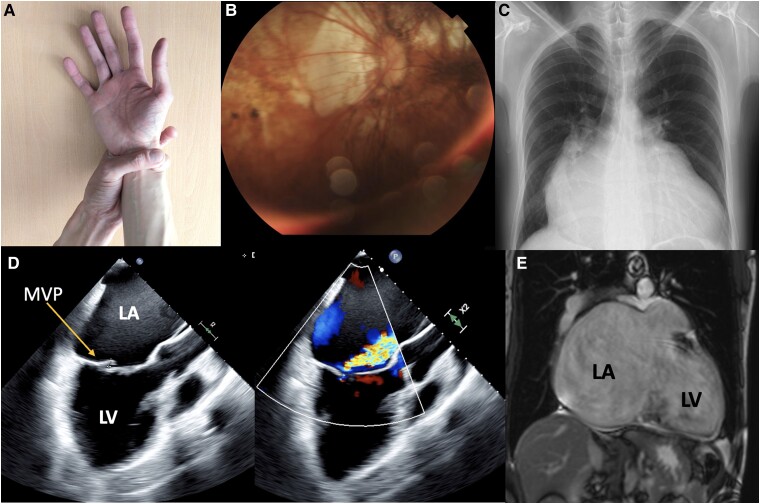 Figure 1
Figure 1Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsCardiomyopathy and Myosin Studies · Cardiovascular Function and Risk Factors · Connective tissue disorders research
A 41-year-old man with Marfan syndrome, complicated by retinal detachment, heart failure with mildly reduced ejection fraction, and atrial fibrillation for 1 year, presented to the cardiology clinic due to worsening dyspnoea. He had no significant family history. On physical examination, vital signs were normal. He had an ectomorphic, dolichocephalic physique with no jugular venous distension. Heart auscultation revealed irregular heart sounds and a mesosystolic murmur at the mitral focus. The Walker–Murdoch wrist sign was positive. Laboratory analysis showed no abnormalities. The electrocardiogram indicated atrial fibrillation and left ventricular hypertrophy. Coronary angiography revealed slow coronary flow. The trans-oesophageal echocardiogram showed left atrial dilation with an anteroposterior diameter of 81.8 mm, volume of 793 mL, and volume index of 425 mL/m^2^. Additionally, there was posterior leaflet prolapse of the mitral valve resulting in severe regurgitation classified as Carpentier type IIA. Magnetic resonance imaging (MRI) measurements showed the left atrium measured 113 × 83 mm, with an area of 122.2 cm^2^ (Figure 1 and Supplementary material).
Due to a decline in functional status attributed to severe mitral regurgitation, the case was reviewed by the heart team, who approved mitral valve replacement surgery. Currently, the patient is classified as New York Heart Association (NYHA) functional class II, with the heart rate controlled by a beta-blocker. The incidence of a giant left atrium is 0.3–0.6%, predominantly secondary to rheumatic mitral disease in up to 92% of cases, with non-rheumatic aetiologies being rare.^1^ A retrospective study associated Marfan syndrome with left atrial dilation, suggesting primary atrial involvement in this syndrome.^2^
Supplementary Material
ytae350_Supplementary_Data
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Ernst L , Zhang K, E Pieske-Kraigher, Pieske B, Heinzel FR, Gehle P. Morphological and secretory dysfunction of left atrium in Marfan syndrome. Eur Heart J 2021;42(Supplement_1):ehab 724–1863.
- 2Zhang K , Ernst L, Schobert I, Philipp K, Böning G, Heinzel FR, et al Is Marfan Syndrome associated with primary structural changes in the left atrium? Diagnostics (Basel) 2023;13:3278.37892098 10.3390/diagnostics 13203278 PMC 10606247 · doi ↗ · pubmed ↗